

Abstract
Clearance of cervical spine injury (CSI) in the obtunded or comatose blunt trauma patient remains controversial. In patients with unreliable physical examination and no evidence of CSI on computed tomography (CT), magnetic resonance imaging of the cervical spine (CS-MRI) is the typical follow-up study. There is a growing body of evidence suggesting that CS-MRI is unnecessary with negative findings on a multi-detector CT (MDCT) scan. This review article systematically analyzes current literature to address the controversies surrounding clearance of CSI in obtunded blunt trauma patients. A literature search through MEDLINE database was conducted using all databases on the National Center for Biotechnology Information (NCBI) website (www.ncbi.nlm.nih.gov) for keywords: “cervical spine injury,” “obtunded,” and “MRI.” The search was limited to studies published within the last 10 years and with populations of patients older than 18 years old. Eleven studies were included in the analysis yielding data on 1535 patients. CS-MRI detected abnormalities in 256 patients (16.6%). The abnormalities reported on CS-MRI resulted in prolonged rigid c-collar immobilization in 74 patients (4.9%). Eleven patients (0.7%) had unstable injury detected on CS-MRI alone that required surgical intervention. In the obtunded blunt trauma patient with unreliable clinical examination and a normal CT scan, there is still a role for CS-MRI in detecting clinically significant injuries when MRI resources are available. However, when a reliable clinical exam reveals intact gross motor function, CS-MRI may be unnecessary.
Keywords: Blunt trauma, cervical spine CT and MRI, obtunded
INTRODUCTION
There is no universally accepted algorithm to clear the cervical spine in an obtunded or comatose blunt trauma patient without apparent neurological deficit. Clinical practice guidelines are left to the discretion of each institution by the Eastern Association for the Surgery of Trauma (EAST).[1] In patients with negative computed tomographic (CT) imaging of the cervical spine (CS) and unreliable physical examinations, magnetic resonance imaging (MRI) to evaluate potential ligamentous injury is the imaging modality of choice.[1,2] However, there is controversy on the use of MRI in the setting of normal findings on multi-detector CT (MDCT) scan in this patient population. While some authors advocate the routine use of MRI in addition to MDCT scan for the clearance of CS in obtunded patients,[3,4,5,6] other practitioners suggest that MRI in the setting of normal findings on MDCT scan is unnecessary.[7,8,9,10,11,12,13,14,15,16] The practice dilemma lies in the idea that the devastating effect of a missed CS injury may outweigh the costs and risks associated with subjecting an obtunded patient to MRI evaluation. In the United States, high healthcare costs and increasing fiscal constraints have prompted re-evaluation of the utilization of expensive practices such as MRI. Across the globe, traumatic injury continues to carry substantial public health costs and MRI is frequently not an option due to its cost or availability. On the other hand, CS immobilization is not without risks; complications related to CS immobilization occurred in 64% of obtunded patients cared for using a strict evaluation protocol utilizing MRI in one study.[16] These risks include decubitus ulcers, dysphagia, discomfort, impaired mobility, respiratory difficulties, and elevations in intracranial pressure.
The purpose of this review article is to systematically analyze clinical studies evaluating the use of MRI in the setting of a normal CS-CT in obtunded blunt trauma patients. Our primary aim was to propose an algorithm for CS clearance in the obtunded blunt trauma patient. As CT and MRI data resolution and image quality have improved significantly over the past decade, the studies evaluated are limited to the last ten years (the period between 2003 and 2013).
MATERIALS AND METHODS
Eligibility criteria
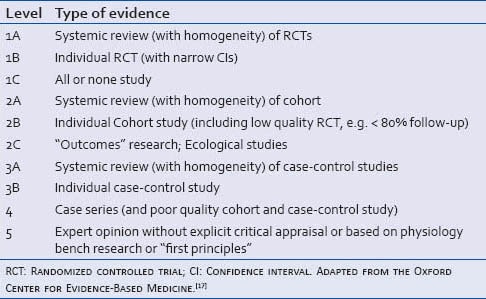
All studies written in the English language with the following patient criteria were included: Adults greater than 18 years of age who had sustained blunt trauma, were obtunded or comatose, had unreliable physical examination, had a negative cervical spine CT and underwent MRI evaluation. Studies in the pediatric population or studies with awake, alert patients with negative CT who underwent MRI due to persistent cervical spine tenderness were excluded. Studies were classified according to levels of evidence for therapeutic studies adapted from the Center for Evidence-Based Medicine [Table 1].
