

Abstract
Objective
To describe the models of practice used by nurse practitioners (NPs) and FPs in community health centres (CHCs), and to examine the roles of NPs and FPs in these models.
Design
Cross-sectional study using an organizational survey completed by managers of the CHC sites, as well as administrative data on patient sociodemographic characteristics and encounter activities.
Setting
A total of 21 CHCs (13 main sites and 8 satellite sites) operating in eastern Ontario during the period from December 1, 2006, to November 30, 2008.
Participants
A total of 44 849 patients, 53 full-time equivalent FPs, and 41 full-time equivalent NPs.
Main outcome measures
Family physicians’ and NPs’ models of practice, the sociodemographic characteristics and medical profiles of patients who were treated in each model of practice, and FPs’ and NPs’ use of time.
Results
Patients were attributed to 1 of 3 models of practice in CHCs based on the proportion of visits to FPs and NPs: FP care (53% of patients), NP care (29%), and shared care (18%). Patients who received care in the NP model of practice were younger and more likely to be female, be homeless, and not have postsecondary education. Patients who received care in the FP model of practice had more complex medical conditions (cardiovascular disease, mental illness, lung disease, and diabetes) and more annual visits. Patients who received care in the shared care model had intermediate profiles. Nurse practitioners performed more off-site care and walk-in visits. Family physicians and NPs spent a similar proportion of time performing various duties such as direct clinical care and administration tasks.
Conclusion
Although NPs mainly cared for their own patient panels (in the NP care model), they did share some patients with FPs and provide some care to patients under the FP model of practice. Patients who were cared for by FPs and NPs had quite different characteristics.
Résumé
Objectif
Décrire les modes de pratique propres aux infirmières praticiennes (IP) et aux MF dans les centres de santé communautaires (CSC) et vérifier les rôles respectifs des MF et des IP dans ces modèles de pratique.
Type d’étude
Étude transversale à l’aide d’une enquête organisationnelle complétée par les gestionnaires des CSC, à l’aide des données administratives sur les caractéristiques sociodémographiques des patients et sur les activités de contact.
Contexte
Un total de 21 CSC (23 sites principaux et 8 sites satellites) opérant dans l’est de l’Ontario entre le 1er décembre 2006 et le 30 novembre 2008.
Participants
Un total de 44 849 patients, 53 MF équivalents temps plein et 41 IP équivalents temps plein.
Principaux paramètres à l’étude
Les modèles de pratique des MF et des IP, les caractéristiques sociodémographiques et les profils médicaux des patients traités selon chacun des modèles de pratique et l’emploi du temps des MF et des IP.
Résultats
Les patients ont été répartis dans un des 3 modèles de pratique utilisés dans les CSC en fonction de la proportion de leurs rencontres avec des MF ou des IP : rencontres avec des MF (53 % des patients), avec des IP (29 %) et avec les deux (18 %). Les patients soignés dans le modèle de pratique des IP étaient plus jeunes et plus susceptibles d’être des femmes, d’être sans domicile fixe et d’avoir une scolarité ne dépassant pas le secondaire. Les patients traités dans le modèle de pratique des MF avaient des conditions médicales plus complexes (diabète, maladie cardiovasculaire ou pulmonaire et problèmes de santé mentale) et plus de visites annuelles. Les patients du modèle des soins partagés avaient des profils intermédiaires. Les IP faisaient plus de soins à l’extérieur du centre et plus de sans rendez-vous. Médecins praticiens et IP consacraient une proportion semblable de leur temps à différentes tâches comme des soins cliniques directs ou des tâches administratives.
Conclusion
Quoique les IP soignent principalement des patients de leur propre groupe (selon le modèle de soins propre aux IP), elles partageaient certains patients avec les MF et leur prodiguaient certains soins selon le modèle de pratique des MF. Les patients traités conjointement par des MF et des IP avaient des caractéristiques plutôt différentes.
