

Abstract
Bowenoid papulosis (BP) corresponds to an in situ squamous cell carcinoma (SCC) located in the anogenital region. It is related to HPV, and presents with gray-brown elevated papules or plaques. A biopsy is needed to confirm the diagnosis; however, dermoscopy may be useful to differentiate this disease from other conditions, such as genital warts, seborrheic keratosis and lichen planus. In this paper we describe the dermoscopic findings in two patients with this disease.
Keywords: dermoscopy, bowenoid papulosis
Case report
Case 1
A 54 year-old-man, presented with multiple, small, well- defined, gray-brown, papules and small papillomatous patches located on his penis, which had appeared over the last year (Figure 1). Genital warts, lichen planus, a verrucous nevus and BP were suspected among our clinical diagnosis. The dermoscopy revealed a pigmented papillomatous surface, brown-gray dots arranged in a linear distribution at the periphery of the lesion, and widespread dotted vessels (Figures 2 and 3). A biopsy was done, and the histology showed mild hyperkeratosis, irregular acanthosis, dyskeratosis, cytological atypia and mitosis (Figures 4 and 5), consistent with the diagnosis of BP.
Figure 1.

Small gray-brown papules. (Copyright: ©2014 Marcucci et al.)
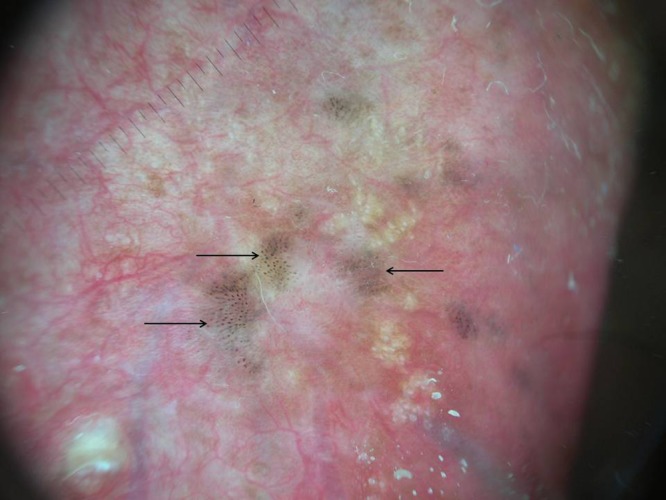
Figures 2 and 3.
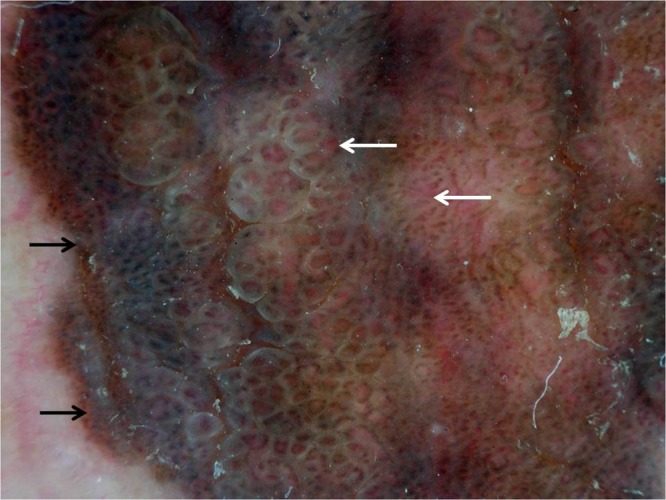
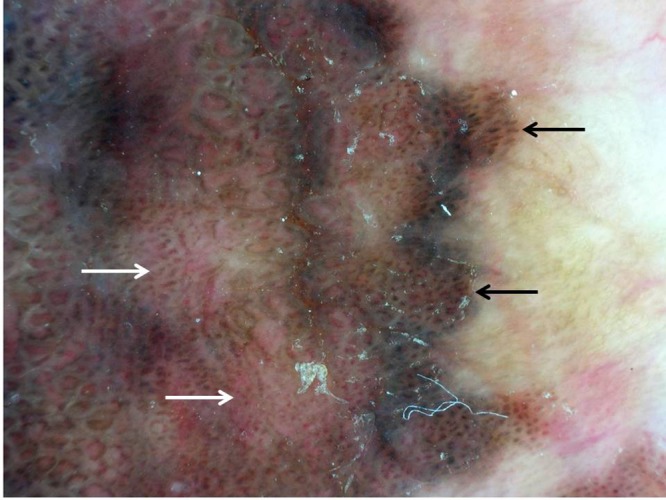
Pigmented papillomatous surface. Linear arrangement of brown-grey dots, at the periphery of the lesion (black arrow) and widespread dotted vessels (white arrow). Original magnification x10. (Copyright: ©2014 Marcucci et al.)
