

Abstract
Background
This study was to evaluate the association of lumbar spine facet joint osteoarthritis (LSFJOA) identified by multi-detector computed tomography (MDCT) with age and low back pain (LBP) in an adult community-based population in Korea.
Methods
A sample of 472 participants (age range, 20 to 84 years) who underwent MDCT imaging for abdominal or urological lesions, not for chief complaints of LBP, were included in this study. LSFJOA based on MDCT findings was characterized using four grades of osteoarthritis of the facet joints. The prevalence of LSFJOA according to age group (below 40 years, 40-49 years, 50-59 years, 60-69 years, and above 70 years), gender, and spinal level was analyzed using chi-square tests and the association between LBP and LSFJOA adjusting for age, gender, and spine level was analyzed using multiple binary logistic regression test.
Results
Eighty-three study subjects (17.58%) had LSFJOA (grade ≥ 2). The prevalence of LSFJOA was not associated with gender (p = 0.092). The prevalence of LSFJOA increased with age (p = 0.015). The highest prevalence of LSFJOA was observed at L4-5 in men (p = 0.001) and at L5-S1 in women (p = 0.003), and at L5-S1 in the overall population (p = 0.000). LSFJOA was not associated with LBP in men (p = 0.093) but was associated with LBP in women (p = 0.003), especially at L3-4 (p = 0.018) and L5-S1 (p = 0.026).
Conclusions
The prevalence of LSFJOA based on the computed tomography imaging was 17.58% in the adult community Korean population. The prevalence of LSFJOA increased with age, and the highest prevalence was noted at L5-S1. LSFJOA was not associated with LBP at any spinal level and age except at L3-4 and L5-S1 in women.
Keywords: Lumbar spine, Facet joint arthritis, Low back pain, Community-based Korean population
The lumbar facet joint was first suggested as the source of low back pain (LBP) and lower extremity pain in 1911.1) Since then, facetogenic back pain has become widely accepted by many authors; however, the entity of facetogenic back pain is still controversial.2,3,4,5,6,7,8,9) Although the role of lumbar spine facet joint osteoarthritis (LSFJOA) has been supported by relief of LBP following intra-articular or periarticular injection,2,6) the relationship between LSFJOA and clinically significant LBP continues to be the subject of controversy.
The prevalence of lumbar spine facet joint originated pain based on single diagnostic blocks have been reported to range from 7.7% to 75% among patients reporting back pain.10,11) In the United States, the prevalence of lumbar facet joint pain is 15% on the basis of local anesthetic diagnostic blocks in a population of injured US workers.6) Similar studies report a prevalence of 40% to 45% in a pain management practice,8,9) and 40% in an Australian rheumatology practice.12)
Many published clinical studies report no correlation between the clinical LBP and degenerative spinal changes observed on many radiological modalities such as radiographs, magnetic resonance imaging, computed tomography (CT) and even radionuclide bone scanning.6,8,9,12,13) CT is the preferred method of imaging LSFJOA,11) providing cross-sectional images of the opposing joint surfaces in the axial plane4) at relatively low cost with precise osseous details.
The efficacy of intra-articular or periarticular injection therapy on LBP potentially associated with LSFJOA has not been clearly estabilished.11) Lewinnek and Warfield2) reported 96% correlation but Schwarzer et al.13) reported no associations. LSFJOA is a multifactorial process, and it has been suggested that the presence of intervertebral disc degeneration leads to a greater load and motion at the facet joint, resulting in degenerative changes similar to those seen in other synovial joints.14,15) LSFJOA is intimately tied to degeneration of the intervertebral discs.
Few studies on the prevalence of LSFJOA have been published. Eubanks et al.16) found that LSFJOA is a universal finding and characteristic osteoarthritis findings begin to appear early in more than one half of the adults younger than 30 years. The most common LSFJOA level appears to be L4-5. However, the prevalence of lumbar spine facet joint pain resulting from radiographically proven degenerative changes has not been known in adult community-based Korean populations and the association between the facet joint pain and radiologically observed facet joint degenerative changes has not been studied and remains controversial.11)
The aim of the present study was (1) to evaluate the prevalence of LSFJOA by age, gender, and spinal level, (2) to evaluate the association of LSFJOA with LBP, and (3) to evaluate which levels of LSFJOA are most associated with LBP in an adult community-based Korean population.
