

Abstract
Objectives
The number of healthcare institutions adopting smartphones continues to increase, implying that their utilization is undoubtedly gaining attention. Understanding the needs of smartphone users will provide a greater opportunity for successful information technology acceptance by expanding the scope of its utilization. This study focuses on how smartphones are accepted and utilized in hospitals and analyzes the factors influencing users' attitude, social influence, and intention of use.
Methods
For the study model, the researcher has mainly adopted the Theory of Reasoned Action and further modified and used the models of Technology Acceptance and Information Systems Success. To test the model empirically, a survey was conducted with 122 professionals on information development teams in Korean tertiary hospitals.
Results
The common smartphone usage modes were Internet searching, e-mail, scheduling, and social networking in consecutive order. Phone calls consisted of 51.4% of work-related purposes, while other functions, such as text message, Web browser, and scheduling, were mostly used for personal purposes. Costs, contents quality, innovation, ease of use, and support were shown to have statistically significant effects on user attitude, and social influence, portability, security, content quality, and innovation were significant. User attitude and social influence were both statistically significant with respect to intention of use, with user attitude greater than social influence.
Conclusions
The participating staff were analyzed as having strong personal faith and principles, independent from their external environment. Timely information exchanges among medical staff will facilitate appropriate communication and improved health services to patients in need.
Keywords: Mobile Phone, Telecommunications, Wireless Technology, Health Information Management, Consumer Health Information
I. Introduction
Today we live in an information society that creates and transfers various types of information. Everyday tasks are completed efficiently and effectively using computers and communication devices. Information systems are being used to further achieve organizational goals, such as decreasing costs, developing new products, expanding businesses, furthering research and development, and providing better services.
The information technology paradigm is shifting to a 'ubiquitous environment' that enables real-time data exchange [1]. A ubiquitous society can interact with personalized information by applying technology, such as wireless integration, mobile convergence, and radio-frequency identification [2]. The information super highway and mobile devices are rapidly converging at this time into this ubiquitous environment. In 10-20 years, this technology will lead a large-scale societal change [3].
Personal device tastes are also shifting from personal digital assistants (PDAs) and laptops to a wide variety of smartphones and tablets. In particular, smartphones have been one of the success stories of the last decade. In a relatively short period of time, smartphone technology has significantly penetrated society, reaching subscribers in Western industrialized nations from school children to senior citizens. Smartphones are the latest evolution in a long history of communication devices, leading to a rapid adoption of mobile communication devices starting in the latter part of the last century [4]. Gartner, an IT research organization, predicts that 80% of businesses will support a workforce using tablets by 2013, and 90% of organizations will support corporate applications on personal devices by 2014 [5].
Therefore, smartphones are changing many industries, including the medical industry. Mobile devices are increasingly used in healthcare industries with more sophisticated treatment and diagnosis, improved financial regulation, and larger volumes of information. Information technology in healthcare provides clinicians with information and tools, such as clinical decision support that can improve the quality of care and reduce potential medical errors [6]. More hospitals are applying PDAs and smartphones for medical professional roles, since mobile devices have been recognized as effective tools. This trend inevitably indicates how important smartphones have already become to the everyday lives of doctors and other clinicians. Smartphone applications can be innovative tools in doctors' pockets, offering ample opportunities through the increasing demand for information to improve the quality of care and patient safety. Further comprehensive analyses of usage patterns would lead to customized applications and services that meet user requirements and are better used at points of care [7].
Recently, many academic medical centers and hospitals have begun to distribute smartphones to physicians and other healthcare professionals. For instance, the University of Pittsburgh Medical Center distributed smartphones to doctors and nurses in some of its emergency rooms and surgical floors [8,9]. Through continued investment in mobile healthcare, information technology has gained widespread acceptance in the Korean medical service through smart terminals, such as smartphones or tablet computers [10]. Medical staff and patients can use smartphones to effectively input information and efficiently view lab results. Smartphone applications can also diminish patient waiting times by providing online registration, payment, and medical information. In addition, mobile Electronic Medical Record systems now allow medical staff to access comprehensive patient information, including his or her medicine administration status, diet, vital signs, X-ray and computed tomography interpretations, and other basic information through a mobile device [10].
Medical staff can assist homebound or preoccupied patients using smartphones, providing check-ups, schedule management, and test results. Information technology also permits remote access to hospital databases, allowing for the exchange of data during business hours and the improvement of doctors' work.
