

Abstract
Background
Since 2002, the professional education for Swiss physiotherapists has been upgraded to a tertiary educational level. With this change, the need for research related to professional practice has become more salient. The elaboration of research priorities is seen as a possible way to determine the profession's needs, to help coordinate research collaborations and to address expectations regarding physiotherapy. There is still limited evidence about stakeholders' views with regard to physiotherapy research. The objective of this study was to investigate key stakeholders' opinions about research in physiotherapy in Switzerland.
Methods
Focus groups with patients, health professionals, researchers and representatives of public health organizations were conducted, and semi-structured interviews were conducted with politicians, health insurers and medical doctors from three linguistic regions in Switzerland. An interview guide was elaborated. Data were transcribed and analysed using inductive content analysis (Atlas-ti 6®).
Results
Eighteen focus groups and 23 interviews/written commentaries included 134 participants with various research experiences and from different settings. Fourteen categories were defined reflecting three themes: identity, interdisciplinarity and visibility. Stakeholders had positive views about the profession and perceived physiotherapists' important role now and in the future. Yet, they also felt that physiotherapy was not sufficiently recognized in society and not visible enough. A stronger professional identity would be key to enhancing interdisciplinary work.
Conclusions
Results of this qualitative study provide insights into key aspects for moving the physiotherapy profession forward. Identity is at the heart of physiotherapy, not necessarily in terms of research priorities but in the definition of domains of competence and future positioning. Identity is also tightly connected to Interdisciplinarity as this might threaten the existence of the profession. Stakeholders outside the profession insist on the importance of visibility. The results of this study can help stakeholders reflect on the future of physiotherapy and elaborate research priorities. © 2013 The Authors. Physiotherapy Research International published by John Wiley & Sons Ltd.
Keywords: interdisciplinary, physiotherapy, policy, qualitative research, research priorities
Introduction
Between 2002 and 2006, the professional education for Swiss physiotherapists has been upgraded to a tertiary educational level and is now taught at four Universities of Applied Sciences (UAS). With this change, the need for research related to professional practice has become more salient. To better address the profession's needs, to help coordinate research collaborations (Rushton and Moore, 2010) and to determine the stakeholders' expectations regarding topics to investigate (HRB, 2010), research priorities or agenda are recommended.
Yet, not only physiotherapists desire to define research priorities but also various health professionals such as nurses and occupational therapists (Ross et al., 2004; Bannigan et al., 2008; Imhof et al., 2008), specialty groups such as gerontology (Burnette et al., 2003) as well as countries such as Canada, USA and Ireland (Miles-Tapping et al., 1990; APTA, 2000; HRB, 2010) have defined topics to investigate. Distinct local, social and political circumstances require a specific process when stakeholders such as politicians and insurance representatives are involved. In addition, a recent literature review suggested involving patients and clinicians in the process of setting research priorities (Stewart et al., 2011).
Research priorities are hence a valuable contribution for planning research and development projects. They benefit the fostering of local, regional and national coordination of physiotherapy research and might support an international reflection on research priorities. Despite the importance of research priorities, limited evidence is available on the perceptions of various stakeholders with regard to the field of physiotherapy research in Switzerland. The overall aim of the study was to define relevant research topics and priorities from the perspective of stakeholder groups. The current paper presents the results of the qualitative part of this national research project. Its objective was to investigate key stakeholders' opinions on physiotherapy research and to gain more knowledge about the context of physiotherapy research and practice.
Methods
Design
The following flow chart (Figure 1) gives an overview of the research procedures. The first part aimed at exploring a broad understanding of physiotherapy research (i.e. qualitative), whereas the second (i.e. quantitative) part concerned the validation of the previously established key issues using a two-phase Delphi approach. The four UAS were involved in this project representing all higher education institutions offering physiotherapy programmes in Switzerland in three languages.
Figure 1.
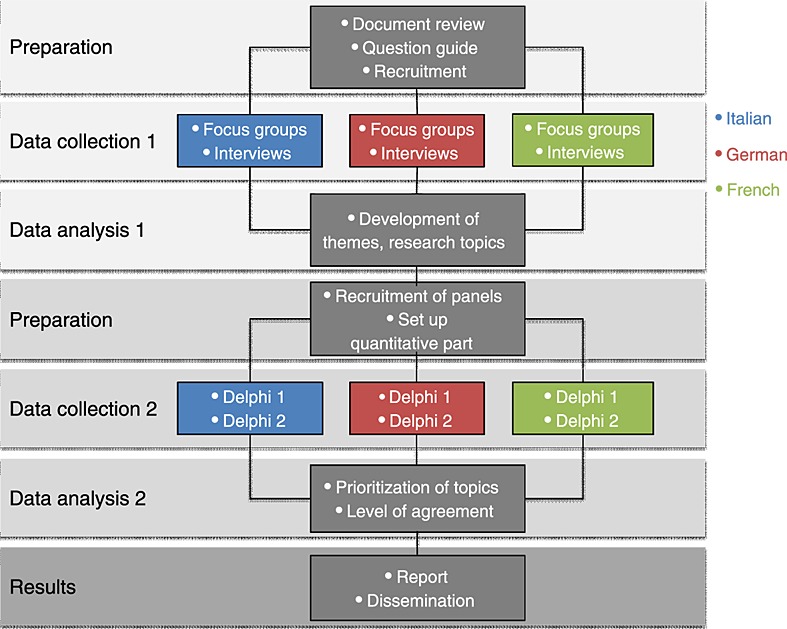
Overview of research procedures
Data collection
A general aim of qualitative research is ‘to discover and understand a phenomenon, a process, or the perspectives, worldviews of the people involved’ (Merriam, 1998, p. 11). As the current study cannot be grouped under a specific methodology, a generic qualitative methodology is suitable (Caelli et al., 2003). Four features are inherent to this research approach: transparency with regard to researchers' disciplinary affiliation and background as well as motivation for the study, congruence between research question and approach chosen, presentation of strategies to establish rigour and a detailed description of the process of data analysis (Caelli et al., 2003). Participants were recruited through various channels: the staff of the involved UAS, physiotherapy associations and local delegates, the heads of the university hospitals' physiotherapy departments, rehabilitation centres (staff and patients), local and national politicians, health insurers and registered local and national patient associations. Data collection included focus groups and semi-structured interviews. Focus groups have the advantage of bringing out more than just individual ideas (Kitzinger, 1995, 2005). As it was difficult to arrange focus groups, especially with politicians, health insurers and physicians, individual semi-structured interviews were conducted or, if time was limited, written responses were also accepted. An interview guide was established to ensure validity and transparency (Table 1). Ethical approval from local ethics committee was sought but not required (No 66/11, 14/11/2011.