METHODS
Sample
This retrospective study included patients who had undergone CT between January 1, 2010, and December 31, 2010, and met the following criteria: they were over the age of 20 years, they gave us their informed consent and they underwent CT examinations to assess abdominal or urological lesions for reasons unrelated to LBP. The CT scans ordered by the Departments of General Surgery and Urology were included. To prevent a result bias, we excluded patients in whom a chief complaint of LBP was the primary indication for the CT examination ordered by the Departments of Orthopaedic Surgery, Neurologic Surgery, Rehabilitation and Pain Clinic. A total of 472 participants who were aged from 20 to 84 years were consecutively enrolled.
LBP Evaluation
All the participants who had undergone multidetector CT scanning were asked to complete two questionnaires, which were administrated by senior trained nurses who were not involved in this study. The question on LBP that was translated into Korean in the questionnaire was "Have you had LBP that needed medication almost every day for at least 1 month in the last 12 months?" This was modified from Nordic Low Back Pain Questionnaire.17) The individual's answers of "yes" or "no" to the above question was used in the present study as the LBP outcome. The question has been widely used by several authors18,19) for work-related compensation.
Scanning Parameters
CT was performed on one of three 16-multidetector computed tomography (MDCT) machines or a dual source 64-MDCT system (Lightspeed Ultra, GE Healthcare, Milwaukee, WI, USA). The axial slice thickness varied from 0.75 to 2.5 mm because the images were obtained from patients with different indications and by different protocols.
LSFJOA Evaluation
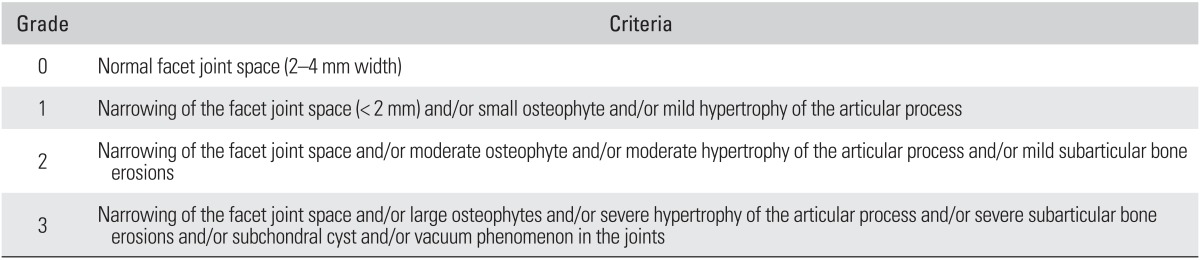
All the CT scans were analyzed in a blinded fashion by two orthopedic surgeons independently. The images were reviewed on a secure-access picture-archiving communication system (Philips Sectra, Linköping, Sweden). All the CT images that were initially reviewed were the axial images at the intervertebral disc level. Lumbar facet joints were graded on both sides at levels of L1-2, L2-3, L3-4, L4-5, and L5-S1. Four grades of facet joint osteoarthritis were defined using criteria similar to those suggested by Pathria et al.20) and Weishaupt et al.21) (Table 1). LSFJOA was defined as at least one joint affected by facet joint disease between the spinal levels L1 and S1 (grade ≥ 2).
Table 1.
Criteria for Grading Osteoarthritis of the Facet Joint
Statistical Analysis
Before the analysis, the study population was dichotomized on the basis of the presence of LSFJOA (≥ grade 2) on any side at any level. We analyzed LSFJOA in 5 different age groups (< 40, 40-49, 50-59, 60-69, and ≥ 70 years) and according to gender. The prevalence of LSFJOA in males and females each was compared according to the age group and according to the involved spinal level using chi-square (χ2) test for trend or multiple binary logistic regression analysis. Multiple binary logistic regression analysis was used to show the association between LBP and LSFJOA after adjusting for age, gender and spinal level. All the statistical analyses were performed with IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA). A p-value of less than 0.05 was considered to be statistically significant.
RESULTS
Epidemiologic Characteristics
The epidemiologic characteristics of the 472 participants are listed in Table 2.
Table 2.
