

Abstract
Objective:
This study aims to evaluate and compare with the existing literature on the etiology, pattern, gender, and anatomical distribution of mandibular fractures.
Materials and Methods:
The data of 225 cases were analyzed over a period of 5 years between March 2009 and November 2013. Of this 110 were unilateral, 23 bilateral, 18 symphysis and 74 multiple fractures.
Results:
Males are more affected than females. The peak incidence rate is occurring in 30-35 years of age group. The most common fracture site is parasymphysis and least common site is ramus of mandible. The most common etiological factor is road traffic accident (RTA) (45.3%) followed by falls (42.6%), assaults (8.9%), sport injuries (2.2%), and gunshot wounds (0.89%).
Conclusion:
Thus, we conclude that RTA is the leading cause of mandibular fractures and males are more affected. The most common site is parasymphysis fracture in association with angle fracture. We observed that gender was significantly associated with body and angle fracture (P = 0.04) and significant relationship between etiology with multiple site fracture such as (parasymphysis-angle), (body-condyle), (body-angle), and (symphysis-condyle) was observed (P ≤ 0.05).
Keywords: Mandibular fracture, parasymphysis fracture, road traffic accident
Introduction
Mandibular fractures comprise most of the traumatic injuries, which are treated by an oral and maxillofacial surgeon. The facial area is one of the most commonly fractured site of the body,[1,2,3] of which mandible is the most frequent.[1,4,5] Injuries of the maxillofacial area can be psychologically disturbing for patients with a functional impact.[6] According to several studies, they account for 15.5-59% of all facial fractures.[7,8,9,10] A fracture is defined as “breach in the continuity of the bone.”[11] The occurrence of facial injuries tends to be high compared to injuries in other parts of the body because the face is without a protective covering, and the mandible the most prominent bone in this region of the body.[12,13] However, the presence of teeth in the mandible is the most important anatomical factor, which makes its fracture different from fractures elsewhere in the body.[14,15] This article aims to analyze retrospectively the age and gender distribution, etiology, and anatomic distribution of mandibular fractures among patients who visited Jodhpur Dental College and Hospital, Jodhpur, Rajasthan in a 5-year period.
Materials and Methods
Before the start of the study, ethical clearance was obtained from the Ethical Committee of the Institutional Review Board of Jodhpur Dental College and General Hospital. The data for this study were obtained from the medical records of 225 cases treated at Jodhpur Dental College and Hospital, Jodhpur, Rajasthan during the 5 years period between March 2009 and November 2013. Information was collected from the clinical and surgical notes of each of the patients in a standardized and systematic pattern. The demographic variables such as age, gender, and residence were assessed. Clinical information included diagnosis, etiology, and anatomical distribution of mandibular fractures was assessed.
Results
In this study, we observed that, total number of patients with mandibular fractures were 225, among them unilateral fractures were 110 (49%), bilateral fractures 23 (10.2%), symphysis 18 (8%), and multiple fractures were 74 (32.9%). Among unilateral fractures right side were 76 (69%) and left side were 34 (31%). Of 18 symphysis fracture three cases had unilateral canine impaction which was seen in OPG. Demographic variables and etiology were not statistically significant with a total number of fractures [Table 1].
Table 1.
Total number of mandibular fracture

Most common cause of fracture was road traffic accident (RTA) 102 (45.3%) followed by falls 96 (42.6%), assaults 20 (8.9%), sport injuries 5 (2.2%) and least commonly from gunshot wounds 2 (0.89%). Thus, we noticed that most common cause was RTA because of increasing number of vehicles now-a-days [Graph 1].
Graph 1.
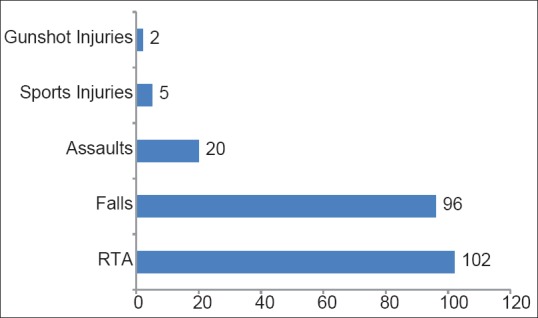
Etiology of mandibular fractures
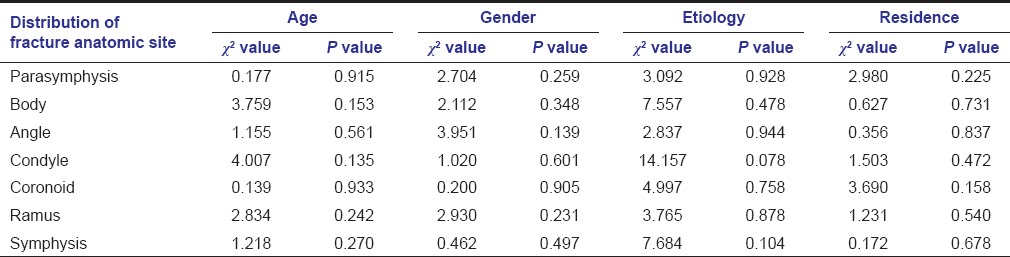
Among unilateral fractures, the most common site was parasymphysis area and among bilateral was body region. The least common site was the ramus region. Demographic variables and etiology were not statistically significant with distribution of fracture according to anatomic site [Table 2].