There is an ongoing search for better ways to organize primary health care to increase population access while maintaining or improving cost-effectiveness and the quality of other dimensions of care.1 Many jurisdictions use interprofessional teams, which include health providers such as social workers, dietitians, and nurse practitioners (NPs), to achieve these ends. Nurse practitioners have been noted as key members of these teams, and we have chosen to focus on this aspect of interprofessional teams.2 In Ontario, one such team is found in community health centres (CHCs). Community health centres are non-profit, community-governed organizations that deliver health, social, and community services to community members using interprofessional teams.3 Community health centres have operated for more than 40 years, and have employed both FPs and NPs for most of this time.4
There is considerable overlap in the scope of practice of NPs and FPs in primary care; however, there has been little guidance dictating how the 2 professions should divide tasks or work together.5 Several studies have identified variation in NP work patterns, especially when NPs are newly introduced into the primary care setting.6–8 Despite this variability, NPs’ practice styles can typically be classified under 1 of 2 distinct models: shared care or consultative care.9,10
The shared care model is characterized by NPs and FPs sharing a patient panel and seeing the same patients at the same or at different times and for different issues. In the consultative care model, NPs and FPs serve separate patient panels and consult with one another as required. In this manuscript, we refer to consultative care as the NP care model. Nurse practitioners working in the NP care model have been compared with FPs on dimensions such as cost efficiency,11,12 health outcomes,13,14 and patient satisfaction.15,16 Only a few studies have compared the actual tasks performed by FPs and NPs serving their own patient panels,17,18 and to our knowledge none has assessed this in the 2 different NP care models.
Across Canada, most provinces have now integrated NPs and other health professionals in primary care practices.19 However, there is no archetypal interprofessional model, and even practices within a single province are independently defining roles and activities of the different professionals. The Ontario CHC is a well established interprofessional model that is a publicly funded, not-for-profit organization governed by a board of directors, which can help support the communication and efforts required to establish optimal role definition. The purpose of this study was to compare and contrast the roles of FPs and NPs by evaluating work patterns and patient characteristics across the 2 groups that practise in the 3 archetypal models (ie, FP care, NP care, and shared care) in CHCs across eastern Ontario.
METHODS
Design
We employed a cross-sectional design using administrative data about patient encounters extracted from the CHCs’ electronic clinical management systems for the time period December 1, 2006, to November 30, 2008, as well as an organizational survey conducted in May 2009. Study procedures were guided by a reference group composed of CHC executive directors, FPs, and NPs. The study was approved by the Ottawa Hospital Research Ethics Board.
Setting
The study was set in CHCs and their satellites (ie, sites where health services are handled locally but administrative, financial, and human resource tasks are managed by a main site) operating in the Champlain and South East Local Health Integration Networks in eastern Ontario in 2008.
Sample
All 21 CHCs in the region were sent an introductory letter explaining the purpose of the study and inviting them to participate. Participation involved completing an organizational survey and allowing anonymized aggregate data to be extracted from the CHC’s patient data records. Patient records from each site were eligible for inclusion if there was at least 1 face-to-face visit with an NP or FP at the site during the 2-year study interval. There was 1 physician assistant practising in 1 CHC for less than half of the study period, and patient records from physician assistant visits were also included and grouped with NP visits.
Variables collected
Patient characteristics and encounter activities
Data extracted from the CHCs’ clinical management systems included patient sociodemographic characteristics and encounter-specific activities. The latter information was used to determine reasons for the visit and provider type. When a patient saw more than 1 provider on the same day, both encounters were captured as separate events.
Practice profile
A 25-item organizational survey was completed by the executive director or clinical manager at each site. The survey was adapted from one previously used by the research team20 and pilot-tested at 3 CHCs located outside of the study area. The survey captured information about number and types of clinical and nonclinical staff, physical layout, team structure, and the amount and type of work performed by its NPs and FPs (eg, hours of work, type of work, overtime). Managers were provided with the definitions of the NP care and shared care models, and they estimated what proportion of time the NPs in their practices worked in each model. Rurality of the practice was established by the use of the Rurality Index of Ontario score.21
Patient assignments to models of care
During the study period, CHC patients were assigned primary care providers upon registration, but this information was not updated over time and thus could not be used to indicate patients’ principal providers. Instead, we used the pattern of patient visits to assign each patient to 1 of 3 groups based on the percentage of his or her encounters with NPs versus FPs. The existing literature did not provide guidance about such an attribution approach, so our group reached consensus on the percentage cutoffs by examining the distribution of patient visits at all the sites. Patients who had more than 70% of their documented clinical encounters with FPs were attributed to the FP care group, and patients who had 70% or more of these encounters with NPs were attributed to the NP care group. Those who did not have more than 70% of their encounters with either group were attributed to the shared care group.
