

Abstract
Malignant syphilis is an uncommon manifestation of secondary syphilis, in which necrotic lesions may be associated with systemic signs and symptoms. Generally it occurs in an immunosuppressed patient, mainly HIV-infected, but might be observed on those who have normal immune response. Since there is an exponential increase in the number of syphilis cases, more diagnoses of malignant syphilis must be expected. We report a case in an immunocompetent female patient.
Keywords: Allergy and immunology; Syphilis; Syphilis, cutaneous; Therapeutics; Treatment outcome
INTRODUCTION
Early malignant syphilis is a rare form of secondary syphilis, more frequently associated with HIV - co-infected patients.1,2 Malnutrition, abusive consumption of alcohol and concomitant debilitating illnesses are other possible predisposing factors.1,3,4 More rarely, it can occur in immunocompetent patient. It was first described by Bazin in 1859 (apud Tucker et al. 2009) as a nodular variant of syphilis.5 It is different from classical manifestations of secondary syphilis for its greater severity and lesion morphology. Cutaneous lesions of malignant syphilis are preceded by prodromal fever, cephalalgia, arthralgia and myalgia of variable intensity. They are characterized by the onset of pleomorphic pustules, nodules and ulcers.6 The mucosas may be compromised and the patient may present associated enlargement of lymph nodes and hepatosplenomegaly.
Before the advent of HV infection, malignant syphilis was extremely rare; between 1900 and 1988 only 14 cases had been published in English language literature. At present, it is estimated that up to 7% of syphilis cases in HIV/aids-infected patients meet the criteria for malignant syphilis, and not rarely they are the first clinical manifestation revealing a hidden HIV infection.7
The authors report a case of early malignant syphilis in young immunocompetent patient being monitored for psoriasis vulgaris controlled with topical treatment.
CASE REPORT
A female patient, 29 years old, presented with a two weeks history of a clinical-dermatological picture characterized by the presence of fever, loss of appetite and myalgia, soon followed by the onset of skin lesions like pustules and nodules that progressed to ulcers. Except for psoriasis, she did not present other comorbidities. The physical examination showed that the patient was in apparent satisfactory general condition, afebrile and with multiple lesions as nodules, ulcerated nodules and ulcers, the latter with a necrotic aspect, sometimes covered by scabs. The lesions were mainly located on the face, thorax and upper limbs (Figures 1, 2 and 3). The palms had sparse lesions of small diameter, erythematous, discreetly infiltrated and with a collarette of scales surrounding them. There were no lesions on oral or genital mucosa, but in the perianal region and along the intergluteal cleft a single, longitudinal ulcerated papulonodular lesion could be observed, compatible with a condiloma lata lesion. The ophthalmological and neurological examination did not reveal abnormalities. Serum investigation showed VDRL = 1/256, positive treponemal test and negative serology for HIV, VHB and VHC infection. The histopathological examination of one of the lesions showed epidermal ulceration, presence of hematic crust and dense lichenoid lymphohistiocytic infiltrate rich in plasmocytes, which extended until the deep dermis. The vessels presented endothelial tumefaction with walls permeated by polymor-phonuclear cells and fibrin microthrombi. Anti-Treponema pallidum immunomarking with polyclonal antibody was positive, evidencing numerous spirochetes (Figures 4, 5 and 6).
FIGURE 1.

Malignant syphilis: papulous and ulcerated papulonodular lesions on the face
FIGURE 2.

Malignant syphilis: papulous, ulcerated papulous and ulcerated nodular lesions covered by scab on forearm
FIGURE 3.

Malignant syphilis: detail of papulous and ulcerated nodular lesions
FIGURE 4.
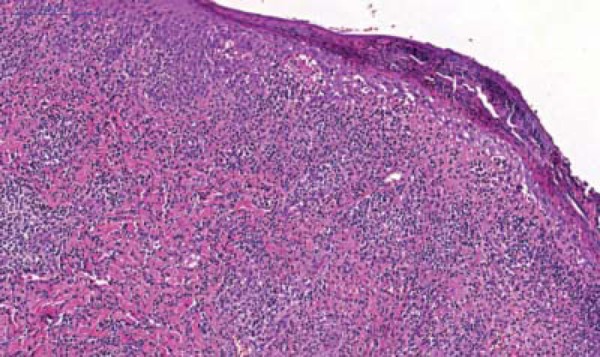
Malignant syphilis: ulcerated lesion with superficial crust and dense lichenoid lymphohistiocytic infiltrate, rich in plasmocytes. HE 10X
FIGURE 5.