Table 2.
Distribution of mandibular fractures according to anatomic site
The order of fracture site from most common to least common were parasymphysis 49 (32.45%), body 42 (27.8%), angle 22 (14.56%), symphysis 18 (11.9%), condyle 13 (8.6%), coronoid 4 (2.64%), and lastly the ramus 3 (1.98%). The data for it is presented below [Graph 2].
Graph 2.
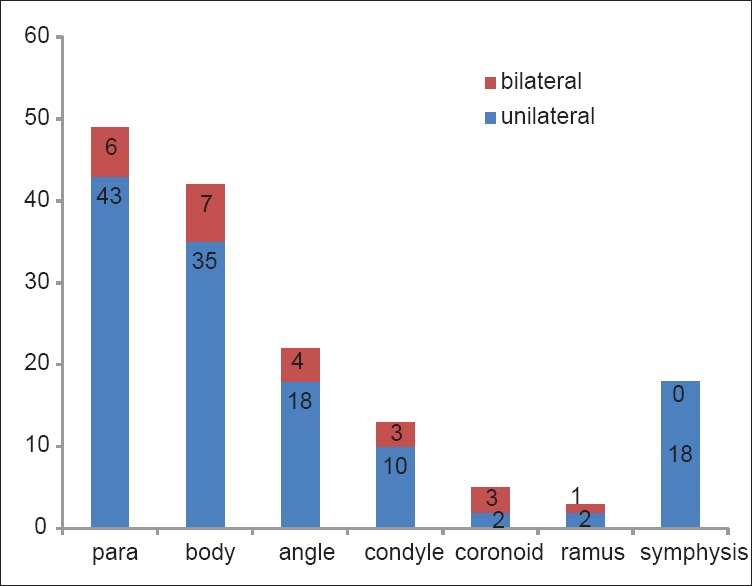
Anatomical and gender distribution of mandibular fractures
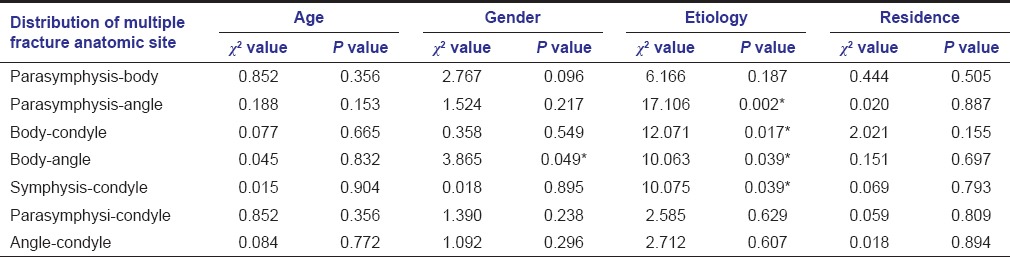
This study revealed that gender was significantly associated with body and angle fracture (P = 0.04) and significant relationship between etiology with multiple site fracture such as parasymphysis-angle, body-condyle, body-angle, and symphysis-condyle was observed (P ≤ 0.05) [Table 3].
Table 3.
Distribution of multiple mandibular fracture site
Discussion
Various studies on the incidence of mandibular fractures in different countries have been studied. The sheer pace of modern life with high-speed travel as well as an increasingly violent and intolerant society has made facial trauma a form of social disease from which no one is immune.[16] Mandible fractures if remains undiagnosed or inappropriately treated may lead to severe consequences on the cosmetic, functional and psychological aspects of the patients. The epidemiology of mandibular fractures has changed dramatically with the advent of higher speed limits, new seat belt and helmet laws, and increased urban violence.[16] Males were predominantly affected, which is in agreement with other studies.[8,17] due to more involvement in outdoor activities.
Most frequent cause of fracture mandible in this study was RTA, which is in accordance with Luce et al.,[18] Bataineh,[19] Shah et al.,[20] Al Ahmed et al.,[21] and Brasileiro and Passeri.[22] This was due to increasing number of vehicles, high-speed driving, less use of seat belts and absence of airbags in most of the vehicles and alcohol abuse during driving. In this study, fall from height is the second common etiologic factor accounting for 42.6% of the cases.