Analysis
Descriptive statistics of patient and practice characteristics, the 3 models of care, and NPs’ and FPs’ use of time were generated using data from all sites. The study was not powered to conduct statistical comparisons.
RESULTS
All 13 main CHCs and 8 satellite sites agreed to participate. Data were collected on patient visits from 44 849 unique patients. There were 82 FPs (53 full-time equivalent [FTE] providers) and 60 NPs (41 FTE) across all sites. For 1 satellite site, the clinical encounter data could not be separated from that of the main site, so the encounter data for the 21 sites are represented in 20 sites.
Description of study sites
The median number (range) of FTE providers per site was 2.0 NPs (0.1 to 4.7) and 3.0 FPs (0.4 to 6.4). The ratio of NPs to FPs across all sites was 0.83. In contrast to rural sites, which primarily served patients from surrounding geographic areas, most urban sites (82%) served priority populations. These included Francophones, homeless persons, persons with no health insurance, recent immigrants, young adults facing barriers, seniors, urban aboriginal people, sexual minorities (lesbian, gay, bisexual, and transgendered), and those with mental health or addiction issues.
Models of care
Based on encounter data, patients were assigned to FP care (53%), NP care (29%), or shared care (18%). This distribution is shown in Figure 1. Of the patients assigned to the 2 models in which NPs provided care in at least 30% of encounters, 63% were assigned to the NP care group and 37% to the shared care group. This division corresponded very closely to the practice managers’ estimated proportion of time that NPs spent working in the 2 care models at their sites: 62% in the NP care model and 38% in the shared care model (Figure 2). In 5 practices, NPs worked almost exclusively in the shared care model; however, in most of the sites, NPs were much more likely to have their own patient panels. There were no important differences in model of care patterns between the rural and urban practices or between main and satellite CHCs (results not shown).
Figure 1.

Proportion of patients treated under the FP care, shared care, and NP (consultative) care models: Of the 44 849 patients cared for in the centres evaluated, 29% were assigned to the NP care model, 18% were assigned to the shared care model, and 53% were assigned to the FP care model. This distribution was determined based on patient pattern of visits. Patients who saw FPs for > 70% of visits were attributed to the FP care group; patients who saw FPs for ≤ 70% and > 30% of visits were attributed to the shared care group; and patients who saw FPs for ≤ 30% of visits were attributed to the NP care group.
CHC—community health centre, NP—nurse practitioner.
Data were derived from health records.
Figure 2.
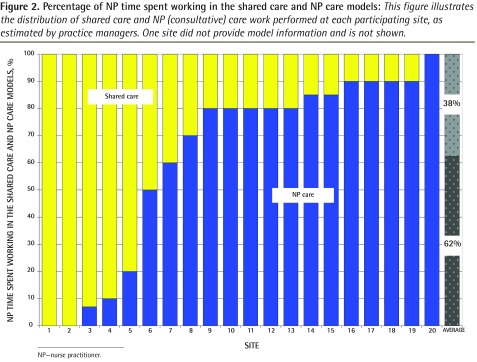
Percentage of NP time spent working in the shared care and NP care models: This figure illustrates the distribution of shared care and NP (consultative) care work performed at each participating site, as estimated by practice managers. One site did not provide model information and is not shown.
NP—nurse practitioner.
