

Abstract
Dendritic myxofibrolipoma is a newly described benign soft tissue tumor that could be easily mistaken for sarcoma. It develops primarily in the subcutis or muscular fascia of the head and neck, shoulders, etc. Histologically, the tumor is characterized by an admixture of mature adipose tissue, spindle and stellate cells, and abundant myxoid stroma with prominent collagenization. These neoplasms typically show positive immunoreactivity for CD-34, vimentin and Bcl-2. Herein, we described a rare case presenting with a papule on the nasal tip in a 69-year old patient. Histopathology and immunohistochemical staining confirmed the diagnosis. In short, it brings the attention of clinicians to the importance of proper identification and characterization of this tumor.
Keywords: Dendritic fibromyxolipoma, fibrous papule, spindle cell lipoma, solitary fibrous tumor, myxoid liposarcoma
Introduction
Dendritic fibromyxolipoma (DFML) is a rare benign soft tissue lesion that most commonly located in the subcutis or muscular fascia of the head and neck, shoulders, chest wall, back in adult male patients [1]. Occasionally, there are cases of DFML reported in the intramuscular, forearm and inguinal and perineum regions [2-4]. Clinically, it presents with a papule or nodule, measuring from 2 to 11 cm in greatest diameter. Histologically, the tumor is characterized by an admixture of mature adipose tissue, spindle and stellate cells, and abundant myxoid stroma with prominent collagenization [1]. These neoplasms typically show positive immunoreactivity for CD-34, vimentin and Bcl-2 [1-4]. Herein, we described a rare case presenting with a papule on the nasal tip in a 69-year old patient. Histopathology and immunochemical staining confirmed the diagnosis.
Case report
A 69-year-old man presented with a skin-colored lesion on his nasal tip of approximately 4 years’ duration. The lesion always has grown up slowly with slight pruritus. Physical examination revealed a solitary, protuberant, rubbery and skin-colored papule, measuring 1.0 cm × 1.0 cm in size, locating on his nasal tip (Figure 1). Its smooth surface indicated slight teleangiectasia. His past and family histories were noncontributory. He was otherwise healthy and all routine laboratory tests were within normal range.
Figure 1.

A Solitary papule with well-circumscribed located on his nasal tip.
Histologically, the exogenous tumor was mainly composed by a proliferation of small spindle or stellate cells, variably admixed with mature adipose tissue, embedded within an abundant myxoid and collagenized stroma in the dermis (Figure 2A). The spindle cells had a small hyperchromatic nuclei in which pleomorphism, atypia, or mitotic activity were extremely rare (Figure 2B). Immunohistochemical staining revealed that the spindle and stellate cells stained strongly positive for CD34 (Figure 3A), vimentin (Figure 3B), and faintly positive for bcl-2 antibodies. Ki-67 showed a lower proliferation index < 2%. Stains for smooth muscle actin, desmin and S-100 were negative.
Figure 2.
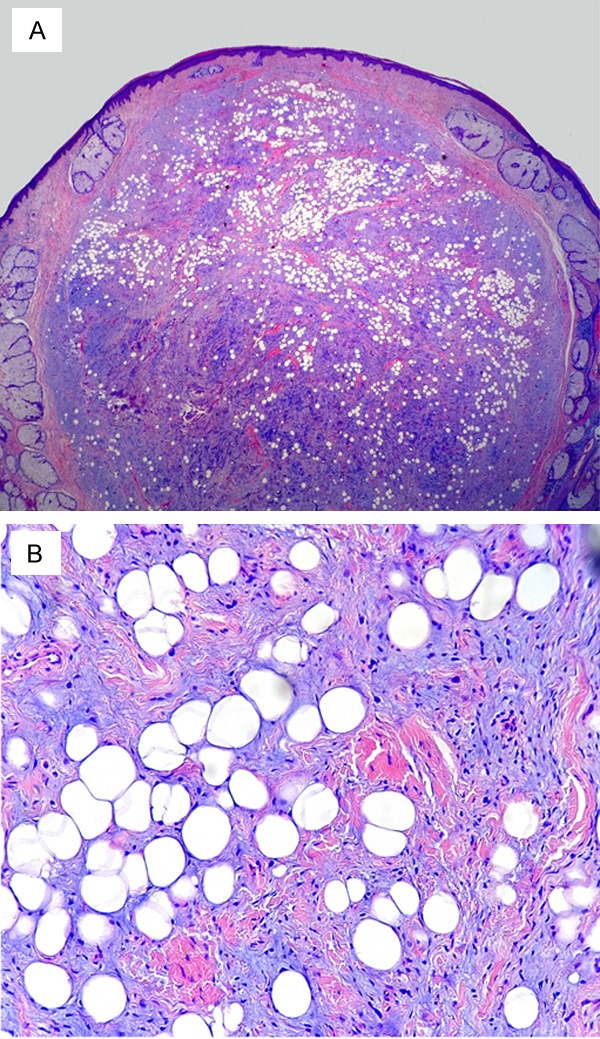
A. Histological features of the lesion showed the tumor was composed by small spindle cells, variably admixed with mature adipose tissue, embedded within an abundant myxoid (HE × 40). B. Higher magnification indicated spindle and stellate cells with thin, dendritic cytoplasmic prolongations (HE × 400).