Figure 4.
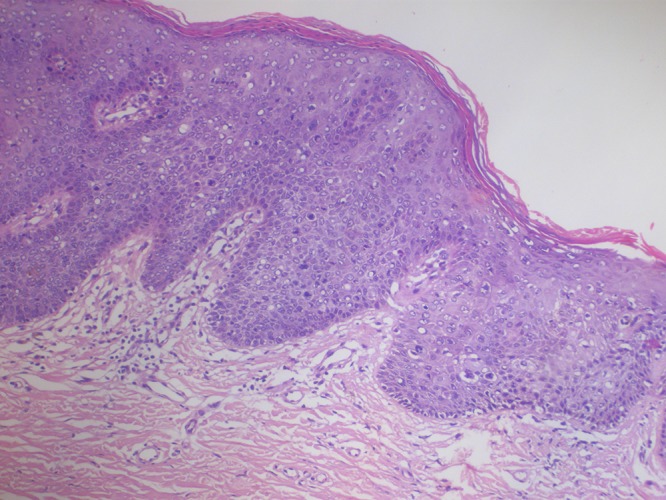
Mild hyperkeratosis, irregular acanthosis, dyskeratosis and mitosis (H&E X10). (Copyright: ©2014 Marcucci et al.)
Figure 5.
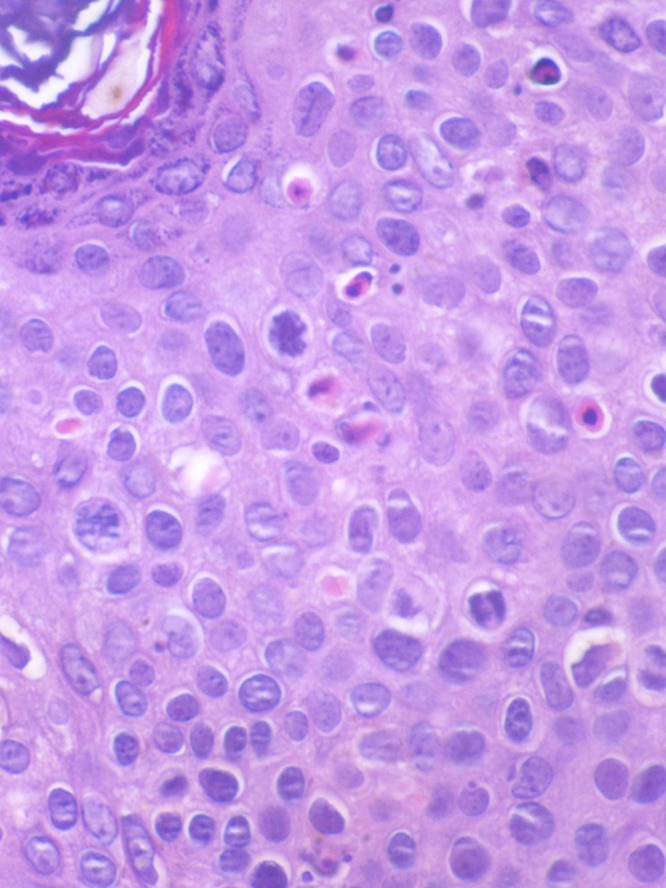
Cytological atypia, dyskeratosis and mitosis (H&E X40). (Copyright: ©2014 Marcucci et al.)