Table 1.
Interview and focus group guide
| Outline | Questions | Follow-up questions |
|---|---|---|
| Introduction | ||
| Research | What do you understand with the term physiotherapy research? | - Other focus group discussions |
| - Related to physiotherapy field | ||
| What are your own questions for physiotherapy research? | - Personal expectations | |
| - Professional expectations | ||
| - Other references | ||
| Is physiotherapy research useful? | - Benefits? | |
| - Beneficiaries? | ||
| On what field/area should physiotherapy research concentrate? | - Different physiotherapy domains | |
| - Various disciplines | ||
| - Types of methods — questioning | ||
| Physiotherapy practice versus physiotherapy research | Which physiotherapy activity should be improved? | - Role in health prevention |
| - Role in health promotion | ||
| - Associated domains | ||
| How do you evaluate physiotherapy in regards to present challenges? | - Development potential | |
| - Specific questioning | ||
| - Development potential | ||
| Which are the specific positions of physiotherapy versus physiotherapy research? | - Actors | |
| - Clinical versus fundamental research | ||
| - Tension ‘education–research–clinic’ | ||
| What are the limits to physiotherapy research? | - Competences | |
| - Offer/demand | ||
| - Financial means | ||
| Physiotherapy researcher | What are the basic requirements to be a physiotherapy researcher? | - Knowledge |
| - Competences | ||
| - Stimulation of next generation | ||
| What is the profile of a ‘good’ physiotherapy researcher? | - Competences, experience | |
| - Attitude, spirit | ||
| - Positioning towards professionals, politics | ||
| - Political orientation versus scientific need | ||
| Final questions | What did surprise you? | - Points to deepen during interviews |
| Which are the important points to consider? | - Subjects to reflect about | |
| Which were the essential points discussed? | - On whose point of view | |
| - In which domains | ||
| - Summary of main points | ||
| - Take-home message | ||
| Conclusion |
Data analysis
Data was transcribed verbatim by research assistants using the software Atlas-ti 6 © (Cleverbridge AG, Cologne, Germany). A subsequent check was conducted to assess the levels of detail (Bucholtz, 2007), keeping in mind that the received information represented an event and is not the event itself (Green et al., 1997).
Following a conventional inductive content analysis approach (Hsieh and Shannon, 2005), text was highlighted into meaning units, which were abstracted and labelled with a code name in English. This analytic process was performed including all data. Categories were then established and discussed within the research group until an agreement was established. Although local teams met on a weekly basis and kept members informed about their progress on an internet platform, the entire research team met once a month during data collection and analysis phase to readjust codes and categories. Finally, the latent content was formulated into three main themes (Graneheim and Lundman, 2004). Examples are given in Figure 2.
Figure 2.
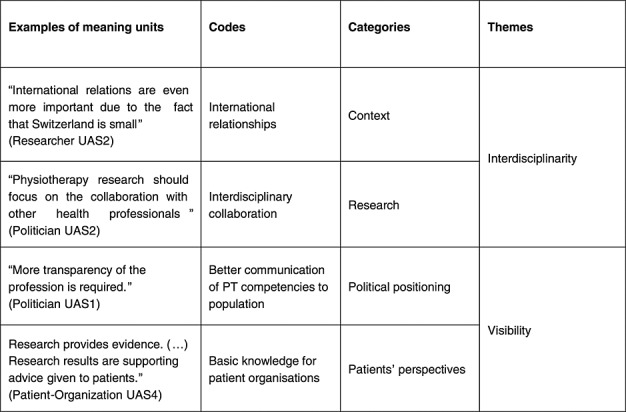
Illustration of example from meaning units into themes
Reflexivity
Reflexivity is the key criterion to ensure rigour of qualitative studies (Murphy et al., 1998). Finlay (2002) defines it as a thoughtful and conscious process, including ‘continuous evaluation of subjective responses, intersubjective dynamics, and the research process itself’ (p. 532). Furthermore, a systematic, rigorous and transparent procedure allows for scrutiny of the whole research process (Silverman, 2005). After each focus group or interview, a memo was written and shared among the members in order to make the growing understanding of the phenomenon explicit. Simultaneously, a coding manual accessible to all team members through the shared platform provided insight into this process and helped increase the awareness of development of thoughts and guided methodological steps (Moretti et al., 2011). An iterative analysis further ensured the validity of data analysis.