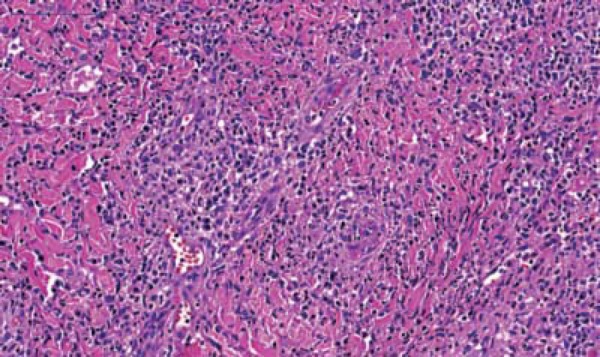
Malignant syphilis: detail of dermal infiltrate and endarteritis with fibrin microthrombi. HE 20X
FIGURE 6.
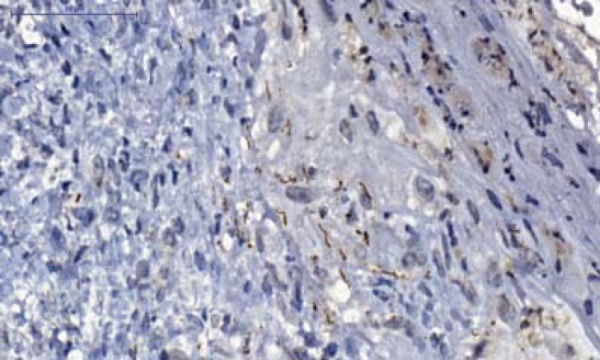
Early malignant syphilis: Treponema pallidum immunomarked with polyclonal antibody. IHQ 60X
The patient was treated with 2.400.000 units of benzathine penicillin, in a total of three series with an interval of one week between the series. She presented intense Jarisch-Herxheimer reaction after the first application of penicillin. Lesion healing was fast and serology showed VDRL titre fell to 1/16 after three months of treatment and negativation after nine months.
DISCUSSION
After the first description in 1859, for many decades doubts remained if malignant syphilis was part of the secondary syphilis spectrum or a manifestation of tertiary syphilis. This issue was clarified by studies conducted by Haslund and Neisser, published in 1897.8,9 Malignant syphilis is distinguished from classical secondary syphilis by the general clinical picture more exuberant and severe, pleomorphic lesions and fundamentally by the presence of ulceronecrotic lesions. It is distinguished from tertiary syphilis by the larger number of lesions, repercussion in the general health condition and for being morphologically distinct from chronic gummas, both clinically and histologically.
Epidemiological data show the recrudescence of syphilis cases, mainly in men who have sex with other men and among HIV-infected patients.10 In Germany it was observed that among 11,368 HIV-infected patients, 151 (1.3%) presented syphilis during follow-up and 11 of them (7.3%) had malignant syphilis.7 These data draw attention to possible higher occurrence of the disease in the different services. A study of 21 cases where the patients were coinfected by HIV showed higher incidence in male patients (62%), median age 34 years and, in 80% of the cases, CD4 count > 200 cells/mm3. In 33% there was ocular involvement and in 24% mucosas were compromised.