The anatomic distribution and incidence of mandibular fracture are widely variable.[23] Many authors reported symphysis[24] as the most frequently affected site whereas, others reported this to be mandibular body,[2,8,17,19] angle[16,25,26] and condyle.[20,21] In this study, the parasymphysis was the most frequently affected site probably due to the presence of permanent tooth buds in the pediatric mandible presenting a high tooth to bone ratio, while in adults it is partly to the length of canine root making the mandible anatomically weak in this region leading to most fractures. Among multiple fracture site we observed that the parasymphysis was commonly associated with angle, which is in accordance with the study by Dongas and Hall[25] and contrary to Ogundare et al.[26] have reported body with angle as the most common combination.
The incidence of mandibular fracture in this study increased with age above 25 years. The ages of the patient were divided into two groups: Group I below 25 years and II above 25 years. We found that the majority of cases were in Group II. This could be explained as children until the age of 6 years are under parental care thereby prevented from sustaining severe injuries and the elasticity of bones makes them less prone to fracture. As the age progresses, they are more involved in physical activities such as fast and rash driving, interpersonal violence, alcohol abuse, contact sports, and so forth. The peak incidence is occurring between 30 and 35 years and least being in the age above 50 years. This is in conformity with Adi et al.,[2] Bataineh,[19] Dongas and Hall,[25] Al Ahmed et al.,[21] Brasileiro and Passeri.[22]
This study revealed that most of the fractures occur in a rural population (55%) compared to urban population (45%) may be due to lack of education leading to unawareness of traffic rules not wearing helmets and tying seat belts.
In this study, out of 225 subjects unilateral fractures were 110 (49%), bilateral fractures 23 (10.2%) and symphysis 18 (8%). Multiple fractures were 74 (32.9%) contrary to Iida et al.[27] and Yamamoto et al.[28] Among unilateral fractures right side were 76 (69%), and left side were 34 (31%). Of 18 symphysis fracture three cases had unilateral canine impaction, which was seen in OPG.
Conclusion
We concluded from the foregoing study that the mandibular fractures were more common in males with the highest percentage in 30–35 years of age. RTA was the most common cause of fracture followed by falls, and the parasymphysis was the most common site. Among multiple mandible fractures, parasymphysis was most commonly associated with angle fractures. The fractures were seen more among the rural population hence there is a need to educate the rural population regarding road safety measures in specific and the whole city population in general. It is a need of the hour to educate the rural population regarding work ergonomics to prevent accidents and falls.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Abiose BO. Maxillofacial skeleton injuries in the western states of Nigeria. Br J Oral Maxillofac Surg. 1986;24:31–9. doi: 10.1016/0266-4356(86)90037-9. [DOI] [PubMed] [Google Scholar]
- 2.Adi M, Ogden GR, Chisholm DM. An analysis of mandibular fractures in Dundee, Scotland (1977 to 1985) Br J Oral Maxillofac Surg. 1990;28:194–9. doi: 10.1016/0266-4356(90)90088-3. [DOI] [PubMed] [Google Scholar]
- 3.Allan BP, Daly CG. Fractures of the mandible. A 35-year retrospective study. Int J Oral Maxillofac Surg. 1990;19:268–71. doi: 10.1016/s0901-5027(05)80417-5. [DOI] [PubMed] [Google Scholar]
- 4.Azevedo AB, Trent RB, Ellis A. Population-based analysis of 10,766 hospitalizations for mandibular fractures in California, 1991 to 1993. J Trauma. 1998;45:1084–7. doi: 10.1097/00005373-199812000-00020. [DOI] [PubMed] [Google Scholar]
- 5.Freidl S, Bremerich A, Gellrich NC. Mandibular fractures. An epidemiological study of a 10-year cohort. Acta Stomatol Belg. 1996;93:5–11. [PubMed] [Google Scholar]
- 6.Boole JR, Holtel M, Amoroso P, Yore M. 5196 mandible fractures among 4381 active duty army soldiers, 1980 to 1998. Laryngoscope. 2001;111:1691–6. doi: 10.1097/00005537-200110000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Brook IM, Wood N. Aetiology and incidence of facial fractures in adults. Int J Oral Surg. 1983;12:293–8. doi: 10.1016/s0300-9785(83)80016-7. [DOI] [PubMed] [Google Scholar]