Patient characteristics
There were apparent differences in the profile of the patients served and in the services rendered across the FP care and NP care groups, with patients receiving shared care having an intermediate profile. For example, the proportions of female patients were 53%, 61%, 65%, in the FP care, shared care, and NP care groups, respectively. Similarly, average ages were 56, 34, and 29 years, in the 3 groups, respectively. A similar trend was observed with the likelihood of addressing a medical issue during a visit. For example, cardiovascular disease was addressed in 27%, 12%, and 4% of visits, and the average numbers of visits per year were 5.6, 4.9, and 3.0 in the 3 groups, respectively (Table 1).
Table 1.
Demographic characteristics of patient populations among the models of care
| CHARACTERISTICS | FP CARE | SHARED CARE BY FPS AND NPS | NP CARE |
|---|---|---|---|
| Patients* | |||
| Population served, n | 23 752 | 7902 | 13 195 |
| Female patients, % | 53 | 61 | 65 |
| Age, % | |||
| • 0–9 y | 6.6 | 14.9 | 17.8 |
| • 10–19 y | 8.9 | 15.5 | 17.8 |
| • 20–49 y | 36.5 | 44.0 | 49.6 |
| • 50–64 y | 27.8 | 17.6 | 11.4 |
| • ≥ 65 y | 20.3 | 10.4 | 3.4 |
| Mean age, y | 56 | 34 | 29 |
| Having at least some post-secondary education, % | 46 | 43 | 40 |
| Homeless, % | 2 | 2 | 5 |
| Recent immigrants (< 5 y in Canada), % | 3 | 3 | 5 |
| Uninsured, % | 1 | 1 | 3 |
| Encounter activities with patients | |||
| Average no. of yearly visits per patient | 5.6 | 4.9 | 3.0 |
| Social issues addressed, % | |||
| • Education | 1 | 1 | 1 |
| • Financial | 7 | 5 | 6 |
| • Legal | 2 | 2 | 2 |
| Medical issues, % | |||
| • Mental illness | 20 | 14 | 7 |
| • Arthritis | 9 | 4 | 1 |
| • Cardiovascular disease | 27 | 12 | 4 |
| • Diabetes | 12 | 5 | 2 |
| • Lung disease | 14 | 13 | 6 |
NP—nurse practitioner.
Patients were assigned to models of care based on the percentage of their visits to NPs versus FPs (see Figure 1).
Patterns of work
Managers reported a very similar distribution of activities across the 2 professions. Both NPs and FPs spent approximately two-thirds of their time in direct patient contact and approximately one-quarter on other tasks related to patient care (Figure 3). Nurse practitioners and FPs dedicated a similar portion of their time to performing various face-to-face duties outside of the clinic but tended to be involved in different types of activities. For example, outreach visits made up 7% and 2% of these encounters for NPs and FPs, respectively. Walk-in encounters and same-day or urgent visits made up 27% and 20% of the NP visits, respectively, and 9% and 27% of FP visits, respectively. Family physicians in rural and urban practices worked an average of 6.8 and 13.6 hours on call, respectively, and NPs in rural regions worked on call 2.8 hours. Urban practices indicated that NPs did not participate in on-call services.
Figure 3.

Percentage of total scheduled hours NPs and FPs spent on various activities, as reported by practitioners in organizational surveys: For every task, FPs and NPs reported similar or identical percentages.
FTE—full-time equivalent, NP—nurse practitioner.
The average appointment length was calculated from the weighted average of the booking interval for each of 4 appointment types and the proportion of appointments in each type. The average length of visit (range) was 34 minutes (22 to 45) for NPs and 28 minutes (22 to 38) for FPs.