Epidemiologic Descriptive Statistics of the Study Population (n = 472)
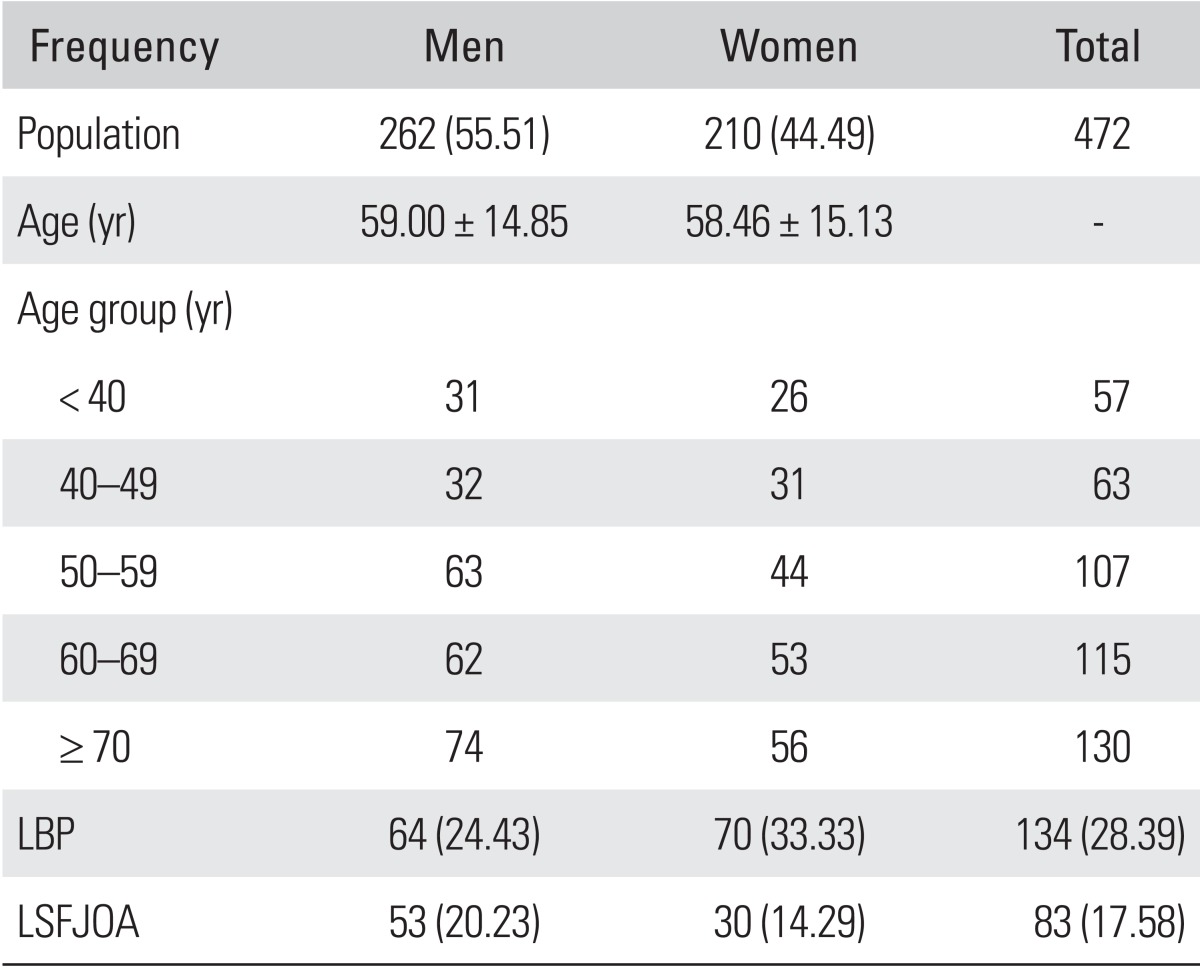
Values are presented as number (%) or mean ± standard deviation.
LBP: low back pain, LSFJOA: lumbar spine facet joint osteoarthritis (≥ grade 2) at one joint or more between spinal levels L1 and S1.
Prevalence of LSFJOA According to Gender and Age
The prevalence of LSFJOA according to gender and age is listed in Table 3. Fifty-three have LSFJOA but 209 have no LSFJOA in men (20.23%) and thirty have LSFJOA but 180 have no LSFJOA in women (14.29%). There is no statistically significant difference between men and women on the prevalence of LSFJOA (p = 0.092). The increasing age demonstrated a higher prevalence of facet joint osteoarthritis with statistical significance (p = 0.015).
Table 3.