Results
Eighteen focus groups (duration: 37 minutes–1 hour 34 minutes), 19 individual semi-structured interviews (duration: 21–42 minutes) were conducted and four written commentaries received between February and September 2011, including 134 participants (patients, physiotherapy practitioners, researchers and educators, politicians, insurers and other healthcare professionals) from three linguistics regions in Switzerland (Table 2). Apart from one mixed group (rehabilitation team with different health professionals), focus groups were composed of professionals from the same background.
Table 2.
Description of participants
| Focus groups (n = 18 groups) | ||||
| Participants | UAS1 | UAS2 | UAS3 | UAS4 |
| Patient | 6 patients (5 male, 1 female) neurological patients in rehabilitation hospital | 7 patients (all female) with musculoskeletal problems in outpatient setting | 6 elderly diabetic patients (1 male, 5 female) | |
| Range: 42–63 years old | Range: 45–77 years old | Duration: 38 minutes | ||
| Duration: 1 hour 02 minutes | Duration: 49 minutes | |||
| Patient representative | 6 representatives of patient organizations (all female) | |||
| Range: 44–62 years old | ||||
| Duration: 1 hour 22 minutes | ||||
| Physiotherapy practitioner | 7 physiotherapists/practitioner in hospital (all female) | 7 physiotherapists (3 male, 4 female) 2 educators, 5 practitioners | 5 physiotherapists (all female) | 6 physiotherapists (2 male, 4 female) 1 educator, 1 researcher/practitioner, 2 team leaders, 2 novices) |
| Range: 31–52 years old | Range: 26–54 years old | Range: 45 years old; 12 years of experience | Range: 32–48 years old | |
| Duration: 1 hour 23 minutes | Duration: 1 hour 05 minutes | Duration: 58 minutes | Duration: 58 minutes | |
| 6 physiotherapists from the University Hospital (4 male, 2 female) between 5–10 years of experience | ||||
| Range: 28–48 years old | ||||
| Duration: 46 minutes | ||||
| 7 physiotherapist/practitioners (2 male, 5 female), between 14–29 years of experience | ||||
| Range: 36–53 years old | ||||
| Duration: 1 hour | ||||
| Physiotherapist educator/researcher | 7 educators/researchers (4 male, 3 female) moderate to extensive research experience | 6 educators (3 male, 3 female) 1 coordinator 5 educators/practitioners | 7 educators (2 male, 5 female) | 6 educators/researchers (3 male, 3 female) |
| Range: 27–58 years old | Range: 32–53 years old | Range: 45–54 years old | Range: 45–62 years old | |
| Duration: 1 hour 17 minutes | Duration: 55 minutes | Duration: 1 hour 34 minutes | Duration: 1 hour 23 minutes | |
| Multidisciplinary practitioner | 6 health professionals working in rehabilitation setting (3 male, 3 female) physician, neuropsychologist, physiotherapist, occupational therapist, nurse | |||
| Experience: 6–15 years | ||||
| Range: 20–48 years old | ||||
| Duration: 37 minutes | ||||
| Researcher | 5 researchers (4 male, 1 female) extensive research experience | |||
| Range: 40–48 years old | ||||
| Duration: 1 hour 25 minutes | ||||
| Health politician | 4 representatives of health organizations (3 male, 1 female) | |||
| Range: 40–70 years old | ||||
| Duration: 1 hour 09 minutes | ||||
| Physician | 7 physicians (5 male, 2 female), 1 cardiologic, 2 neurologist, 2 internal medicine, 1 rheumatologist, 1 general practitioner | |||
| Range: 40–57 years old | ||||
| Duration: 53 minutes | ||||
| Interviews (n = 19) | ||||
| UAS1 | UAS2 | UAS3 | UAS | |
| Patient representative | Patient representative | |||
| Duration: 32 minutes | ||||
| Physician | Physician hospital | Medical direction of rehabilitation clinic | ||
| Duration: 21 minutes | Duration: 35 minutes | |||
| General practitioner | General practitioner | |||
| Duration: 31 minutes | Duration: 34 minutes | |||
| Clinical director at the University Hospital | ||||
| Duration: 27 minutes | ||||
| Politician both at cantonal and federal level | Politician (cantonal level) | National councillor (federal level) | National councillor (federal level) | Health politician in retirement (both cantonal and federal level) |
| Duration: 35 minutes | Duration: 40 minutes | Duration: 38 minutes | Duration: 34 minutes | |
| Physiotherapy politician (federal level) | Former health politician at federal level | Physiotherapy educator/politician (cantonal level) | ||
| Duration: 29 minutes | Duration: 25 minutes | Duration: 42 minutes | ||
| Politician at cantonal level | ||||
| Duration: 26 minutes | ||||
| Insurance company | Insurance representative | Insurance representative | ||
| Duration: 29 minutes | Duration: 38 minutes | |||
| Physiotherapy educator | Dean of Physiotherapy Faculty | Dean of Physiotherapy Faculty | ||
| Duration: 33 minutes | Duration: 41 minutes | |||
| Physiotherapy educator/researcher | ||||
| Duration: 32 minutes | ||||
| Written commentaries (n = 4) | ||||
| Participants | UAS1 | UAS2 | UAS3 | UAS |
| Politician | Politician at cantonal level | Cantonal minister of health | ||
| Health politician at cantonal and federal level | Collaborator at Swiss Ministry of Health | |||
Table 3 provides information regarding qualifications and experience of researchers at the four sites. The two teams with less experience in interviewing and focus groups were coached by qualitative researchers who were present during the discussions and provided a feedback after the session.