Table 1.
Levels of evidence applied to individual studies
Information sources
A literature search of the National Library of Medicine and the National Institutes of Health MEDLINE database was conducted using all databases on the National Center for Biotechnology Information (NCBI) website (www.ncbi.nlm.nih.gov) and by scanning through the reference lists of articles retrieved.
Search
Keywords used to search all databases were: “Cervical spine injury,” “obtunded,” and “MRI.” Limitations were applied to the English language, studies conducted within the last 10 years, and adults older than 18 years of age.
Study selection
Article selection was conducted by the authors based on our eligibility criteria discussed above.
Data collection process and items
From the selected studies, data were extracted primarily by the first author and reviewed by all authors; disagreements were resolved by discussion between the authors. The following information was extracted from all studies: Number of patients, radiology findings, method of treatment based on radiology findings, and patient outcomes.
Summary measures
The principal summary measure was any significant devastating MRI finding that was missed on CS-CT.
RESULTS
Study selection
The search yielded 44 PubMed scientific and medical abstracts, 83 PubMed Central full text journal articles, 5 book reports and 5 PubMed health clinical effectiveness, disease and drug report for a total of 137 articles [Figure 1]. Limitations of the 137 articles to publication date within the last 10 years and/or adult population and the English language resulted in 63 articles. Eleven of these articles met the inclusion criteria, yielding data on a total of 1,535 patients [Figure 2]. Descriptions of the 11 studies are listed in Tables 2 and 3.
Figure 1.
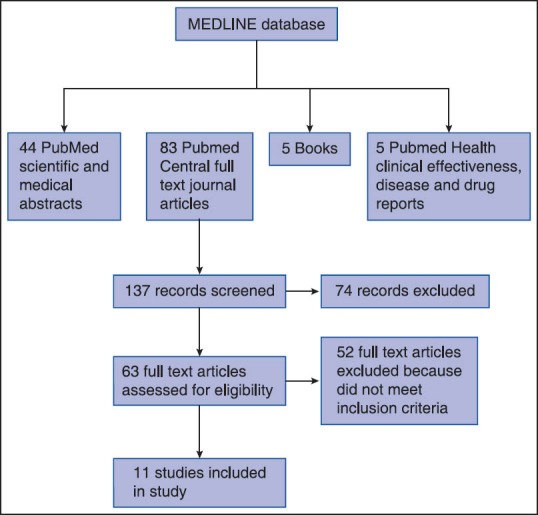
Methodology for identification of relevant quality studies
Figure 2.
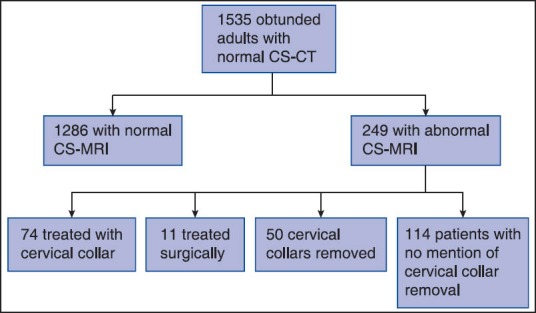
Evaluations, results, and interventions in included patients. CS-CT: Cervical spine computed tomography; CS-MRI: Cervical spine magnetic resonance imaging
Table 2.