Prevalence of LSFJOA According to Gender and Age
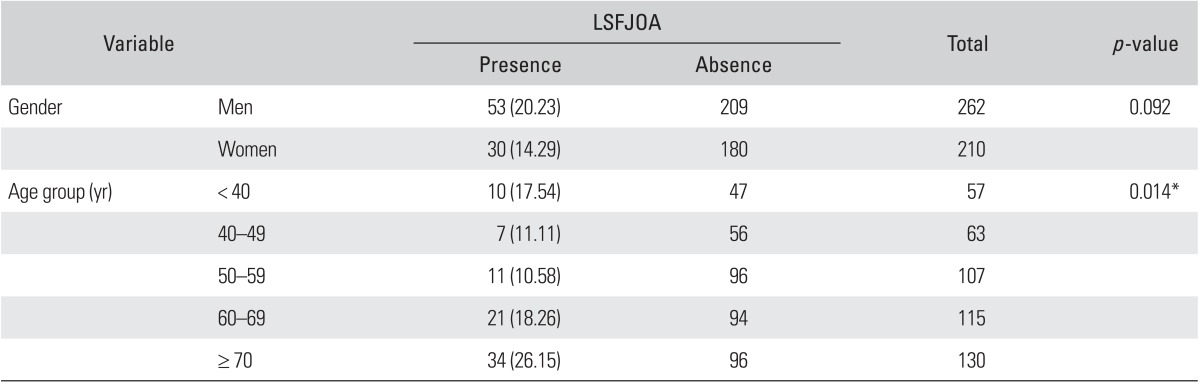
Values are presented as number (%).
LSFJOA: lumbar spine facet joint osteoarthritis (≥ grade 2) at one joint or more between spinal levels L1 and S1.
*p < 0.05.
Prevalence of LSFJOA According to Spinal Level
In men, the difference in the prevalence of LSFJOA according to the spinal level was statistically significant (p = 0.001) and the highest prevalence of LSFJOA was found at L4-5. In women, the different in the prevalence of LSFJOA across spinal levels was statistically significant (p = 0.003) and the highest prevalence of LSFJOA was found at L5-S1. In all population, the difference in the prevalence of LSFJOA according to the spinal level was statistically significant (p = 0.000) and the L5-S1 level exhibited highest prevalence. The gender difference at each level was not statistically significant (L1-2, p = 0.377; L2-3, p = 0.741; L3-4, p = 0.567; L5-S1, p = 0.893) except at L4-5 (p = 0.002). Men demonstrated a higher prevalence of LSFJOA compared to women at L4-5 level (Table 4).
Table 4.
Prevalence of LSFJOA According to Spinal Level
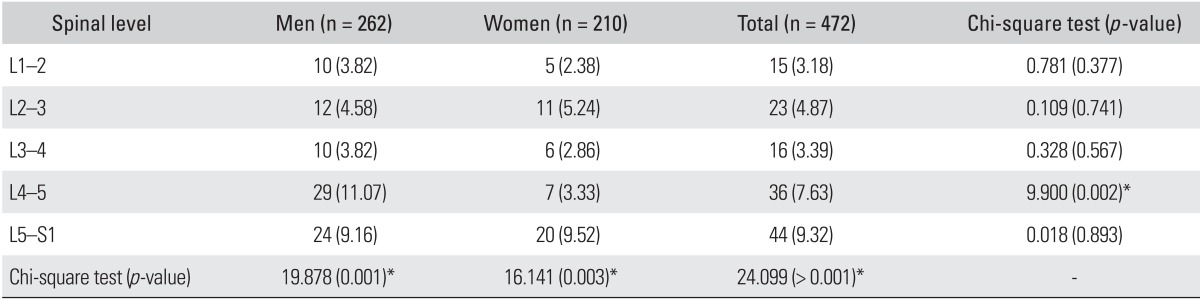
Values are presented as number (%) unless otherwise indicated.
LSFJOA: lumbar spine facet joint osteoarthritis (≥ grade 2) at one joint or more between spinal levels L1 and S1.
*p < 0.05.