DISCUSSION
This study documented differences in patient profile and care provision among the practice models of FPs and NPs in these Ontario CHCs. Other studies have reported similar contrasts, noting that NPs see higher proportions of patients in some vulnerable groups and perform more routine care on women and children, while FPs treat more patients with serious acute or chronic illnesses.18 This pattern might result from a number of factors, including legislation and regulations governing NP practice, NP education and continuing professional development, practice organization approaches to role clarity, implementation of NP role components, and support.22 During the time of this study, legislation and regulation in Ontario limited the number of medications NPs could prescribe and the diagnostic tests they could order,23 reducing their ability to deliver certain types of care.10,24,25 As a consequence, NPs reported that they were unable to prescribe about 30% of the drugs required by their patients.6 Nurse practitioner training at the time was a postbaccalaureate certificate, which might have emphasized care for conditions falling within their limited prescribing and diagnostic authority.6 Continuing education programs were also reportedly difficult for NPs to access.26 To maximize NPs’ ability to care for their own patients with minimal consultation with FPs, CHCs might have used intake questionnaires to determine whether an incoming patient would be assigned to an NP (less medical complexity) or FP (greater medical complexity). Nurse practitioners who found themselves caring for more medically complex patients were probably obliged to have FPs provide care that they were unable to provide themselves, potentially explaining the finding that shared care patients had characteristics intermediate to the FP care and NP care patients. Data on whether this model of patient distribution is most effective are not yet available; however, numerous Ontario studies have shown that the quality of primary care delivered in CHCs is at least equivalent or superior to that in other models.19,27–29 Further study of this model is needed to determine how shared care is negotiated and used, in addition to understanding its effect on patient care. Relaxation of the restrictions on prescribing and ordering of tests by NPs in Ontario in 2010, changes in NP training (which now requires a master’s degree), and improvements in continuing education might lead to changes in the division of patients within CHCs and in NP and FP patient panels.
Nurse practitioners and FPs in CHCs spent similar amounts of time on different clinical and nonclinical activities. Nurse practitioners in our study spent most of their work hours in direct patient care, a pattern also observed in other jurisdictions.24 On-call services were considerably more likely to be covered by FPs than NPs. This is especially evident in urban practices, where only FPs were reported to be responsible for on-call services (13.6 hours per week). It is unclear whether this pattern represents the relative scarcity of FPs in rural areas or whether other factors, such as funding for on-call services, might be responsible. Other studies comparing NPs with FPs reported that the former provide more disease prevention and supportive services,30 and report longer appointment times.15,30 In this salaried context, NP appointments (mean duration 34 minutes, range 22 to 45) were slightly longer than FP appointments (mean duration 28 minutes, range 22 to 38), and both NPs and FPs had longer booking appointments than had previously been reported in Ontario fee-for-service and capitation models (15 minutes).31
In our study, most of the clinical hours worked by NPs were done within an NP care model. This finding is similar to findings of other reports that NPs are able to provide a large amount of primary health care relatively autonomously.6 Nurse practitioners provided more walk-in care and fewer same-day appointments than FPs did. Nurse practitioners also performed more street outreach functions. Community health centres might have made NPs responsible for walk-in and outreach care because the tasks aligned well with functions they could carry out independently. Family physicians might have coded visits as “same day” or “urgent” when they were consulted by NPs about patients who were acutely ill.
Strengths and limitations
Our study has several key strengths, most notably in its setting. We were able to compare patient- and provider-level data from all CHCs operating in eastern Ontario during the study period, which provided us with a comprehensive picture of practice patterns and patient characteristics within that setting. Community health centres are a well established community-governed model of primary health care delivery with a particular focus on interprofessional practice, making them ideally suited to comparing NP and FP interaction.
However, our study also has several limitations. We relied largely on administrative data that might not have been an accurate or complete representation of patients’ health and social conditions. It is possible that some fields had not been thoroughly and consistently documented between provider groups and among the CHCs. While we collected more extensive data on the team structure, including the presence of other health professionals such as social workers and dietitians, we did not evaluate their roles, and, owing to the small sample size, could not relate the presence of these individuals to the observed medical roles of the NPs and FPs. The practice managers or executive directors responded to the organizational survey, and might not have represented provider activities accurately.
Conclusion
Nurse practitioners and FPs had similar work schedules but practised in 3 distinct models of care and served different patient panels. New larger studies could help further explain the roles of NPs and FPs in CHCs in the current less-restrictive regulatory environment. Future research might also examine the patterns of care in different primary health care practice models, as there has been an increase in the number of NPs practising outside of CHCs in recent years.6,32 It is especially important to understand how the division of the NP role and the FP role is established in the shared care model, and how the various approaches to structuring that model support better care.