The included studies, their types, levels of evidence, and summaries of conclusions
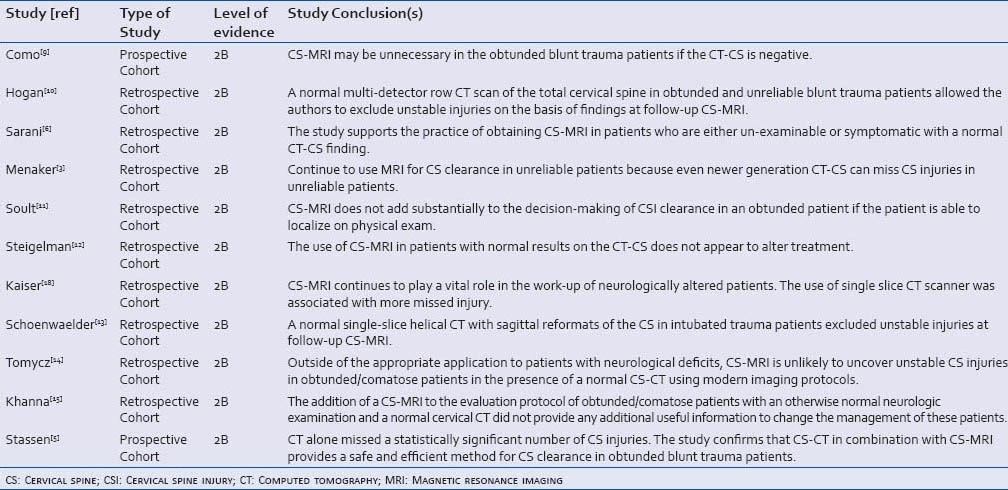
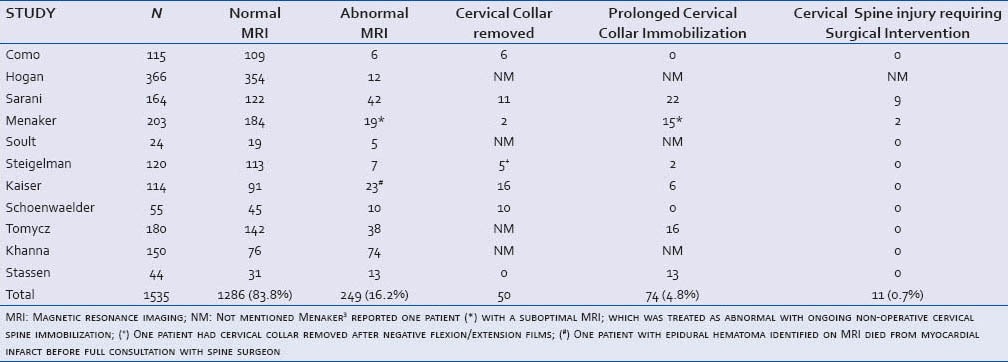
Table 3.
Individual and overall study results
Synthesis of results
Each of the 1,535 patients had a negative CS-CT and was subsequently evaluated with CS-MRI. One thousand two hundred and eighty-six patients out of the 1535 (83.8%) had normal MRI findings. CS-MRI detected abnormalities in the remaining 249 (16.2%), including one exam that was reported as suboptimal but treated as abnormal.[3] The strategy of maintaining cervical collar placement as a precautionary measure with no major change in management was selected in 74 of these 249 patients (29.6%); 11 patients out of the 249 with abnormal CS-MRI (4.3%, 0.7% of the total 1543 patients) were found to have an unstable CS injury on CS-MRI, and all underwent surgical intervention. Fifty patients had their cervical collar removed after CS-MRI; no mention of cervical collar removal was mentioned in the remaining 114 patients [Table 3 and Figure 2].
DISCUSSION
As criteria for clinical assessment of potential CS injury continue to evolve, there continues to be lack of consensus regarding the evaluation of a patient with an unreliable physical examination. The obtunded patient population is more vulnerable to the risks of unindicated imaging, procedures, and orthotic immobilization due to the inability to clinically evaluate their CS for a prolonged time.[19] There are currently no universally accepted guidelines for CS clearance in the obtunded blunt trauma patient. The Eastern Association for the Surgery of Trauma leaves practice guidelines for this difficult problem to the discretion of each institution.[1] Computed tomography of the CS is the current gold standard for the initial evaluation of CS injury in blunt trauma patients; when this is normal, CS-MRI is often recommended as a follow-up examination for obtunded patients. There are several reports, however, suggesting that MRI is not necessary and may lead to harm in this patient population, resulting in complications related to unnecessarily prolonged immobilization and increased healthcare costs.