LSFJOA and LBP
The prevalence of LSFJOA according to spinal level in individuals with or without LBP is listed in Table 5. The prevalence of LSFJOA was not associated with LBP in men (p = 0.093), whereas the prevalence of LSFJOA was associated with LBP in women (p = 0.003). The prevalence of LSFJOA according to age in individuals with or without LBP is shown in Table 6. The prevalence of LSFJOA was not statistically significantly associated with LBP (all, p > 0.05). LSFJOA at L3-4 and L5-S1 was related to LBP in women at a statistically significant level (p = 0.018 and p = 0.026, respectively). No significant difference in the prevalence of LSFJOA was identified between individuals with and without LBP in the study population as a whole or in the subgroup analysis based on age and gender except for the above-mentioned cases.
Table 5.
The Prevalence of LSFJOA According to Spinal Level in Individuals with or without LBP
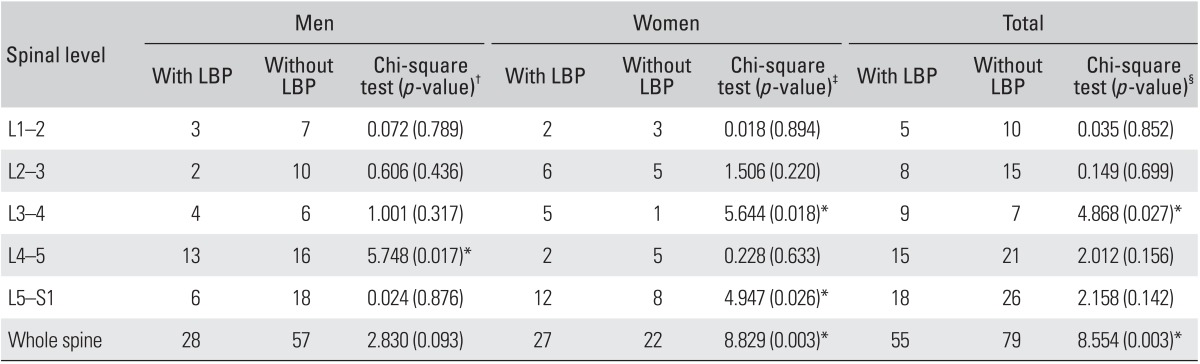
LSFJOA: lumbar spine facet joint osteoarthritis (≥ grade 2) at one joint or more between spinal levels L1 and S1, LBP: low back pain.
*p < 0.05. †Chi-square test (LBP vs. non-LBP by spinal level in men). ‡Chi-square test (LBP vs. non-LBP by spinal level in women). §Chi-square test (LBP vs. non-LBP by spinal level).
Table 6.
The Prevalence of LSFJOA According to Age in Individuals with or without LBP
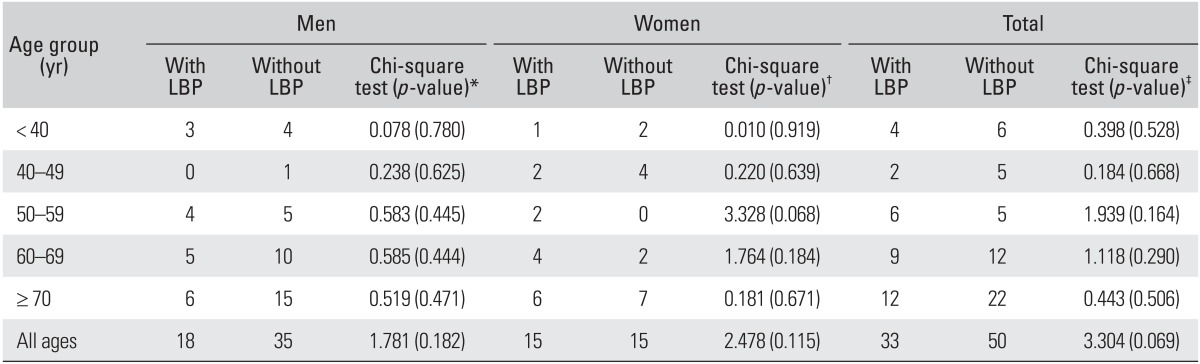
LSFJOA: lumbar spine facet joint osteoarthritis (≥ grade 2) at one joint or more between spinal levels L1 and S1, LBP: low back pain.
*Chi-square test (LBP vs. non-LBP according to age in men). †Chi-square test (LBP vs. non-LBP according to age in women). ‡Chi-square test (LBP vs. non-LBP according to age).
Multiple Logistic Regression Test
Regarding the multiple logistic regression analysis, LBP was a dependent variable and LSFJOA at each spinal level and gender were included as independent variables. LBP was not associated with spinal level and age group but was more common in women than men (p = 0.002) (Table 7).