Table 3.
Qualifications and background of research team
| Research team | ||||
|---|---|---|---|---|
| UAS1 | UAS2 | UAS3 | UAS4 | |
| Interviewers' background | Psychologist, PhD candidate | Physiotherapist MSc | Physiotherapist MSc/educational sciences | Physiotherapist MSc |
| Physiotherapist PhD | Sociologist BSc | Physiotherapist MSc | Physiotherapist MSc/Sociologist, PhD candidate | |
| Physiotherapist PhD | ||||
| Experience in interviewing and moderating focus groups | Experienced | Moderate experience | Moderate experience | Experienced |
The initially inductively defined 14 categories were reduced to six topics (physiotherapy research, physiotherapy profession, physiotherapy among others, education, patients' perspectives and research topics) (Figure 2). The six topics constituted the ‘manifest content’ (Graneheim and Lundman, 2004) and were used for elaborating structure of the quantitative Delphi questionnaire: participants of the Delphi survey rated statements on the current state and future positioning of physiotherapy and on the context of physiotherapy research. Furthermore, they prioritized physiotherapy research areas (e.g. physiotherapy assessment and diagnosis and physiotherapy education) and research topics related to areas of diseases (e.g. cardiothoracic and neurology) (part 2 of the entire study, reported elsewhere).
In the last step of qualitative analysis, the underlying meaning, ‘latent content’ (Graneheim and Lundman, 2004), was formulated into three themes: identity, interdisciplinarity and visibility (Figure 3).
Figure 3.
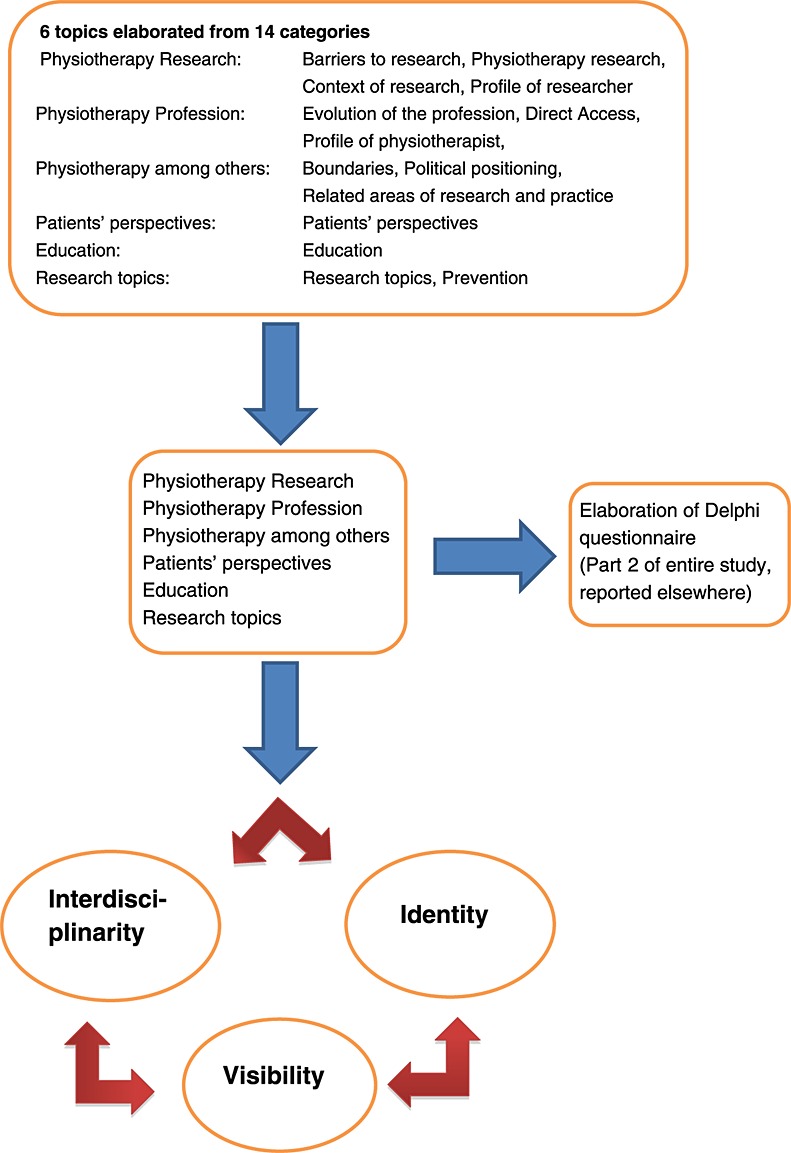
Three main themes
Identity
The results within this theme indicated that there was a quest for identity in the physiotherapy profession. Because of the ever changing healthcare environment, boundaries become blurred and research topics might be shared by different professions. Sports education, osteopathy or the fitness market were perceived as threatening the status of the physiotherapy profession. This threat, however, was not only visible from the inside. Insurance companies, educators and researchers were also questioning the specific identity of physiotherapy.