- 8.Ellis E, 3rd, Moos KF, el-Attar A. Ten years of mandibular fractures: An analysis of 2,137 cases. Oral Surg Oral Med Oral Pathol. 1985;59:120–9. doi: 10.1016/0030-4220(85)90002-7. [DOI] [PubMed] [Google Scholar]
- 9.Scherer M, Sullivan WG, Smith DJ, Jr, Phillips LG, Robson MC. An analysis of 1,423 facial fractures in 788 patients at an urban trauma center. J Trauma. 1989;29:388–90. doi: 10.1097/00005373-198903000-00020. [DOI] [PubMed] [Google Scholar]
- 10.van Hoof RF, Merkx CA, Stekelenburg EC. The different patterns of fractures of the facial skeleton in four European countries. Int J Oral Surg. 1977;6:3–11. doi: 10.1016/s0300-9785(77)80066-5. [DOI] [PubMed] [Google Scholar]
- 11.Kruger GO. 6th ed. India: Jaypee Brothers; 1990. Textbook of Oral and Maxillofacial Surgery. [Google Scholar]
- 12.Huelke DF. Mechanism in the production of mandibular fractures. J Oral Surg. 1968;26:86–9. [Google Scholar]
- 13.Akama MK, Chindia ML, Ndungu FL. Occurrence and pattern of mandibular fractures at Kisii District Hospital, Kenya. East Afr Med J. 1993;70:732–3. [PubMed] [Google Scholar]
- 14.Rowe NL, William J. 2nd ed. Edinburgh: Churchill Livingstone; 1994. Maxillofacial Injuries; p. 216. [Google Scholar]
- 15.Banks P, Brown A. 2nd ed. Oxford, Woburn: Butterworth-Heinemann; 2001. Fractures of the Facial Skeleton; pp. 171–85. [Google Scholar]
- 16.Natu SS, Pradhan H, Gupta H, Alam S, Gupta S, Pradhan R, et al. An epidemiological study on pattern and incidence of mandibular fractures. Plast Surg Int 2012. 2012 doi: 10.1155/2012/834364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Olson RA, Fonseca RJ, Zeitler DL, Osbon DB. Fractures of the mandible: A review of 580 cases. J Oral Maxillofac Surg. 1982;40:23–8. doi: 10.1016/s0278-2391(82)80011-6. [DOI] [PubMed] [Google Scholar]
- 18.Luce EA, Tubb TD, Moore AM. Review of 1,000 major facial fractures and associated injuries. Plast Reconstr Surg. 1979;63:26–30. doi: 10.1097/00006534-197901000-00005. [DOI] [PubMed] [Google Scholar]
- 19.Bataineh AB. Etiology and incidence of maxillofacial fractures in the north of Jordan. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;86:31–5. doi: 10.1016/s1079-2104(98)90146-9. [DOI] [PubMed] [Google Scholar]
- 20.Shah A, Ali AS, Abdus S. Pattern and management of mandibular fractures: A study conducted on 264 patients. Pak Oral Dent J. 2007;27:103–6. [Google Scholar]
- 21.Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: A review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:166–70. doi: 10.1016/j.tripleo.2004.01.020. [DOI] [PubMed] [Google Scholar]
- 22.Brasileiro BF, Passeri LA. Epidemiological analysis of maxillofacial fractures in Brazil: A 5-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:28–34. doi: 10.1016/j.tripleo.2005.07.023. [DOI] [PubMed] [Google Scholar]
- 23.Imazawa T, Komuro Y, Inoue M, Yanai A. Mandibular fractures treated with maxillomandibular fixation screws (MMFS method) J Craniofac Surg. 2006;17:544–9. doi: 10.1097/00001665-200605000-00026. [DOI] [PubMed] [Google Scholar]
- 24.Chuong R, Donoff RB, Guralnick WC. A retrospective analysis of 327 mandibular fractures. J Oral Maxillofac Surg. 1983;41:305–9. doi: 10.1016/0278-2391(83)90297-5. [DOI] [PubMed] [Google Scholar]
- 25.Dongas P, Hall GM. Mandibular fracture patterns in Tasmania, Australia. Aust Dent J. 2002;47:131–7. doi: 10.1111/j.1834-7819.2002.tb00316.x. [DOI] [PubMed] [Google Scholar]
- 26.Ogundare BO, Bonnick A, Bayley N. Pattern of mandibular fractures in an urban major trauma center. J Oral Maxillofac Surg. 2003;61:713–8. doi: 10.1053/joms.2003.50118. [DOI] [PubMed] [Google Scholar]
- 27.Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial fractures. Int J Oral Maxillofac Surg. 2001;30:286–90. doi: 10.1054/ijom.2001.0056. [DOI] [PubMed] [Google Scholar]
- 28.Yamamoto K, Kuraki M, Kurihara M, Matsusue Y, Murakami K, Horita S, et al. Maxillofacial fractures resulting from falls. J Oral Maxillofac Surg. 2010;68:1602–7. doi: 10.1016/j.joms.2009.09.029. [DOI] [PubMed] [Google Scholar]