Table 7.
Results of the Multiple Logistic Regression Analysis with LBP (Yes vs. No) Used as a Dependent Variable
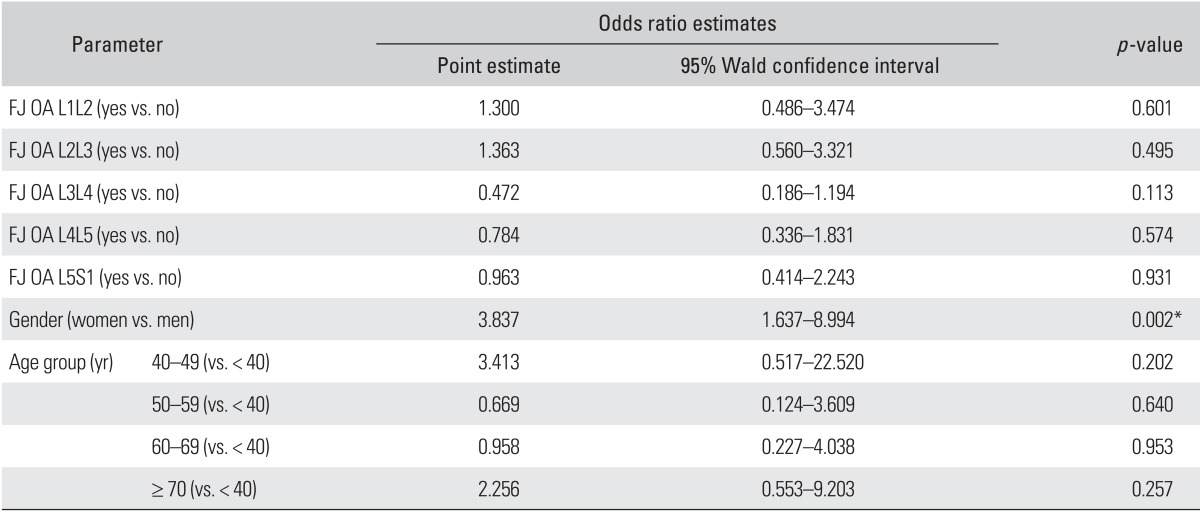
FJ OA: facet joint osteoarthritis (≥ grade 2).
*p < 0.05.
DISCUSSION
This is the first study to describe the prevalence of LSFJOA identified by MDCT in an adult community-based Korean population. The prevalence of LSFJOA in this study was lower than that in the study by Kalichman et al.11) This study also evaluated the association between LSFJOA and LBP in the adult community-based Korean population. Several authors have reported that LSFJOA is more common in the most caudal motion segments.22,23,24) Fujiwara et al.25) found that the median grade of LSFJOA at L4-5 was significantly higher than that at L3-4, while no significant differences were found between L3-4, L5-S1, and between L4-5 and L5-S1. Kalichman and Hunter23) stated that the possible reason for the high prevalence and severity of LSFJOA at the L4-5 spinal level may be its position as a transition between the more mobile lumbar segments and the relatively stiff L5-S1 segment. Unlike previous studies, the highest prevalence of LSFJOA was found at the L4-5 spinal level in men and at L5-S1 in women. Approximately 15%-40% of chronic LBP is attributed to LSFJOA.10) The histologic basis for facet joint pain has been scientifically established, but the precise clinical etiology remains undetermined.10) Hyperextension increases the load on the lumbar facet joint and stretches the capsule. This mechanical deformation may stimulate nociceptors in the joint capsule causing pain.26,27)
The observation that the age is associated with the incidence of LSFJOA is not surprising.11)
Lewin22) stated that facet joints showed only minor cartilage changes before the age of 45 years and that the osteoarthritis advanced with age. Kalichman and Hunter23) also reported that the prevalence of LSFJOA increases with age. However, some authors28,29) have reported the presence of LSFJOA in younger patients. The prevalence of LSFJOA in our study was more common in subjects less than 40 years of age than 40-49 years. The cause of this observation is unclear.
Gender has not been associated with the prevalence of LSFJOA in other studies.23,24) Fujiwara et al.25) found that motion segments in women showed significantly greater motion in lateral bending, flexion, and extension, but not in axial rotation, than in men in a cadaveric study. In our study, the prevalence of LSFJOA was not different between men and women.