Acknowledgments
Funding for this project was provided by the community health centres of the Champlain and South East Local Health Integration Network.
EDITOR’S KEY POINTS
This study documented differences in patient profiles and care provision among the practice models of nurse practitioners (NPs) and FPs in 21 Ontario community health centres.
Nurse practitioners and FPs dedicated a similar proportion of their time to performing various face-to-face duties outside of the clinic but tended to be involved in different types of activities. Nurse practitioners provided more walk-in care and fewer same-day appointments than FPs did. Nurse practitioners also performed more street outreach functions. Nurse practitioner appointments were also slightly longer than FP appointments were. On-call services were considerably more likely to be covered by FPs than NPs.
Compared with FPs, NPs saw patient panels that were less medically complex but more socially complex.
POINTS DE REPÈRE DU RÉDACTEUR
Dans cette étude, on a voulu déterminer ce qui différencie les modes de pratique des infirmières praticiennes (IP) et des MF pour ce qui est des types de patients et des soins dispensés, et ce, dans 21 centres de santé communautaires de l’Ontario.
Les infirmières praticiennes et les MF consacraient la même proportion de leur temps à des rencontres avec des patients à l’extérieur de la clinique, mais leurs activités étaient souvent différentes. Par rapport aux MF, les infirmières praticiennes faisaient plus de sans-rendez-vous et donnaient moins de rendez-vous le jour même. Elles assumaient aussi plus de fonctions à l’extérieur de la clinique. La durée de leurs rendez-vous était aussi plus longue que celle des MF. En-dehors des heures normales, les services étaient beaucoup plus souvent fournis par les MF que par les IP.
Par rapport aux patients des MF, ceux des IP avaient des conditions médicales moins graves mais des problèmes sociaux plus complexes.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Contributors
Drs Dahrouge and Muldoon conceptualized the current study, oversaw data collection, and planned the analyses. Dr Dahrouge conducted the statistical analysis and wrote the initial draft of the manuscript.
Drs Russell, Ward, and Hogg were consulted throughout the study. All authors reviewed, edited, and approved the final manuscript.
Competing interests
None declared
References
- 1.Canadian Institutes of Health Research. Canada’s strategy for patient-oriented research. Improving health outcomes through evidence-informed care. Ottawa, ON: Canadian Institutes of Health Research; 2011. Available from: www.cihr-irsc.gc.ca/e/documents/P-O_Research_Strategy-eng.pdf. Accessed 2014 Sep 30. [Google Scholar]
- 2.Virani T. Interprofessional collaborative teams. Ottawa, ON: Canadian Health Services Research Foundation; 2012. Available from: www.cfhi-fcass.ca/Libraries/Commissioned_Research_Reports/Virani-Interprofessional-EN.sflb.ashx. Accessed 2014 Sep 30. [Google Scholar]
- 3.Ministry of Health and Long-Term Care [website] Community health centre. Ottawa, ON: Ministry of Health and Long-Term Care; 2014. Available from: www.health.gov.on.ca/en/public/programs/hco/options/community.aspx. Accessed 2014 Sep 30. [Google Scholar]
- 4.Muldoon L, Rowan MS, Geneau R, Hogg W, Coulson D. Models of primary care service delivery in Ontario: why such diversity? Healthc Manage Forum. 2006;19(4):18–23. doi: 10.1016/S0840-4704(10)60240-2. [DOI] [PubMed] [Google Scholar]