The purpose of this study is to analyze and determine factors that influence the application of smartphones to hospitals. Smartphone application status, application problems, and the influence factor on hospital applications will be investigated. Specifically, this study aims to examine smartphone application status at hospitals, show acceptability factors by analyzing smartphone acceptance at hospitals, and suggest successful guidance for smartphone application and user acceptance at hospitals.
II. Methods
1. Research Model
The theoretical background of this study focuses on the Theory of Reasoned Action (TRA) by Fishbein and Ajzen [11] to analyze the influence of smartphones at tertiary hospitals. This study also applies the Technology Acceptance Model (TAM) by Davis et al. [12], which is a modified version of the TRA and the Information Systems (IS) Success Model by DeLone and McLean [13,14]. Based on the accumulated knowledge from Kim and Chang [15] and Chang [16], the research model was derived as is shown in Figure 1 from modifying properties to reflect the characteristics and environments of smartphones.
Figure 1.

Research model.
2. Data Collection
The research subjects of this study were medical staff from two tertiary hospitals, which use smartphones at work. A self-administered questionnaire was distributed to 400 employees in November 2010, and 36.3% (145) were returned during a 3-week period. After discarding 16 surveys of participants who did not use a smartphone and 7 surveys with incomplete answers, a total of 122 surveys were analyzed.
3. Survey Instrument
The survey was developed from literature review and face-to-face interviews with directors of the hospital departments of information technology and management. The survey consisted of 61 total questions: 4 questions on smartphone use status; a question set on smartphone awareness that included 7 questions on devices, 3 questions on costs, 4 questions on portability, 6 questions on contents quality, 4 questions on social influence, and 5 questions on user innovation; and a question set about smartphones usage awareness with 5 questions on usefulness, 6 questions on support, 4 questions on attitude, 3 questions on purpose of use, and 5 questions on demographic characteristics. Survey responses were recorded on a 7-point Likert scale, with 1 being 'strongly disagree' and 7 being 'strongly agree', except for the questions with respect to the awareness of smartphones and their use.
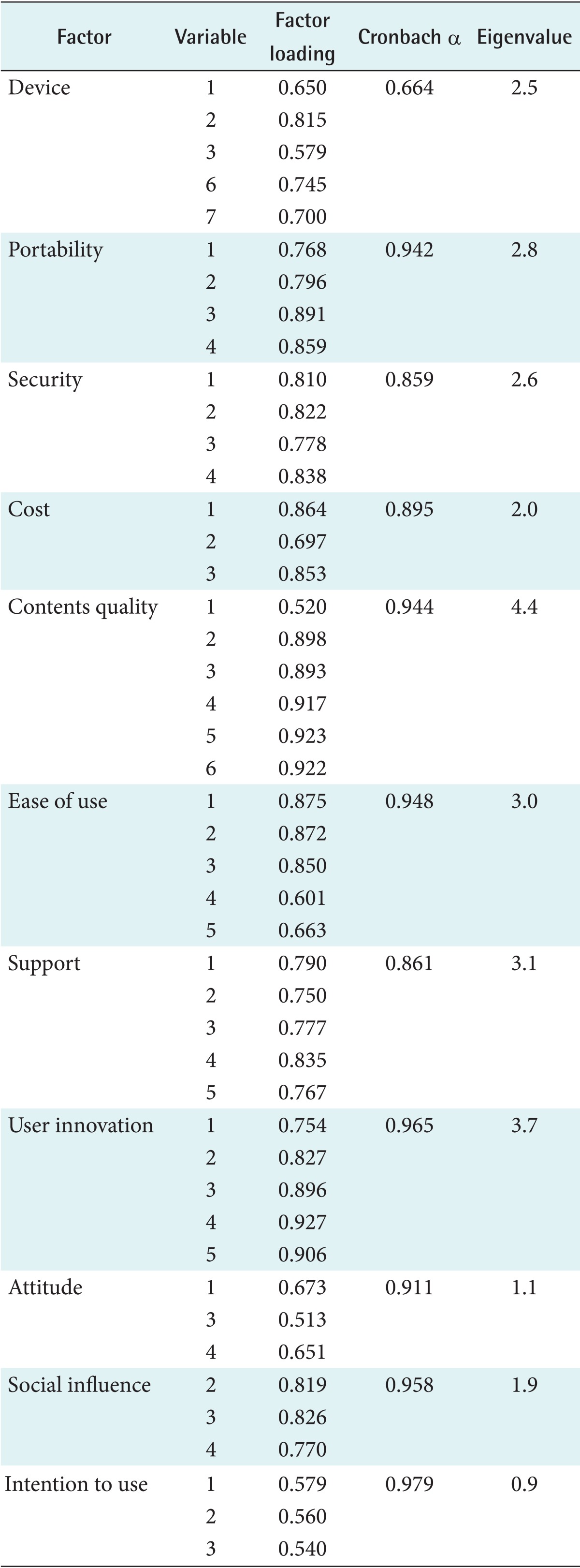
Reliability and validity tests were conducted for the developed survey instrument. Cronbach's α was analyzed to measure internal reliability, and factor analysis and principal component analysis were conducted as validity tests. As shown in Table 1, the alpha values were 0.86-0.98, which reflects high internal consistency in the scaled results, except questions on devices. Ten factors had an eigenvalue greater than 1.0, and 85.53% of the variance was accounted for by the model, which shows high explanation and validity. Moreover, the factor loading value, which explains correlation between the measurement variables, was over 0.50 for each of the factors shown. Based on the analyses, two factors from devices, one factor from portability, one factor from portability, one factor from support, one factor from attitude, and one factor from social influence were removed.