Strictly speaking, the pathogenesis of malignant syphilis is unknown, but the prevalent opinion is that in those coinfected by HIV the immunodeficiency favors the predominance of the virulence of the agent in the agent-host contest1 This reasoning is coherent with its occurrence in those who have the abusive use of alcohol or illicit drugs, malnutrition or debilitating disease as a cofactor. The occurrence of malignant syphilis, as in the case described, in immunocompetent patient, raises the possibility, already considered by other authors, of infection by more virulent strains of Treponema , which, although possible, is difficult to be demonstrated.1,2
When there is clinical suspicion of malignant syphilis, confirmation of the diagnosis will be supported by three criteria: clinical and histopathological characteristics; presence of high titre of antibodies in VDRL or a similar test; intense and severe Jarisch-Herxheimer reaction and rapid resolution of lesions with adequate therapy. The investigation of immunodeficiency inducing factor, particularly HIV-infection, is mandatory. The treatment of secondary syphilis, according to the Ministry of Health of Brazil proposal, foresees two series of 2,400,000 U of benzathine penicillin, with an interval of one week between the series.4 There is no mention of the scheme to be used for malignant syphilis and the literature mentions both three and four series regarding the use of crystalline penicillin. Strictly speaking, the definition of the treatment should attend to the coexistence or not of neurosyphilis or syphilitic uveitis. In this studied case, three series of 2,400,000 U of benzathine penicillin were fully effective.
In face of the increased number of syphilis cases, dermatologists and general practitioners should be attentive to the possibility of occurrence of malignant syphilis cases and equally attentive to the intensity of the Jarisch-Herxheimer reaction and for this reason to include antihistaminic drugs or even corticosteroids in the prescription prior to penicillin.
Footnotes
Conflict of Interests: None
Financial Support: None
How to cite this article: Requena CB, Orasmo CR, Ocanha JP, Barraviera SRCS, Marques MEA, Marques SA. Malignant syphilis in an immunocompetent female patient. An Bras Dermatol. 2014;89(6)806-7.
Work carried out at the Department of Dermatology and Radiotherapy - Faculdade de Medicina de Botucatu. Universidade Estadual Paulista "Júlio de Mesquita Filho" (Unesp) - Botucatu (SP), Brazil.
References
- 1.Corti M, Solari R, De Carolis L, Figueiras O, Vittar N, Maronna E. Sífilis maligna en un paciente con infección por VIH. Presentación de un caso y revisión de la literatura. Rev Chilena Infectol. 2012;29:678–681. doi: 10.4067/S0716-10182012000700017. [DOI] [PubMed] [Google Scholar]
- 2.Watson KM, White JM, Salisbury JR, Creamer D. Lues maligna. Clin Exp Dermatol. 2004;29:625–627. doi: 10.1111/j.1365-2230.2004.01630.x. [DOI] [PubMed] [Google Scholar]
- 3.Belda W, Jr, Dias MC, Zolli CA, Santos Junior MFQ, Siqueira LFG. Sífilis maligna precoce: a propósito de um caso. An Bras Dermatol. 1990;65:147–150. [Google Scholar]
- 4.Avelleira JCR, Rangel GCB. Syphilis: diagnosis, treatment and control. An Bras Dermatol. 2006;81:111–126. [Google Scholar]
- 5.Tucker JD, Shah S, Jarell AD, Tsai KY, Zembowicz A, Kroshinsky D. Lues maligna in early HIV infection case report and review of the literature. Sex Transm Dis. 2009;36:512–514. doi: 10.1097/OLQ.0b013e3181a2a946. [DOI] [PubMed] [Google Scholar]
- 6.Passoni LF, de Menezes JA, Ribeiro SR, Sampaio EC. Lues maligna in an HIV-infected patient. Rev Soc Bras Med Trop. 2005;38:181–184. doi: 10.1590/s0037-86822005000200011. [DOI] [PubMed] [Google Scholar]
- 7.Schöfer H, Imhof M, Thoma-Greber E, Brockmeyer NH, Hartmann M, Gerken G, et al. Active syphilis in HIV infection: a multicentre retrospective survey. Genitourin Med. 1996;72:176–181. doi: 10.1136/sti.72.3.176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Haslund A. Syphilis maligna. Arch Dermatol Syph. 1897;38:345–392. [Google Scholar]
- 9.Neisser A. Malignant syphilis. Br J Dermatol. 1897;9:11–26. [Google Scholar]
- 10.Pathela P, Braunstein SL, Schillinger JA, Shepard C, Sweeney M, Blank S. Men who have sex with men have a 140-fold higher risk for newly diagnosed HIV and syphilis compared with heterosexual men in New York City. J Acquir Immune Defic Syndr. 2011;58:408–416. doi: 10.1097/QAI.0b013e318230e1ca. [DOI] [PubMed] [Google Scholar]