‘We are very close to the adapted sport education (…) and we are not really able to distinguish ourselves from those areas.’ (Educator, UAS4)
‘We engage in the question of integrated care and specialization within physiotherapy. Which way do physiotherapists go? (…) Are there specializations? (…) To which physiotherapist shall we send him, who cares that the patient can return to work?’ (Insurance, UAS1)
The focus groups with patients gave an idea of how the main beneficiaries of physiotherapy saw the physiotherapists' work and on what research and/or practice should focus on. Patient education, muscle strengthening and movement were considered core competencies of the profession. In addition, patients and their representatives insisted on the importance of good interaction between patients and physiotherapists.
‘Physiotherapy brings us a lot because one gets stronger, develops one's muscles.” (Patient, UAS4)
‘I think, motivation and communication of feedback (…), this is a major factor for treatment success. You can apply the best techniques – if feedback and motivation are not in line. I believe that this is the big part of the result.’ (Patient-organization, UAS1)
Patients insisted on getting individualized care from physiotherapists and perceived them as being passionate about their work. Yet, it should be mentioned that physiotherapists work in a challenging environment (limited time) and that patients felt the pressure that insurance companies put on available resources.
‘…not only the intellect, but that the heart is also involved.’ (Patient, UAS3)
‘In private practice the time allocated to the patient is reduced, but this is something that has not only to do with physiotherapists, but with health insurances too. (…) Their role is really important, especially for those who need to do physiotherapy all the time.’ (Patient, UAS2)
When it came to the definition of the physiotherapy profession, the statements were often a justification of physiotherapy interventions or an evaluation of assessment methods.
‘If we provide scientific evidence, that patients treated with physiotherapy have less recurrence, are better educated and have fewer medical consultations, health insurances should be interested in a better salary for physiotherapists.’ (Politician, UAS1)
More specifically, physiotherapy research should be performed by physiotherapists, because insider knowledge was considered important. Nevertheless, it was recognized that research skills were different from professional skills. Tension existed between practitioners who were asked to practice according to ‘best available evidence’ and researchers who should focus on relevant and practical issues. This means that adaptation seems necessary. An important aspect for participants was the need for sharing knowledge between both groups in order to reduce the gap between research and practice and to foster unity.
‘Anyway, if one is not a physiotherapist, it is hard, because one doesn't know the physiotherapy state of the art and therefore, doesn't know where the gaps are’ (Practitioner, UAS4)
‘It would be good to keep… to avoid physiotherapy on 2 levels… doctorates and practitioners… that the same physiotherapist could keep the aspect of research and clinic and also to make a bridge between the two’ (Practitioner, UAS4)
Stakeholders such as politicians, physicians or insurance company representatives were convinced that physiotherapy plays an important role in today's healthcare system, especially considering the demographic evolution.
‘Physiotherapists have competencies that physicians for example don't have. Physiotherapists are movement specialists and they cannot be replaced by the skills of an orthopedic surgeon or a rheumatologist.’ (Politician, UAS3)
‘Physiotherapy plays a major role in today's and future healthcare system.’ (Politician, UAS3)
Educating the next generation of physiotherapists will require a cultural change. Several stakeholders indicated that evaluating research studies was key for the future profession. It also seems necessary to debate and discuss and update their knowledge.
‘I think that there is a cultural change needed and it will come automatically. The generations we are educating are focused on research and the results from it.’ (Educator, UAS3)
‘It's important to give them this research wish, this wish to improve; it's a way to think (…) it's to push yourself under discussion, to update. It's something that can be given to you when you're studying, as an input’ (Physician, UAS2)
Stakeholders considered physiotherapy valuable and believe that the profession plays an important role in society. A stronger identity was seen as an opportunity to strengthen the domain of competency of physiotherapy. However, changes in the healthcare system were perceived as threatening, putting the profession at risk. Education should prepare future professionals for changes in the demographic, socio-political and health insurance context. The tension between practitioners and researchers will have to be tackled to ensure a cultural change for the next generation of professionals.
Interdisciplinarity
Interdisciplinarity was the second theme emerging from the data. Although it was closely linked to the theme ‘Identity’, it has to be considered separately. Various stakeholders such as patient representatives, health insurance, politicians and other health professionals insisted on the need for collaborative research.
‘That (i.e. collaboration) is a must these days and should be like this.’ (Patient-organization, UAS1)
‘There is a need for networks in the field of medicine, enabling the foundation of research.’ (Physician, UAS1)
‘Physiotherapy research should focus on the collaboration with other health professions and show its specificity’ (Politician, UAS4)
This collaboration was not only emphasized by the ‘outsiders’ but also physiotherapists from different areas valued interdisciplinarity highly.
‘I think that everything must be done in teamwork. We can't imagine that it's only one person or that it's only the physiotherapist having all those competencies. (…) Depending on what we are going to do we need a team who can support us.’ (Educator, UAS2)
‘But here to have done this work with the cancer group (i.e. interdisciplinary), to have exchanged, to have (read) those articles, to have given some thoughts, to have another practical experience, this was good.’ (Practitioner, UAS4)
Although expectations to perform high quality interdisciplinary research are high, participants were aware of barriers to research. Funding was not only a major concern but also the lack of structure (teams and organization) and education (doctoral studies and research skills) was viewed as an obstacle for conducting high quality research.
‘Dependent on funding it is clear that the research follows a certain direction, i.e. certain areas are investigated while others are not, just depending on the priority list of the funding sources.’ (Educator, UAS3)
‘There is neither structure nor education to do research’ (Practitioner, UAS4)
If the questions about identity and domain of competencies persist, interdisciplinary collaborations might prove difficult. Even though barriers to interdisciplinary research were identified as important and the future of health context challenging, collaboration seemed to be a prerequisite in order to bring the physiotherapy profession ‘to the next level’.