Table 1.
Results of reliability and validity tests
4. Analysis Method
Descriptive statistics and frequencies were computed for subjects' characteristics and their status of smartphone purchase and use. According to the research model, statistical significances were tested using multiple regression analyses by generating equations to describe the statistical relationship between influential factors and response variables, such as user attitude, social influence, and intention of use. Explicitly, the independent variables consisted of device, cost, portability, security, contents quality, innovation, ease of use, and support, while attitude, social influence, and intention to use were dependent variables. In general, the significance was tested at the alpha level of 0.05.
III. Results
1. Characteristics of Respondents
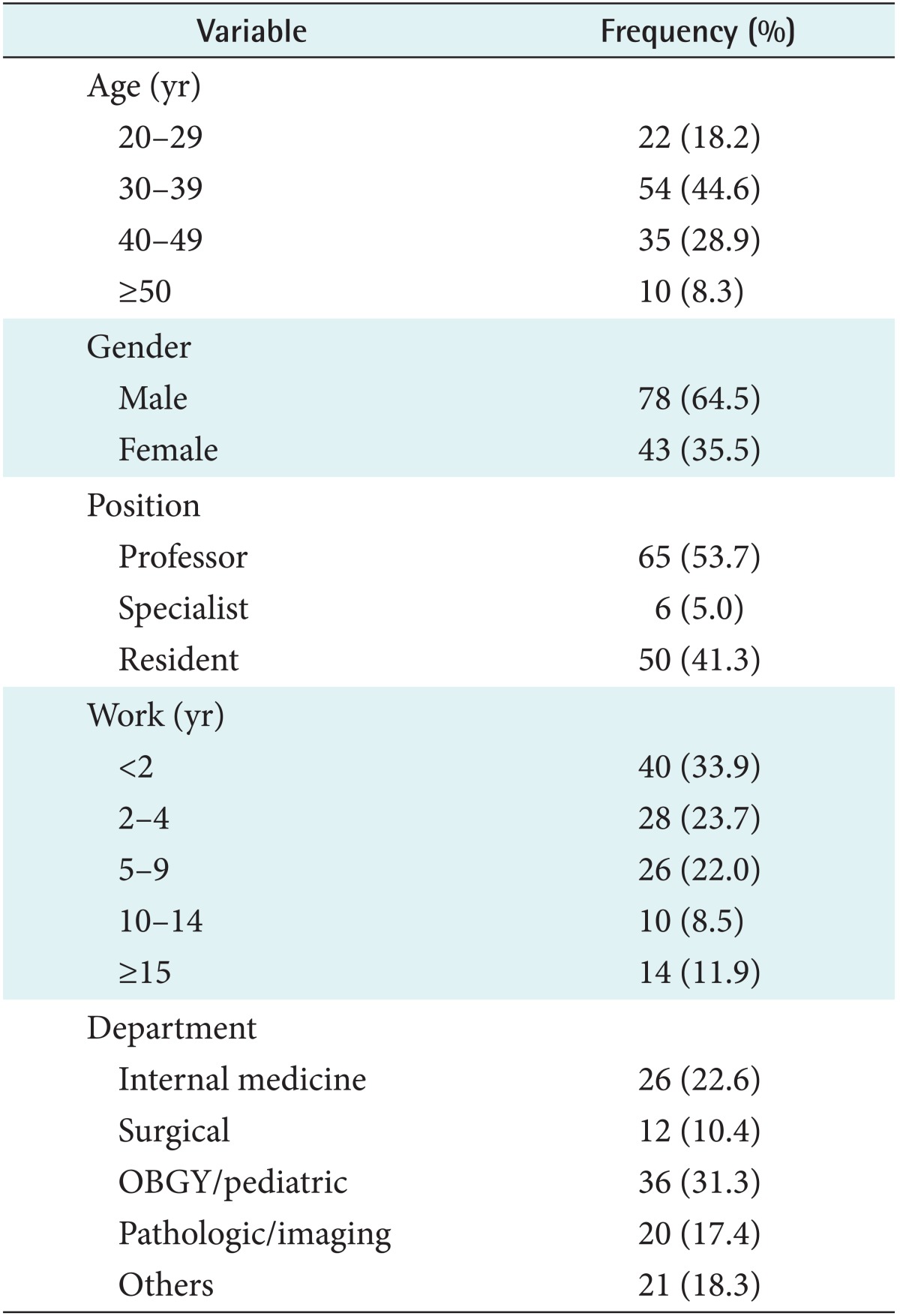
The general characteristics of the sample group were analyzed using descriptive statistics. The resulting demographic characteristics are shown in Table 2. Seventy-eight (64.5%) respondents were male and 43 (35.5%) were female. The age distribution of respondents consisted of 54 (44.6%) in their 30s, 35 (28.9%) in their 40s, 22 (18.2%) in their 20s, and 10 (8.3%) in their 50s, respectively. With respect to professions, 65 (53.7%) of the respondents were professors, 50 (41.3%) residents, and 6 (5%) specialists. Users' departments were concentrated in gynecology & pediatrics (31.3%) and internal medicine related departments (22.6%), with other departments (18.3%), pathology/radiology (17.4%), and surgical (10.4%) in consecutive order.
Table 2.
Subject characteristics
2. Status of Smartphone Purchase and Contract
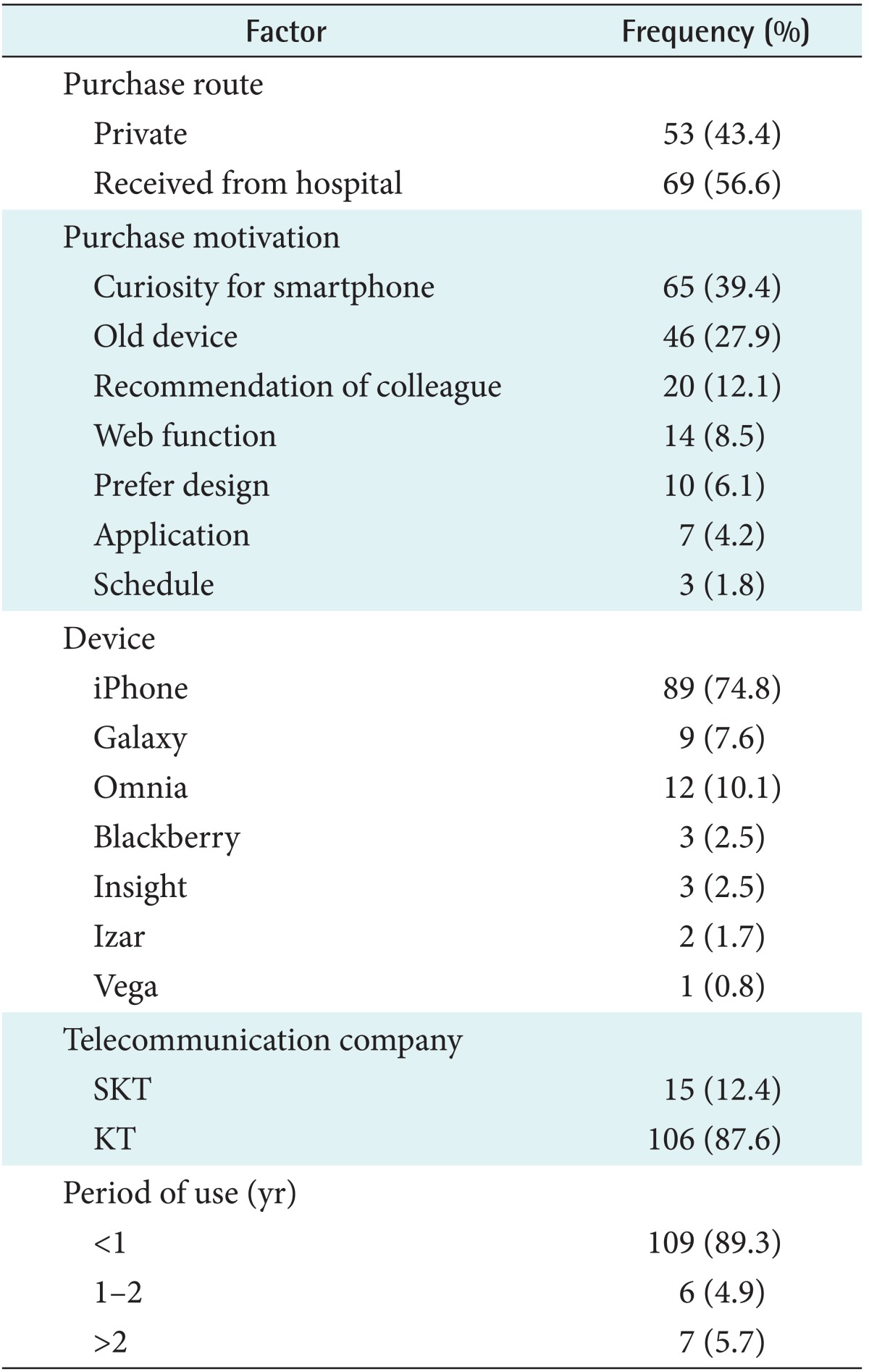