Figure 3.
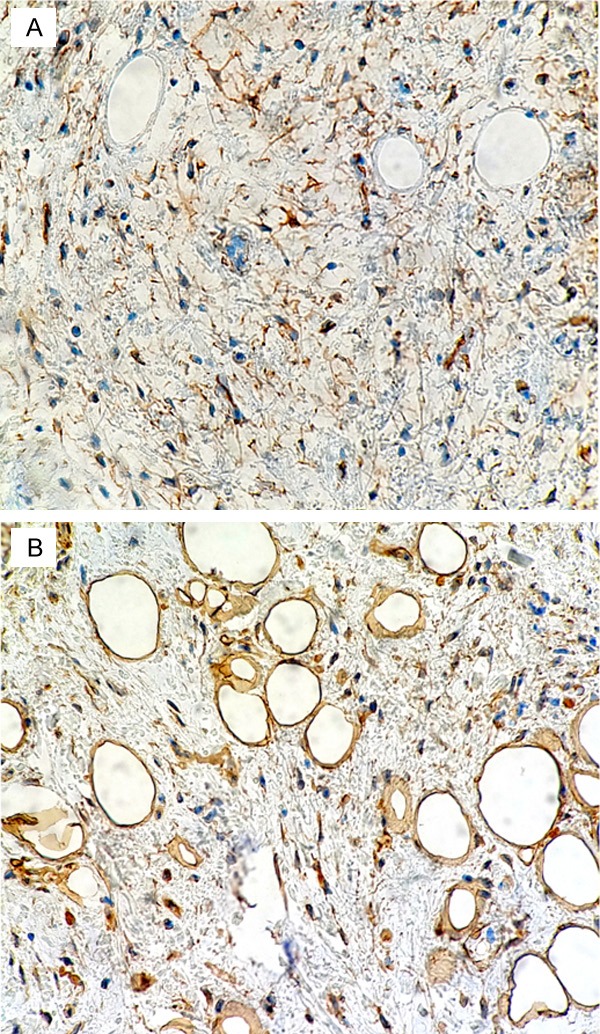
The spindle and stellate cells stained strongly positive for CD34 (A) and vimentin (B). Immunohistochemistry × 200.
Discussion
Dendritic fibromyxolipoma is an uncommon benign soft tissue tumor that first reported by Suster et al. in 1998 [1]. The mass more commonly arises in the subcutaneous tissue or muscular fascia of the head and neck, shoulders, chest wall or back, and predominantly affects male adults; rare cases were reported in the intramuscular, forearm, lower lip, inguinal and perineum regions [2-5]. Clinically, it presented with a papule or nodule and occurred at age of 33 to 81 years (mean, 64 years), and measured from 2 to 11 cm in greatest diameter (mean, 6 cm) [1]. Lesion in the dermis with size less than 2 cm has not been reported.
Clinical differential diagnosis mainly includes fibrous papule, angiofibroma, epithelioid cell histiocytoma and keloid. Fibrous papule of the nose occurs in adults as dome-shaped, sessile, skin-colored, white or reddish papules, 3-6 mm in diameter, on or near the nose [6]. Like angiofibromas with a solitary nonhereditary form, fibrous papules demonstrate concentric fibrosis surrounding vessels and adnexal structures. Stellate dermal dendrocytes are often prominent [6,7]. Epithelioid cell histiocytoma is a distinctive, rare, epithelioid form of benign fibrous histiocytoma and usually presents with a solitary, asymptomatic, erythematous, dome-shaped nodule on the extremities and trunk [8]. A keloid is a firm, irregularly shaped, fibrous, pink or red excrescence. The growth usually arises as the result of a trauma, rarely on the face and may be telangiectatic. It is usually not difficult to distinguish from these diseases above according to clinicopathological features.
The most striking histological feature of DFML is an admixture of mature adipose tissue, spindle and stellate cells, and abundant myxoid stroma with prominent collagenization. Immunohistochemically, vimentin and CD34 immunohistochemical stains accentuated the cell’s dendritic nature by revealing slender, complex cytoplasmic prolongations.
Histologically, DFML should be differentiated from some benign and malignant lesions: spindle cell lipoma (SCL), solitary fibrous tumor (SFT), lipoblastoma, lipoblastomatosis, nodular fascitis and myxoid liposarcoma (MLS) [1,4]. SCL shares many features with DFML including age, male predilection, location, gross features. Suster et al. [1] emphasized the dendritic nature of the spindle cells, the plexiform vascular pattern, and the abundance of keloidal collagen as the three essential features in DFML, which were not commonly presented in SCL. Moreover, the similar clinicopathological features of the lesions make it difficult for distinguishing DFML from myxoid variants of SCL. So some authors speculate that DFML probably represents an unusual variant of myxoid SCL [2].