- 5.Sangster-Gormley E, Martin-Misener R, Burge F. A case study of nurse practitioner role implementation in primary care: what happens when new roles are introduced? BMC Nurs. 2013;12:1. doi: 10.1186/1472-6955-12-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Koren I, Mian O, Rukholm E. Integration of nurse practitioners into Ontario’s primary health care system: variations across practice settings. Can J Nurs Res. 2010;42(2):48–69. [PubMed] [Google Scholar]
- 7.Humbert J, Legault F, Dahrouge S, Halabisky B, Boyce G, Hogg W, et al. Integration of nurse practitioners into a family health network. Can Nurse. 2007;103(9):30–4. [PubMed] [Google Scholar]
- 8.Sullivan-Bentz M, Humbert J, Cragg B, Legault F, Laflamme C, Bailey PH, et al. Supporting primary health care nurse practitioners’ transition to practice. Can Fam Physician. 2010;56:1176–82. [PMC free article] [PubMed] [Google Scholar]
- 9.DiCenso A, Matthews S. Report on the integration of primary health care nurse practitioners into the province of Ontario. Executive summary. Ottawa, ON: Ministry of Health and Long-Term Care; 2005. Available from: www.health.gov.on.ca/en/common/ministry/publications/reports/nurseprac03/exec_summ.pdf. Accessed 2014 Sep 30. [Google Scholar]
- 10.DiCenso A, Auffrey L, Bryant-Lukosius D, Donald F, Martin-Misener R, Matthews S, et al. Primary health care nurse practitioners in Canada. Contemp Nurse. 2007;26(1):104–15. doi: 10.5172/conu.2007.26.1.104. [DOI] [PubMed] [Google Scholar]
- 11.Rohrer JE, Angstman KB, Garrison GM, Pecina JL, Maxson JA. Nurse practitioners and physician assistants are complements to family medicine physicians. Popul Health Manag. 2013;16(4):242–5. doi: 10.1089/pop.2012.0092. Epub 2013 Mar 28. [DOI] [PubMed] [Google Scholar]
- 12.Liu N, D’Aunno T. The productivity and cost-efficiency of models for involving nurse practitioners in primary care: a perspective from queueing analysis. Health Serv Res. 2012;47(2):594–613. doi: 10.1111/j.1475-6773.2011.01343.x. Epub 2011 Nov 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lawson B, Dicks D, Macdonald L, Burge F. Using quality indicators to evaluate the effect of implementing an enhanced collaborative care model among a community, primary healthcare practice population. Nurs Leadersh (Tor Ont) 2012;25(3):28–42. doi: 10.12927/cjnl.2013.23057. [DOI] [PubMed] [Google Scholar]
- 14.Owens D, Eby K, Burson S, Green M, McGoodwin W, Isaac M. Primary palliative care clinic pilot project demonstrates benefits of a nurse practitioner-directed clinic providing primary and palliative care. J Am Acad Nurse Pract. 2012;24(1):52–8. doi: 10.1111/j.1745-7599.2011.00664.x. Epub 2011 Sep 4. [DOI] [PubMed] [Google Scholar]
- 15.Iglesias B, Ramos F, Serrano B, Fabregas M, Sanchez C, Garcia MJ, et al. A randomized controlled trial of nurses vs. doctors in the resolution of acute disease of low complexity in primary care. J Adv Nurs. 2013;69(11):2446–57. doi: 10.1111/jan.12120. Epub 2013 Mar 21. [DOI] [PubMed] [Google Scholar]
- 16.Mundinger MO, Kane RL, Lenz ER, Totten AM, Tsai WY, Cleary PD, et al. Primary care outcomes in patients treated by nurse practitioners or physicians: a randomized trial. JAMA. 2000;283(1):59–68. doi: 10.1001/jama.283.1.59. [DOI] [PubMed] [Google Scholar]
- 17.Salisbury CJ, Tettersell MJ. Comparison of the work of a nurse practitioner with that of a general practitioner. J R Coll Gen Pract. 1988;38(312):314–6. [PMC free article] [PubMed] [Google Scholar]
- 18.Way D, Jones L, Baskerville B, Busing N. Primary health care services provided by nurse practitioners and family physicians in shared practice. CMAJ. 2001;165(9):1210–4. [PMC free article] [PubMed] [Google Scholar]