As is shown below in Table 3, 53 (43.4%) survey respondents personally purchased their device, with hospital-given smartphones making up the balance (56.6%). Respondents purchased smartphones for curiosity (65), as an upgraded device (46), from the recommendations of an acquaintance (20), for convenient internet use (14), for their design (10), applications (7), and scheduling (3). The majority of respondents used the iPhone (74.8%), followed by the Omnia, Galaxy S, BlackBerry, LG Insight, Izar, and Vega in descending order. One hundred six respondents (87.6%) subscribed to Korea Telecom (KT) and 15 (21.4%) were using SK Telecom (SKT). Most of the respondents (89.3%) had been using their smartphones for less than a year.
Table 3.
Status of smartphone purchase
Most respondents were unaware of the exact smartphone purchase price because they obtained the device under a 1- to 3-year service plan with an account transfer. Therefore, the average smartphone cost was calculated based on the purchase price and Internet service costs. The average price was $287.8 for self-purchased devices and $276.7 for hospital-purchased devices. Over 90% of the respondents bought their smartphones on a 2-year contract. The monthly wireless plan fee averaged $51.6 for individuals and $13.8 for hospitals, as is shown below in Table 4.
Table 4.
Costs of smartphone and its use (unit: US dollar)

3. Smartphone Usage
As shown in Figure 2, the most common smartphone usage mode was internet searching with 101 responses (82.8%), e-mail with 94 responses (76.2%), and scheduling with 78 responses (63.9%). Other uses included social networking with 43 responses (35.2%), staff information queries with 25 responses (20.5%), groupware (electronic transfers and hospital mail) with 11 respondents (9.0%), and drug information queries with 9 responses (7.4%). The uses below 5% were medical record search, picture archiving and communication system (PACS), task reporting, in-hospital calls, and games. Regular phone calls consisted of 51.4% for work-related purposes and 48.6% for private purposes, as shown in Figure 3. For text messages, 37.5% were for work purposes and 62.5% were for personal purposes. Web browser use was 21.9% for work purposes and 78.1% for personal purposes. Scheduling, photo viewing, and movies were also concentrated for personal purposes (61.3%).