Visibility
The third theme described the environment in which physiotherapists practice. ‘Identity’ and ‘interdisciplinarity’ could be achieved from within the profession, yet positioning the profession in the political landscape was considered a key issue for future development of physiotherapy.
‘Physiotherapy does an excellent job, but it is unfortunately marginalized, not because of the quality of its benefit, but because of its size. And that should, in my opinion, be approached in another way, in sense of social marketing, which means to appear more outward with more publicity.’ (Educator, UAS1)
‘…to analyze legislative processes such as e.g. managed care. (…) figuring out where the emphases are that apply to physiotherapy (…) Physiotherapists should get a place in the managed care network.’ (Politician, UAS3)
Stakeholders believed that research could also contribute to the fostering of this visibility:
‘We should have costs-effectiveness analysis in the branch of physiotherapy as well, maybe with comparison of different therapies’ (Practitioner, UAS2)
‘To define research topics and priorities I would analyse health needs of the patients, of the population.’ (Politician, UAS2)
‘I think research can improve and consolidate the value of physiotherapy.’ (Practitioner, UAS1)
With the third theme, ‘visibility’, participants indicated the importance of the context. Socio-political as well as demographic change will require the profession to further develop and grow. Stakeholders stated the importance of analysing the populations' health needs in order to establish relevant and appropriate research priorities. It seemed to be not enough to treat patients effectively and efficiently, but lobbying and marketing were aspects not to be neglected. Results of research studies might help improve the visibility of the profession.
Discussion
The goal of this study was to identify stakeholders' opinions on research in the field of physiotherapy. Three themes — identity, interdisciplinarity and visibility — covered topics elaborated by participants. This qualitative part of the project helped reveal the participants' perceptions with regard to physiotherapy research and thereby provided a basis for further investigations using the Delphi method (reported elsewhere).
Identity
The results indicated that physiotherapy has not established a firm identity yet. Changes in demographics, health organizations and staff recruitment might dissolve boundaries of close professions, for example, that occupational therapy and physiotherapy should merge and that rehabilitation therapists should be created (Smith et al., 2000). This move would involve a mapping of core skills, unique skills and competencies in order to recommend a dual qualification and a combined profession. Professions have symbiotic relationships with society (Sparkes, 2002). Although society drives the demand for professionals' services, it also maintains a certain status of the profession. Professions have certain criteria to be considered such as skill level and systematic knowledge, the development of professional ethics, freedom of judgement and autonomy, high prestige and earnings and the provision of a crucial social function (Sparkes, 2002).
Participants emphasized the changing nature of the physiotherapy profession on two levels, first related to the problems addressed and second, regarding competencies increased. Physical activity as well as assessments of smoking habits, stress levels, sleep patterns and nutritional aspects should be part of physiotherapists' practice (Dean, 2009a). Physiotherapists have the advantage to work with patients over prolonged periods and are committed to health and well-being. They have therefore the capacity to minimize social and economic burdens of lifestyle conditions (Dean, 2009b). Direct access to physiotherapy has recently been promoted, and there is evidence that fear of overutilization or increased cost is unwarranted (Mitchell and de Lissovoy, 1997). The benefit of physiotherapy interventions gives therefore the profession an advantage in the healthcare field (Deyle, 2006).
The question of identity was mentioned by participants not only related to physiotherapy practice but also research in physiotherapy was not clearly established. Along this line, results of a study in nursing confirmed the challenge of adjusting to a new role when professionals move to a tertiary level (Duffy, 2012). He identified five stages in the adjustment to a new role as nurse educator: pre-entry, reaffirming, surmounting, stabilizing and actualizing. It became clear that identity is an evolving state of affair and that adjustment within educational context is not easily achieved.
It has been 10 years now since the Swiss physiotherapy education is embedded in a university education. It might just not have been long enough to embrace the new philosophy of clinical practice and research that comes with this change.
Interdisciplinarity
Each healthcare profession develops according to ‘their own and society's historic forces and sociological processes’ (Hall, 2005, p. 190). Various professions overlap in many areas and must therefore share some responsibilities (Hall, 2005). This opinion was also obtained by the participants in the current study. To collaborate successfully in teams, there is a need for respect of differences, trust and rules for ‘cohabitation’ (Curry et al., 2012). Selective collaboration, cross-training, sustained relationships, good humour and participation in peer reviews are just a few of the strategies helping to avoid pitfalls of interdisciplinarity (Giacomini, 2004).
Participants indicated the interdependence between identity and interdisciplinarity. Creating a strong identity increases the likelihood to be recognized for specific competencies, whereas collaborations make boundaries fade or even disappear. The example of sport rehabilitation exemplifies that while organizational changes promote multi-disciplinary healthcare teams, relations are also affected by specialization and legitimization discourses (Malcolm and Scott, 2011).
To legitimize their work, professionals rely on discourse by including reference to the scientific basis, the identification of particular skills and expertise, the holistic and patient-centred nature of practice, the provision of care and emotional support, organizational efficiency and accountability as well as claims to competence (Sanders and Harrison, 2008 cited in Malcolm and Scott, 2010).