We performed a systematic review analyzing studies conducted from 2003 to present in an effort to develop an algorithm for CS clearance in the obtunded blunt trauma patient. All studies reviewed had level of evidence 2B with conflicting findings regarding the routine need for CS-MRI to evaluate for CS injury in the obtunded blunt trauma patient.
One of the few consistencies among the 11 studies evaluated is that in obtunded patients with gross motor function, clearing the cervical collar in the presence of a normal finding on multi-detector scanner appeared safe; none of such patients in these studies had any significant abnormalities on CS-MRI, and none subsequently developed any neurologic dysfunction. This is in alignment with a recent prospective study by Como et al,[20] demonstrating that removal of cervical precautions is safe and efficacious when CS-CT is normal in obtunded blunt trauma patients who exhibit gross movement of all extremities. On the other hand, none of the included studies reported a clear definition of an “unreliable physical examination;” whether the mere obtundation of a patient classified a patient's exam as unreliable was not consistently noted throughout the 11 articles reviewed. This limitation may be one source of the conflicting results between the studies. When the physical examination is of high quality and reliable, it may be reasonable to remove the cervical collar, but the data does not unanimously support this conclusion.
In all studies, CS-CT failed to reveal acute ligamentous injury, which was the reason for prolonged cervical collar immobilization in at least 74 (4.8%) patients after CS-MRI and surgical intervention in 11 (0.7%) patients. In the obtunded patient, the reported negative predictive value of flexion/extension films performed under fluoroscopy in ruling out ligamentous injury is over 99%; however, in the setting of normal CS-CT, the incidence of diagnosing any occult injury is very low.[21,22] Moreover, the flexion/extension views are not generally recommended in the obtunded patient due to chance for further neurologic compromise.[23]
CONCLUSIONS
Based on these results, we recommend the simple algorithm demonstrated in Figure 3. This allows the clearance of the cervical spine for patients with a normal CS-CT and intact gross motor function, but requires CS-MRI for other obtunded blunt trauma patients when an MRI scanner is available. In resource-limited settings where MRI is not available, patients without a reliable physical examination can be managed with prolonged cervical immobilization despite its drawbacks.
Figure 3.
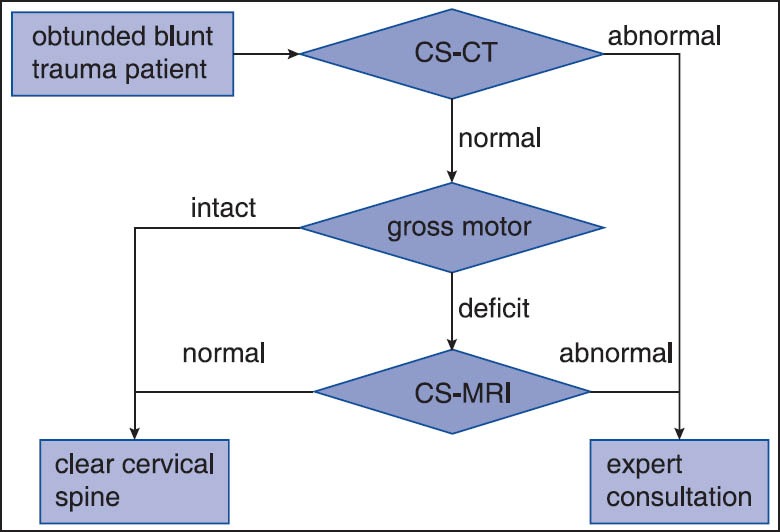
Simplified algorithm for the evaluation of cervical spine injury in the obtunded blunt trauma patient. CS-CT: Cervical spine computed tomography; CS-MRI: Cervical spine magnetic resonance imaging
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Como JJ, Diaz JJ, Dunham CM, Chiu WC, Duane TM, Capella JM, et al. Practice management guidelines for identification of cervical spine injuries following trauma: Update from the eastern association for the surgery of trauma practice management guidelines committee. J Trauma. 2009;67:651–9. doi: 10.1097/TA.0b013e3181ae583b. [DOI] [PubMed] [Google Scholar]