Figure 2.

Proportion of smartphone usage mode. SNS: social network service, PACS: picture archiving and communication system.
Figure 3.

Proportion of official smartphone use. SMS: short message service.
4. Multiple Regression Analysis
Tables 5 and 6 show the results of multiple regression analyses, which include the parameter estimates and their significance of relationship between predictor and response variable. The p-value for each term tests the null hypothesis that the coefficient is equal to zero, which means no effect. In the model of attitude, cost (p = 0.000), quality (p = 0.000), innovation (p = 0.000), ease of use (p = 0.006), and support (p = 0.031) were statistically significant, but device, portability, security were not associated with attitude (p > 0.05). In the model of social influence, security (p = 0.000), innovation (p = 0.000), contents quality (p = 0.029), and portability (p = 0.044) were statistically significant, but device, cost, ease of use, and support were not associated with social influence (p > 0.05). In the additional model for intention to use, the relative significance of attitude and social influence was tested (Table 6). The p-values were 0.000 and 0.005 for attitude and social influence, respectively. Although both predictors were significant at 0.05, users' attitude mattered more than social influence with respect to intention to use smartphone, comparing standardized coefficients (0.598 vs. 0.209). The overall results of significant relationships were summarized in Figure 4. The characteristics of the device influenced neither attitude nor social influence.