Visibility
Switzerland is known for its direct democracy and its federalism giving the individual cantons an important role in the political landscape. One could assume that physiotherapists had a more direct approach to politicians, but this is not the case. Because of the limited number of physiotherapists (8232 members as of 31 March 2013), the Swiss Physiotherapy Association (Physioswiss, 2013) is not visible enough to politicians. Even though they started to be more present in the media, lobbying has been a cornerstone not only of the political agenda for the association (Physioswiss, 2011). Compared with bigger countries such as the USA where the American Physical Therapy Association (APTA, 2012) promotes a Federal Advocacy Forum for their members to lobby the American congress, the Swiss profession is less vocal. Another point expressed by participants was that physiotherapy research and the position of the profession could not be separated from the socio-political context in which the profession grows and develops. It is a continuous adaptation to the health needs of the population and to the scientific and political change.
Limitations
To minimize the limitations of the study and to increase reliability, the interview guide was established in English and was tested and adjusted (Blanchet and Gotman, 2005). Unfortunately, the number of participants in the three regions was not equally distributed. Although the French part provided the most focus groups, especially with physiotherapists, the German region interviewed more politicians than any other regions, and patients and physicians were the most frequent participants in the Italian region. However, there was no difference between the discourses of each linguistic region.
Interview citation help to provide transparency of the analytic process in the result section and increase the credibility of the data (Murphy et al., 1998). Because of the aforementioned translation of categories into English, some imprecision might have been produced. To minimize errors, a coding manual was established and shared within the group (Moretti et al., 2011).
Conclusions and implications
The results of this study indicated that a quest for identity is at the heart of physiotherapy, not necessarily in terms of research priorities but in the definition of domains of competencies and future positioning. Identity is tightly connected to interdisciplinarity and not being able to find the place might threaten the existence of the profession in an ever changing healthcare context. Stakeholders outside of the profession insisted on the importance of visibility, which was also brought up by the physiotherapy association. It has previously been argued that research priorities cannot solely be defined by professionals but must include users', collaborators' and funders' perspectives in order to formulate relevant research topics. The results of this nation-wide project will support the profession in defining future research actions and to prioritize research topics in the second part of the project, the Delphi survey. The findings could also be used to reflect on the future of physiotherapy and how physiotherapy education and research need to be adjusted in order to respond to the socio-political demands.
Acknowledgments
This study was supported by the following: Stiftung Physiotherapie Wissenschaften, Physioswiss, Réseau d'études aux confins de la santé et du social RECSS/HES-SO, as well as the UAS BFH, ZHAW, SUPSI and HES-SO. Ethical Approval submitted to Ethics Committee of Canton Vaud (Protocol 66/11; 14/11/2011).
REFERENCES
- APTA. Clinical research agenda for physical therapy. Physical Therapy. 2000;80:499–513. [PubMed] [Google Scholar]
- APTA. 2012. Federal Advocacy Forum. (Available at: http://www.apta.org/FederalForum/ ) (Accessed 9/11/2012)
- Bannigan K, Boniface G, Doherty P, Porter-Armstrong A, Scudds R. Priorities for Occupational Therapy Research in the United Kingdom: Executive Summary of the POTTER Project. British Journal of Occupational Therapy. 2008;71(1):13–16. [Google Scholar]
- Blanchet A, Gotman A. L'enquête et ses méthodes: l'entretien. Paris: Armand Colin; 2005. [Google Scholar]
- Bucholtz M. Variation in transcription. Discourse Studies. 2007;9(6):784–808. [Google Scholar]
- Burnette D, Morrow-Howell N, Chen LM. Setting priorities for gerontological social work research: a national Delphi study. Gerontologist. 2003;43(6):828–838. doi: 10.1093/geront/43.6.828. [DOI] [PubMed] [Google Scholar]
- Caelli K, Lynne R, Mill J. Clear as Mud': Toward Greater Clarity in Generic Qualitative Research. International Journal of Qualitative Methods. 2003;2(2):1–24. [Google Scholar]
- Curry L, O'Cathain A, Plano Clark VL, Aroni R, Fetters M, Berg D. The role of group dynamics in mixed methods health sciences research teams. Journal of Mixed Methods Research. 2012;6(1):5–20. [Google Scholar]
- Dean E. Physical therapy in the 21st century (Part I): Toward practice informed by epidemiology and the crisis of lifestyle conditions. Physiotherapy Theory and Practice. 2009a;25(5–6):330–353. doi: 10.1080/09593980802668027. [DOI] [PubMed] [Google Scholar]
- Dean E. Physical therapy in the 21st century (Part II): Evidence-based practice within the context of evidence-informed practice. Physiotherapy Theory and Practice. 2009b;25(5–6):354–368. doi: 10.1080/09593980902813416. [DOI] [PubMed] [Google Scholar]