Case 2
A 31-year-old male patient with no relevant medical history presented with gray-brown asymptomatic small papules on his penis that had appeared a few months before (Figure 6). The dermoscopy revealed multiple areas with grey-brown dots aligned in a linear fashion and a keratotic surface. No vascular pattern could be identified (Figure 7). A skin biopsy was conducted and the histological examination confirmed the presence of BP.
Figure 6.

Gray-brown asymptomatic small papules. (Copyright: ©2014 Marcucci et al.)
Figure 7.
Multiple gray dots aligned in a linear fashion (black arrow). Original magnification ×10. (Copyright: ©2014 Marcucci et al.)
Discussion
BP represents a multifocal intraepithelial neoplasia located in the anogenital region [1]. The natural course of this disease is unpredictable: the lesions may increase, decrease, and even disappear spontaneously. Although progression to an invasive SCC is uncommon, it has been estimated in 2.6% of cases [2]. The most important differential diagnoses are genital warts, both clinically and dermoscopically [3].
To date and to our knowledge, no reports that specifically describe the dermoscopic findings of BP are available, and a few reports of dermoscopic examinations of this dermatosis have been published in the literature. Dong et al. [3] reported two cases of BP showing an unspecific pattern, and one of the lesions also showed dotted vessels and a keratotic surface as in our first case. In a study describing pigmented lesions of the vulva, Ferrari et al. [4] also presented 2 cases of BP: one lesion revealed brown to gray structureless areas and glomerular vessels in a clustered and linear arrangement; the other lacked pigmentation and revealed multiple whitish-red exophytic papillary structures with central glomerular and hairpin vessels.
The features of the two cases we presented were similar: brown-gray dots with a linear arrangement, located at the periphery of the lesion. These features remind us of pigmented Bowen’s disease, an in situ variant of cutaneous squamous cell carcinoma, which needs to be differentiated from BP at histopathological level [5,6].
Although more studies are needed to confirm these findings as criteria for BP, we think that in the presence of linear arrangement of brown-gray dots in a genital lesion, we should rule out BP among other diagnosis.
Footnotes
Funding: None.
References
- 1.Campione E, Centonze C, Diluvio L, et al. Bowenoid papulosis and invasive Bowen’s disease: a multidisciplinary approach. Acta Derm Venereol. 2013;93:216–56. doi: 10.2340/00015555-1328. [DOI] [PubMed] [Google Scholar]
- 2.Kutlubay Z, Engin B, Zara T, Tüzün Y. Anogenital malignancies and premalignancies: Facts and controversies. Clin Dermatol. 2013;31:362–73. doi: 10.1016/j.clindermatol.2013.01.003. [DOI] [PubMed] [Google Scholar]
- 3.Dong H, Shu D, Campbell TM, et al. Dermoscopy of genital warts. J Am Acad Dermatol. 2011;64:859–64. doi: 10.1016/j.jaad.2010.03.028. [DOI] [PubMed] [Google Scholar]
- 4.Ferrari A, Zalaudek I, Argenziano G, et al. Dermoscopy of pigmented lesions of the vulva: a retrospective morphological study. Dermatol. 2011;222:157–66. doi: 10.1159/000323409. [DOI] [PubMed] [Google Scholar]
- 5.Elston Dirk M. The diagnosis: bowenoid papulosis. Cutis. 2010;86:295–96. [PubMed] [Google Scholar]
- 6.Cameron A, Rosendahl C, Tschandl P, Riedl E, Kittler H. Dermatoscopy of pigmented Bowen’s disease. J Am Acad Dermatol. 2010;62:597–604. doi: 10.1016/j.jaad.2009.06.008. [DOI] [PubMed] [Google Scholar]