- 2.Diaz JJ, Aulino JM, Collier B, Roman C, May AK, Miller RS, et al. The early work-up for isolated ligamentous injury of the cervical spine: Does computed tomography scan have a role? J Trauma. 2005;59:897–904. doi: 10.1097/01.ta.0000188012.84356.dc. [DOI] [PubMed] [Google Scholar]
- 3.Menaker J, Philp A, Boswell S, Scalea TM. Computed tomography alone for cervical spine clearance in the unreliable patient-are we there yet? J Trauma. 2008;64:898–904. doi: 10.1097/TA.0b013e3181674675. [DOI] [PubMed] [Google Scholar]
- 4.Menaker J, Stein DM, Philp AS, Scalea TM. 40-slice multidetector CT: Is MRI still necessary for cervical spine clearance after blunt trauma? Am Surg. 2010;76:157–63. [PubMed] [Google Scholar]
- 5.Stassen NA, Williams VA, Gestring ML, Cheng JD, Bankey PE. Magnetic resonance imaging in combination with helical computed tomography provides a safe and efficient method of cervical spine clearance in the obtunded trauma patient. J Trauma. 2006;60:171–7. doi: 10.1097/01.ta.0000197647.44202.de. [DOI] [PubMed] [Google Scholar]
- 6.Sarani B, Waring S, Sonnad S, Schwab CW. Magnetic resonance imaging is a useful adjunct in the evaluation of the cervical spine of injured patients. J Trauma. 2007;63:637–40. doi: 10.1097/TA.0b013e31812eedb1. [DOI] [PubMed] [Google Scholar]
- 7.Panczykowski DM, Tomycz ND, Okonkwo DO. Comparative effectiveness of using computed tomography alone to exclude cervical spine injuries in obtunded or intubated patients: Meta-analysis of 14,327 patients with blunt trauma. J Neurosurg. 2011;115:541–9. doi: 10.3171/2011.4.JNS101672. [DOI] [PubMed] [Google Scholar]
- 8.Mushahid R, Elkhodair S, Zaheer A, Yousaf S. Safe cervical spine clearance in adult obtunded trauma patients on the basis of a normal multidetector CT scan-A meta-analysis and cohort study. Injury. 2013;44:1589–95. doi: 10.1016/j.injury.2013.06.005. [DOI] [PubMed] [Google Scholar]
- 9.Como JJ, Thompson MA, Anderson JS, Shah RR, Claridge JA, Yowler CJ, et al. Is magnetic resonance imaging essential in clearing the cervical spine in obtunded patients with blunt trauma? J Trauma. 2007;63:544–9. doi: 10.1097/TA.0b013e31812e51ae. [DOI] [PubMed] [Google Scholar]
- 10.Hogan GJ, Mirvis SE, Shanmuganathan K, Scalea TM. Exclusion of unstable cervical spine injury in obtunded patients with blunt trauma: Is mr imaging needed when multi-detector row ct findings are normal? Radiology. 2005;237:106–13. doi: 10.1148/radiol.2371040697. [DOI] [PubMed] [Google Scholar]
- 11.Soult MC, Weireter LJ, Britt RC, Collins JN, Novosel TJ, Reed SF, et al. MRI as an adjunct to cervical spine clearance: A utility analysis. Am Surg. 2012;78:741–4. [PubMed] [Google Scholar]
- 12.Steigelman M, Lopez P, Dent D, Myers J, Corneille M, Stewart R, et al. Screening cervical spine MRI after normal cervical spine CT scans in patients in whom cervical spine injury cannot be excluded by physical examination. Am J Surg. 2008;196:857–62. doi: 10.1016/j.amjsurg.2008.07.040. [DOI] [PubMed] [Google Scholar]