- Deyle GD. Direct access physical therapy and diagnostic responsibility: The risk-to-benefit ratio. The Journal of Orthopaedic and Sports Physical Therapy. 2006;36(9):632–634. doi: 10.2519/jospt.2006.0110. [DOI] [PubMed] [Google Scholar]
- Duffy R. 2012. Nurse to educator? Academic roles and the formation of personal academic identities, Nurse Education Today. (Available at: http://dx.doi.org/10.1016/j.nedt.2012.07.020 ) (ahead of print)
- Finlay L. “Outing” the Researcher: The Provenance, Process and Practice of Reflexivity. Qualitative Health Research. 2002;12(4):531–545. doi: 10.1177/104973202129120052. [DOI] [PubMed] [Google Scholar]
- Giacomini M. Interdisciplinarity in health services research: dreams and nightmares, maladies and remedies. Journal of Health Services Research & Policy. 2004;9(3):177–183. doi: 10.1258/1355819041403222. 2004. [DOI] [PubMed] [Google Scholar]
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Education Today. 2004;24:105–112. doi: 10.1016/j.nedt.2003.10.001. [DOI] [PubMed] [Google Scholar]
- Green J, Franquiz M, Dixon C. The myth of the objective transcript. TESOL Quarterly. 1997;31(1):172–176. [Google Scholar]
- Hall P. Interprofessional teamwork: professional culture as barriers. Journal of Interprofessional Care. 2005;19(Suppl 1):188–196. doi: 10.1080/13561820500081745. [DOI] [PubMed] [Google Scholar]
- HRB - Health Research Board. 2010. The Identification of Research Priorities for Therapy Professions in Ireland. (Available at: http://www.hrb.ie/uploads/tx_hrbpublications/Physical_Therapies_Priorities_Summary_Report_01.pdf ) (Accessed 23/9/2010)
- Hsieh HF, Shannon SE. Three Approaches to Qualitative Content Analysis. Qualitative Health Research. 2005;15(9):1277–1288. doi: 10.1177/1049732305276687. [DOI] [PubMed] [Google Scholar]
- Imhof L, Abderhalden C, Cignacco E, Eicher M, Mahrer-Imhof R, Schubert M, Shaha M. Swiss Research Agenda for Nursing (SRAN) Die Entwicklung einer Agenda für die klinische Pflegeforschung in der Schweiz. Pflege. 2008;21:252–261. doi: 10.1024/1012-5302.21.4.252. [DOI] [PubMed] [Google Scholar]
- Kitzinger J. Qualitative research: Introducing focus group. British Medical Journal. 1995;311:299. doi: 10.1136/bmj.311.7000.299. (Available at: http://www.bmj.com/content/311/7000/299.extract (Accessed 8/10/2010) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kitzinger J. Focus group research: using group dynamics to explore perceptions, experiences and understandings. In: Holloway I, editor. Qualitative Research in Health Care. Maidenhead: Open University Press; 2005. pp. 56–70. [Google Scholar]
- Malcolm D, Scott A. Professional relations in sport healthcare: Workplace responses to organisational change. Social Science & Medicine. 2011;72:513–520. doi: 10.1016/j.socscimed.2010.11.016. [DOI] [PubMed] [Google Scholar]
- Merriam SB. Qualitative research and case study applications in education. San Francisco: Jossey-Bass; 1998. [Google Scholar]
- Miles-Tapping C, Dyck A, Brunham S, Simpson E, Barber L. Canadian therapists' priorities for clinical research: A Delphi study. Physical Therapy. 1990;70:448–454. doi: 10.1093/ptj/70.7.448. [DOI] [PubMed] [Google Scholar]
- Mitchell JM, de Lissovoy G. A comparison of resource use and cost in direct access versus physician referral episodes of physical therapy. Physical Therapy. 1997;77:10–18. doi: 10.1093/ptj/77.1.10. [DOI] [PubMed] [Google Scholar]
- Moretti F, van Vliet L, Bensing J, Deledda G, Mazzi M, Rimondini M, Zimmermann C, Fletcher I. A standardized approach to qualitative content analysis of focus group discussions from different countries. Patient Education and Counseling. 2011;82:420–428. doi: 10.1016/j.pec.2011.01.005. [DOI] [PubMed] [Google Scholar]
- Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P. Qualitative research methods in health technology assessment: a review of the literature. Southampton: Health Technology Assessment, NHS R&D HTA Programme, NCCHTA, University of Southampton; 1998. [PubMed] [Google Scholar]
- Physioswiss. 2011. Stratégie du domaine de la communication 2009–2013. (Available at: http://www.physioswiss.ch/download/online/dokkr081005_05_f_Strategie_Kommunikation.pdf (Accessed 9/11/12012)
- Physioswiss. 2013. Members. (Available at: http://www.physioswiss.ch/swiss/verband/mitglieder.htm.
- Ross F, Smith E, Mackenzie A, Masterson A. Identifying research priorities in nursing and midwifery service delivery and organisation: a scoping study. International Journal of Nursing Studies. 2004;41(5):547–558. doi: 10.1016/j.ijnurstu.2003.12.008. [DOI] [PubMed] [Google Scholar]
- Rushton A, Moore A. International identification of research priorities for postgraduate thesis in musculoskeletal physiotherapy using a modified Delphi technique. Manual Therapy. 2010;15(2):142–148. doi: 10.1016/j.math.2009.09.003. [DOI] [PubMed] [Google Scholar]
- Silverman D. Doing qualitative research: A practical handbook. London: Sage; 2005. [Google Scholar]
- Smith S, Roberts P, Balmer S. Role overlap and professional boundaries: Future implications for physiotherapy and occupational therapy in the NHS. Physiotherapy. 2000;86(8):397–400. [Google Scholar]
- Sparkes VJ. Profession and professionalization. Part 1. Physiotherapy. 2002;88(8):481–486. [Google Scholar]
- Stewart RJ, Caird J, Oliver K, Oliver S. Patients’ and clinicians’ research priorities. Health Expectations. 2011;14(4):439–448. doi: 10.1111/j.1369-7625.2010.00648.x. [DOI] [PMC free article] [PubMed] [Google Scholar]