Table 5.
Multiple regression results of factors influencing attitude and social influence
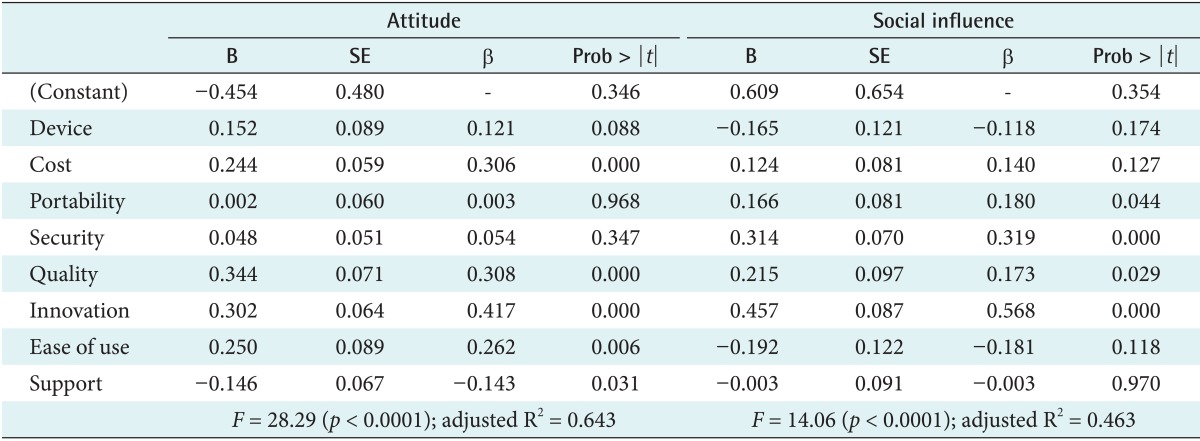
B is the unstandardized regression coefficient, β is the standardized regression coefficient.
Table 6.
Multiple regression results of attitude and social influence on intention to use
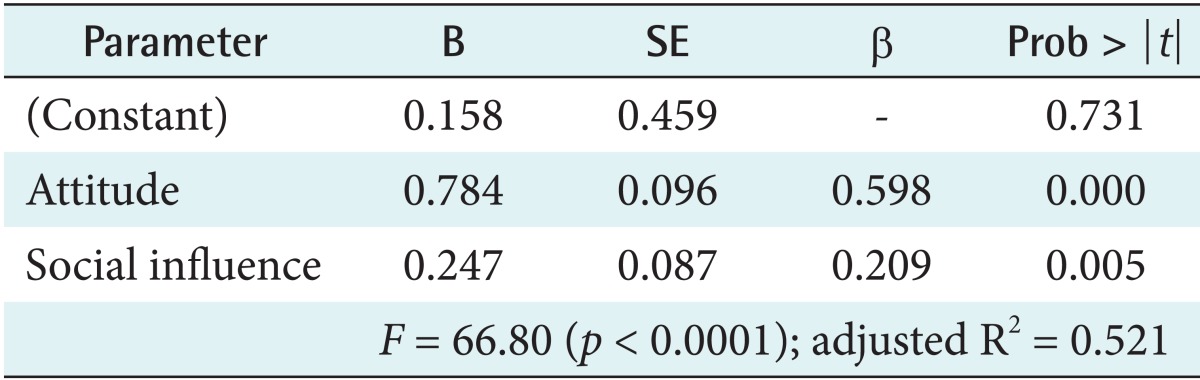
B is the unstandardized regression coefficient, β is the standardized regression coefficient.
Figure 4.

Test results of the research model.
IV. Discussion
Many people and organizations today use mobile wireless technology via wireless application protocol (WAP) phones, handheld devices, smartphones, wireless laptops, mobile commerce, and other portable devices. However, despite this market's growth, research examining the key factors affecting user behavior and mobile adoption is scarce [17]. Therefore, this research focused on factors that affect users' intentions when adopting smartphones at medical institutions. Tertiary hospitals were selected for this study over primary and secondary hospitals because they adopted smartphones faster and currently utilize them.