- 13.Schoenwaelder M, Maclaurin W, Varma D. Assessing potential spinal injury in the intubated multitrauma patient: Does MRI add value? Emerg Radiol. 2009;16:129–32. doi: 10.1007/s10140-008-0749-7. [DOI] [PubMed] [Google Scholar]
- 14.Tomycz ND, Chew BG, Chang YF, Darby JM, Gunn SR, Nicholas DH, et al. MRI is unnecessary to clear the cervical spine in obtunded/comatose trauma patients: The four-year experience of a level 1 trauma center. J Trauma. 2008;64:1258–63. doi: 10.1097/TA.0b013e318166d2bd. [DOI] [PubMed] [Google Scholar]
- 15.Khanna P, Chau C, Dublin A, Kim K, Wisner D. The value of cervical magnetic resonance imaging in the evaluation of the obtunded or comatose patient with cervical trauma, no other abnormal neurological findings, and a normal cervical computed tomography. J Trauma Acute Care Surg. 2012;72:699–702. doi: 10.1097/TA.0b013e31822b77f9. [DOI] [PubMed] [Google Scholar]
- 16.Stelfox HT, Velmahos GC, Gettings E, Bigatello LM, Schmidt U. Computed tomography for early and safe discontinuation of cervical spine immobilization in obtunded multiply injured patients. J Trauma. 2007;63:630–6. doi: 10.1097/TA.0b013e318076b537. [DOI] [PubMed] [Google Scholar]
- 17.OCEBM Levels of Evidence Working Group. “Oxford Centre for Evidence-based Medicine Levels of Evidence”. Oxford Centre for Evidence-Based Medicine. [Last accessed on 2013 Nov 3]. Available from: http://www.cebm.net/index.aspx?o=1025 .
- 18.Kaiser ML, Whealon MD, Barrios C, Kong AP, Lekawa ME, Dolich MO. The current role of magnetic resonance imaging for diagnosing cervical spine injury in blunt trauma patients with negative computed tomography scan. Am Surg. 2012;78:1156–60. doi: 10.1177/000313481207801032. [DOI] [PubMed] [Google Scholar]
- 19.Dunham CM, Brocker BP, Collier BD, Gemmel DJ. Risks associated with magnetic resonance imaging and cervical collar in comatose, blunt trauma patients with negative comprehensive cervical spine computed tomography and no apparent spinal deficit. Crit Care. 2008;12:R89. doi: 10.1186/cc6957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Como JJ, Leukhardt WH, Anderson JS, Wilczewski PA, Samia H, Claridge JA. Computed Tomography alone may clear the cervical spine in obtunded blunt trauma patients: A prospective evaluation of a revised protocol. J Trauma. 2011;70:345–51. doi: 10.1097/TA.0b013e3182095b3c. [DOI] [PubMed] [Google Scholar]
- 21.Davis JW, Parks SN, Detlets CL, Williams GG, Williams JL, Smith RW. Clearing the cervical spine in obtunded patients: The use of dynamic fluoroscopy. J Trauma. 1995;39:435–8. doi: 10.1097/00005373-199509000-00006. [DOI] [PubMed] [Google Scholar]
- 22.Hadley MN. Radiographic assessment of the cervical spine in symptomatic trauma patients. Neurosurgery. 2002;50(3 Suppl):S36–43. doi: 10.1097/00006123-200203001-00009. [DOI] [PubMed] [Google Scholar]
- 23.Anderson PA, Gugala Z, Lindsey RW, Schoenfeld AJ, Harris MB. Clearing the cervical spine in the blunt trauma patient. J Am Acad Orthop Surg. 2010;18:149–59. doi: 10.5435/00124635-201003000-00004. [DOI] [PubMed] [Google Scholar]