- 19.Hutchison B, Levesque J, Strumpf E, Coyle N. Primary health care in Canada: systems in motion. Milbank Q. 2011;89(2):256–88. doi: 10.1111/j.1468-0009.2011.00628.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dahrouge S, Hogg W, Russell G, Geneau R, Kristjansson E, Muldoon L, et al. The Comparison of Models of Primary Care in Ontario (COMP-PC) study: methodology of a multifaceted cross-sectional practice-based study. Open Med. 2009;3(3):e149–64. Epub 2009 Sep 1. [PMC free article] [PubMed] [Google Scholar]
- 21.Ministry of Health and Long-Term Care [website] Communities by rurality index for Ontario (RIO) score. Ottawa, ON: Ministry of Health and Long-Term Care; 2013. Available from: www.health.gov.on.ca/en/pro/programs/northernhealth/rio_score.aspx. Accessed 2014 Sep 30. [Google Scholar]
- 22.DiCenso A, Bryant-Lukosius D, Martin-Misener R, Donald F, Abelson J, Bourgeault I, et al. Factors enabling advanced practice nursing role integration in Canada. Nurs Leadersh (Tor Ont) 2010;23:211–38. doi: 10.12927/cjnl.2010.22279. (Spec No. 2010) [DOI] [PubMed] [Google Scholar]
- 23.Donald F, Martin-Misener R, Bryant-Lukosius D, Kilpatrick K, Kaasalainen S, Carter N, et al. The primary healthcare nurse practitioner role in Canada. Nurs Leadersh (Tor Ont) 2010;23:88–113. doi: 10.12927/cjnl.2013.22271. (Spec No. 2010) [DOI] [PubMed] [Google Scholar]
- 24.Sangster-Gormley E. A survey of nurse practitioner practice patterns in British Columbia. Victoria, BC: University of Victoria School of Nursing; 2012. Available from: www.uvic.ca/hsd/nursing/assets/docs/news/np_practice_patterns.pdf. Accessed 2014 Sep 30. [Google Scholar]
- 25.Hanrahan C, Way C, Housser J, Applin M. Final report: the nature of the extended/expanded nursing role in Canada. St John’s, NL: Institute for the Advancement of Public Policy, Inc; 2001. [Google Scholar]
- 26.Baxter P, DiCenso A, Donald F, Martin-Misener R, Opsteen J, Chambers T. Continuing education for primary health care nurse practitioners in Ontario, Canada. Nurse Educ Today. 2013;33(4):353–7. doi: 10.1016/j.nedt.2012.07.018. Epub 2012 Aug 11. [DOI] [PubMed] [Google Scholar]
- 27.Dahrouge S, Hogg WE, Russell G, Tuna M, Geneau R, Muldoon LK, et al. Impact of remuneration and organizational factors on completing preventive manoeuvres in primary care practices. CMAJ. 2012;184(2):E135–43. doi: 10.1503/cmaj.110407. Epub 2011 Dec 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Glazier R, Zagorski B, Rayner J. Comparison of primary care models in Ontario by demographics, case mix and emergency department use, 2008/09 to 2009/10. Toronto, ON: Institute of Clinical Evaluative Sciences; 2012. Available from: www.cqco.ca/common/pages/UserFile.aspx?fileId=250501. Accessed 2014 Sep 30. [Google Scholar]
- 29.Russell GM, Dahrouge S, Hogg W, Geneau R, Muldoon L, Tuna M. Managing chronic disease in Ontario primary care: the impact of organizational factors. Ann Fam Med. 2009;7(4):309–18. doi: 10.1370/afm.982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Seale C, Anderson E, Kinnersley P. Comparison of GP and nurse practitioner consultations: an observational study. Br J Gen Pract. 2005;55(521):938–43. [PMC free article] [PubMed] [Google Scholar]
- 31.Dahrouge S, Hogg W, Ward N, Tuna M, Devlin RA, Kristjansson E, et al. Delivery of primary health care to persons who are socio-economically disadvantaged: does the organizational delivery model matter? BMC Health Serv Res. 2013;13:517. doi: 10.1186/1472-6963-13-517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Canadian Institute for Health Information. Regulated nurses: Canadian trends, 2006 to 2010. Ottawa, ON: Canadian Institute for Health Information; 2012. Available from: https://secure.cihi.ca/free_products/RegulatedNursesCanadianTrends2006-2010_EN.pdf. Accessed 2014 Sep 30. [Google Scholar]