Even though younger groups adopt IT technology more quickly than older groups in hospitals [18], smartphone use in the hospitals studied was mostly due to medical staff professors, since the hospital provided smartphones to them first. Estimates project that younger groups in hospitals will use smartphones for medical purposes more than older groups in the near future.
Current users tend to use smartphones for Web services, such as Internet searches and e-mail, but were able to use the full functionality of smartphones by also including scheduling, social networking, staff information inquiries, drug information inquiries, diagnosis information inquiries, PACS, and in-company calls. Since smartphone adoption is still in its early stages at hospitals, education, infrastructure expansion and medical software applications will increase smartphone use. In addition, smartphones could potentially be used in emergency settings to document injuries or lesions [19].
As was shown in the results section, costs, contents quality, innovation, ease of use, and support affected user attitude while device, portability and security were insignificant, since medical doctors were unaware of smartphones' usefulness in providing accurate information at their current stage. Developers should develop and upgrade their contents for accuracy, promptness, usefulness, and individual suitability for smartphone usage.
Also, the research did not show a significant influence on user attitude, but after hospitals expand the scope of smartphone use, device input, resolution, and size are expected to play a more important role in actual use. The hardware and software functionality of the devices should be improved to expand smartphone use.
After looking over the factors studied, this study found that portability, security, contents quality, and innovation significantly affect the social influence of smartphones. Such factors are equally important in other industries. Exchanging information and enhancing communication will promote a timely and high-quality diagnosis on patients. Security systems should also be developed to protect medical information. In case smartphones are lost or stolen, an independent security system should be used over wireless control to prevent the theft of patients' medical records.
Finally, user attitude influenced the intention to use a smartphone more than social influences within the subject group. Medical doctors who participated in the survey are more likely to rely on their beliefs than peer pressure from their environment. However, the findings of this study need to be further investigated in specific subgroups and/or processes. For example, Ismail et al. [18] showed that the younger generations and females reported better acceptance of smartphone use in their work, and Takao et al. [20] recommended a new support system using a smartphone for diagnostic image display and treatment of stroke.
This research has many implications when compared to earlier research. Lee et al. [21] divided organization characteristics into technical support and education, and both factors positively affected actual use. The results of this research also show that support factors have a significant influence on user attitude. Supporting users is an important aspect of technology adoption. Educating smartphone users and solving their inconveniences would positively affect user intention by increasing accessibility.
Oliva et al. [22] mentioned that user satisfaction directly affects repurchase because positive attitudes lead to continued smartphone purchases. In this research, user attitude was also found to influence the intention to adopt smartphones. The intention to use smartphones would obviously be higher if the user's attitude is more positive.
Ajzen [23] mentioned in the Theory of Reasoned Action (TRA) [11] that attitude, standards, and behavior control will affect product and service use, and this will make users utilize actual products and services. Also, Kim and Kim [24] suggested a theoretical model about the effect on mobile wireless Internet use from recognized value and use intention. They verified that ease of use, usability, system quality, and instant connectivity affected actual use. As these results also showed that user attitude and social influence affect actual smartphone use intention based on the Theory of Reasoned Action (TRA), this research verified that the awareness of the user and surrounding people affects the actual intention to use a technology.
Despite the suggested implications, additional study is needed to address the limitations of this research. Testing research relationships across multiple hospitals would generalize the smartphone study among healthcare professionals [25]. To generalize the results of this study, the subject group should be expanded and the subject groups should be subdivided more finely.