The “hemangiopericytoma-like” vascular pattern and the lack of an adipose tissue component are two histologically features for differentiating SFT from DFML [4,9]. The patients’ age and the absence of lipoblasts were a key discriminating point between DFML and lipoblastoma and lipoblastomatosis [10]. Nodular fascitis shows proliferating spindle cells embedded in a loosely textured myxoid and inflammatory stroma. Unlike DFML, the lesion is relatively well circumscribed but poor encapsulated. Immunohistochemically, the spindle cells are positive for muscle markers except desmin and are S-100 protein and CD-34 negative [11].
MLS shares many features with DFML including a delicate plexiform vascular pattern, large size, and a myxoid matrix. But MLS is distinguished from DFML by the lower extremities fascial planes predilection, the infiltration of surrounding structures, and the presence of lipoblasts on higher magnification [12].
The histological features of our case were similar to those of the reported DFML cases, except for its rather small size, unusual site, histological changes in superficial dermis and only 4-year duration. The treatment of this case is remedied by simple excision of the lesion and a close follow-up.
In summary, we describe a rare case of DFML on the nasal tip. It is difficult for distinguishing DFML from SFT, especially for myxoid variants of SCL. Due to our limited hospital conditions, further study such as immunohistochemical staining like STAT6 expression could not be implemented.
Disclosure of conflict of interest
None.
References
- 1.Suster S, Fisher C, Moran CA. Dendritic fibromyxolipoma: clinicopathologic study of a distinctive benign soft tissue lesion that may be mistaken for a sarcoma. Ann Diagn Pathol. 1998;2:111–20. doi: 10.1016/s1092-9134(98)80047-6. [DOI] [PubMed] [Google Scholar]
- 2.Karim RZ, McCarthy SW, Palmer AA, Bonar SF, Scolyer RA. Intramuscular dendritic fibromyxolipoma: myxoid variant of spindle cell lipoma? Pathol Int. 2003;53:252–8. doi: 10.1046/j.1320-5463.2003.01464.x. [DOI] [PubMed] [Google Scholar]
- 3.Dahlin LB, Ljungberg O. Dendritic fibromyxolipoma adherent to the median nerve in the foream. J Plast Surg Hand Surg. 2012;46:120–3. doi: 10.3109/02844311.2010.503083. [DOI] [PubMed] [Google Scholar]
- 4.Zhang XJ, Zhou S, Nie K, Chen da F, Kui GJ, Zhang XH. Dendritic fibromyxolipoma in the right inguinal and perineum regions: a case report and review of the literature. Diagn Pathol. 2013;8:157. doi: 10.1186/1746-1596-8-157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Al-Maskery AY, Al-Sidairy SM, Al-Hamadani AS. Dendritic Myxofibrolipoma: often misdiagnosed as sarcoma. Craniomaxillofac Trauma Reconstr. 2011;4:171–4. doi: 10.1055/s-0031-1286122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kucher C, McNiff JM. Epithelioid fibrous papule-a new variant. J Cutan Pathol. 2007;34:571–5. doi: 10.1111/j.1600-0560.2006.00667.x. [DOI] [PubMed] [Google Scholar]
- 7.Hall MR, Kovach BT, Miller JL. Unilateral facial angiofibromas without other evidence of tuberous sclerosis: case report and review of the literature. Cutis. 2007;80:284–8. [PubMed] [Google Scholar]
- 8.Jang MS, Kang DY, Park JB, Kang JS, Baek JW, Kim ST, Suh KS. Epithelioid cell histiocytoma: broad differential diagnostic considerations. J Dermatol. 2012;39:579–81. doi: 10.1111/j.1346-8138.2011.01429.x. [DOI] [PubMed] [Google Scholar]
- 9.Erdag G, Qureshi HS, Patterson JW, Wick MR. Solitary fibrous tumors of the skin: a clinicopathologic study of 10 cases and review of the literature. J Cutan Pathol. 2007;34:844–50. doi: 10.1111/j.1600-0560.2006.00728.x. [DOI] [PubMed] [Google Scholar]
- 10.Bourelle S, Viehweger E, Launay F, Quilichini B, Bouvier C, Hagemeijer A, Jouve JL, Bollini G. lipoblastoma and lipoblastomatosis. J Pediatr Orthop B. 2006;15:356–61. doi: 10.1097/01202412-200609000-00010. [DOI] [PubMed] [Google Scholar]
- 11.Squillaci S, Tallarigo F, Patarino R, Bisceglia M. Nodular fasciitis of the male breast: a case report. Int J Surg Pathol. 2007;15:69–72. doi: 10.1177/1066896906295999. [DOI] [PubMed] [Google Scholar]
- 12.Powers MP, Wang WL, Hernandez VS, Patel KS, Lev DC, López-Terrada DH. Detection of myxoid liposarcoma-associated FUS-DDIT3 rearrangement variants including a newly identified breakpoint using an optimized RT-PCR assay. Mod Pathol. 2010;23:1307–15. doi: 10.1038/modpathol.2010.118. [DOI] [PubMed] [Google Scholar]