After smartphones become more available in hospitals, further studies, such as the effect of smartphones on hospital performance and the suitability of smartphones for hospital work, would be important to research. In addition, the further study would focus on the influence of smartphones on the quality of work outcome and performance.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Lee Y, Chang H. Ubiquitous health in Korea: progress, barriers, and prospects. Healthc Inform Res. 2012;18(4):242–251. doi: 10.4258/hir.2012.18.4.242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bae JK, Jeong HM. An empirical study on the determinants factors by including functional attributes of smart phone adoption. e-Business Stud. 2008;9(4):337–361. [Google Scholar]
- 3.Ministry of Public Administration and Security. 2011 National informatization white paper. Seoul, Korea: Ministry of Public Administration and Security; 2011. [Google Scholar]
- 4.Boulos MN, Wheeler S, Tavares C, Jones R. How smartphones are changing the face of mobile and participatory healthcare: an overview, with example from eCAALYX. Biomed Eng Online. 2011;10:24. doi: 10.1186/1475-925X-10-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gartner. Gartner top end-user predicts 2011: Gartner's top predictions for IT organizations and users, 2011 and beyond: it's growing transparency [Internet] Stamford (CT): Gartner; c2010. [cited at 2014 Oct 1]. Available from: http://www.brittenford.com/documents/products/Gartner%20Predicts2011_IT_Transparency.pdf. [Google Scholar]
- 6.Putzer GJ, Park Y. The effects of innovation factors on smartphone adoption among nurses in community hospitals. Perspect Health Inf Manag. 2010;7:1b. [PMC free article] [PubMed] [Google Scholar]
- 7.Nolan T. A smarter way to practise. BMJ. 2011;342:d1124. doi: 10.1136/bmj.d1124. [DOI] [PubMed] [Google Scholar]
- 8.Putzer GJ, Park Y. Are physicians likely to adopt emerging mobile technologies? Attitudes and innovation factors affecting smartphone use in the Southeastern United States. Perspect Health Inf Manag. 2012;9:1b. [PMC free article] [PubMed] [Google Scholar]
- 9.Sheth N, Kane YI. Smart-phone makers call the doctor [Internet] New York (NY): Wall Street Journal; 2009. [cited at 2014 Oct 1]. Available from: http://online.wsj.com/news/articles/SB125487806705169673?mod=_newsreel_4. [Google Scholar]
- 10.Yeo K, Lee K, Kim JM, Kim TH, Choi YH, Jeong WJ, et al. Pitfalls and Security Measures for the Mobile EMR System in Medical Facilities. Healthc Inform Res. 2012;18(2):125–135. doi: 10.4258/hir.2012.18.2.125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fishbein M, Ajzen I. Belief, attitude, intention and behavior: an introduction to theory and research. Reading (MA): Addison-Wesley; 1975. [Google Scholar]
- 12.Davis FD, Bagozzi RP, Warshaw PR. User acceptance of computer technology: a comparison of two theoretical models. Manag Sci. 1989;35(8):982–1003. [Google Scholar]
- 13.Delone WH, McLean ER. Information system success: the quest for the dependent variable. Inf Syst Res. 1992;3(1):60–95. [Google Scholar]
- 14.DeLone WH, McLean ER. The DeLone and McLean Model of information systems success: a ten-year update. J Manag Inf Syst. 2003;19(4):9–30. [Google Scholar]
- 15.Kim D, Chang H. Key functional characteristics in designing and operating health information websites for user satisfaction: an application of the extended technology acceptance model. Int J Med Inform. 2007;76(11-12):790–800. doi: 10.1016/j.ijmedinf.2006.09.001. [DOI] [PubMed] [Google Scholar]
- 16.Chang H. Application of the extended technology acceptance model to picture archiving and communication systems in dental hospitals. J Korean Soc Med Inform. 2009;15(3):265–272. [Google Scholar]
- 17.Kim SH. Moderating effects of job relevance and experience on mobile wireless technology acceptance: adoption of a smartphone by individuals. Inf Manag. 2008;45(6):387–393. [Google Scholar]
- 18.Ismail WK, Kit PC, Buhari N, Muzaini A. Acceptance of smartphone in enhancing patient-caregivers relationship. J Technol Manag Innov. 2012;7(3):71–79. [Google Scholar]
- 19.Choi JS, Yi B, Park JH, Choi K, Jung J, Park SW, Rhee PL. The uses of the smartphone for doctors: an empirical study from Samsung Medical Center. Healthc Inform Res. 2011;17(2):131–138. doi: 10.4258/hir.2011.17.2.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Takao H, Murayama Y, Ishibashi T, Karagiozov KL, Abe T. A new support system using a mobile device (smartphone) for diagnostic image display and treatment of stroke. Stroke. 2012;43(1):236–239. doi: 10.1161/STROKEAHA.111.627943. [DOI] [PubMed] [Google Scholar]
- 21.Lee JO, Whang J, Kang S, Lee S. Extended TAM for accepting mobile devices including functional attributes: the case of cellular phone. J Inf Technol Appl Manag. 2006;13(1):39–66. [Google Scholar]
- 22.Oliva TA, Oliver RL, MacMillan IC. A catastrophe model for developing service satisfaction strategies. J Mark. 1992;56(3):83–95. [Google Scholar]
- 23.Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. [Google Scholar]
- 24.Kim H, Kim J. An empirical research on important factors of mobile internet usage. J MIS Res. 2002;12(3):89–113. [Google Scholar]
- 25.Park Y, Chen JV. Acceptance and adoption of the innovative use of smartphone. Ind Manag Data Syst. 2007;107(9):1349–1365. [Google Scholar]