In terms of specific spinal level, the present study did reveal statistically significant differences in the prevalence of LSFJOA between men and women at L4-5 spinal level where men demonstrated a significantly higher prevalence of LSFJOA than women. The result is same as the study by Eubanks et al.16) but is in contrast to the study of Kalichman et al.11)
The relationship of radiographic LSFJOA to the clinical syndrome of LBP is inconsistent.3) The cardinal role of facet joint abnormalities in patients with LBP is still debated.5,6,7) Schwarzer et al.13) even questioned the clinical importance of facet joint osteoarthritis. They were not able to demonstrate a significant correlation between the degree of osteoarthritis observed on CT and the pain score during the facet block. In our study, the prevalence of LSFJOA was not associated with LBP.
One of the limitations of this study is that it was a cross-sectional investigation without any longitudinal follow-up. In addition, we did not adjust for the bias such as occupation, which should be addressed in further analysis.
The prevalence of LSFJOA based on CT imaging was 17.58% (20.23% in men and 14.29% in women), was not associated with gender, increased with age, and was the highest at the L5-S1 spinal level in an adult community-based Korean population. At the L4-5 spinal level, LSFJOA was more common in men than in women. No significant association was observed between LSFJOA and LBP at any spinal level and age except at L3-4 and L5-S1 levels where LSFJOA was related to LBP in women.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Goldthwait JE. The lumbo-sacral articulation: an explanation of many cases of "lumbago", "sciatica" and paraplegia. Boston Med Surg J. 1911;164:365–372. [Google Scholar]
- 2.Lewinnek GE, Warfield CA. Facet joint degeneration as a cause of low back pain. Clin Orthop Relat Res. 1986;(213):216–222. [PubMed] [Google Scholar]
- 3.Helbig T, Lee CK. The lumbar facet syndrome. Spine (Phila Pa 1976) 1988;13(1):61–64. doi: 10.1097/00007632-198801000-00015. [DOI] [PubMed] [Google Scholar]
- 4.Carrera GF, Haughton VM, Syvertsen A, Williams AL. Computed tomography of the lumbar facet joints. Radiology. 1980;134(1):145–148. doi: 10.1148/radiology.134.1.7350594. [DOI] [PubMed] [Google Scholar]
- 5.Badgley CE. The articular facets in relation to low-back pain and sciatic radiation. J Bone Joint Surg Am. 1941;23(2):481–496. [Google Scholar]
- 6.Nachemson AL. Newest knowledge of low back pain: a critical look. Clin Orthop Relat Res. 1992;(279):8–20. [PubMed] [Google Scholar]
- 7.Schwarzer AC, Aprill CN, Derby R, Fortin J, Kine G, Bogduk N. Clinical features of patients with pain stemming from the lumbar zygapophysial joints. Is the lumbar facet syndrome a clinical entity? Spine (Phila Pa 1976) 1994;19(10):1132–1137. doi: 10.1097/00007632-199405001-00006. [DOI] [PubMed] [Google Scholar]
- 8.Manchikanti L, Pampati V, Fellows B, Bakhit CE. Prevalence of lumbar facet joint pain in chronic low back pain. Pain Physician. 1999;2(3):59–64. [PubMed] [Google Scholar]
- 9.Manchikanti L, Pampati V, Fellows B, Bakhit CE. The diagnostic validity and therapeutic value of lumbar facet joint nerve blocks with or without adjuvant agents. Curr Rev Pain. 2000;4(5):337–344. doi: 10.1007/s11916-000-0016-4. [DOI] [PubMed] [Google Scholar]
- 10.Dreyer SJ, Dreyfuss PH. Low back pain and the zygapophysial (facet) joints. Arch Phys Med Rehabil. 1996;77(3):290–300. doi: 10.1016/s0003-9993(96)90115-x. [DOI] [PubMed] [Google Scholar]
- 11.Kalichman L, Li L, Kim DH, et al. Facet joint osteoarthritis and low back pain in the community-based population. Spine (Phila Pa 1976) 2008;33(23):2560–2565. doi: 10.1097/BRS.0b013e318184ef95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schwarzer AC, Wang SC, Bogduk N, McNaught PJ, Laurent R. Prevalence and clinical features of lumbar zygapophysial joint pain: a study in an Australian population with chronic low back pain. Ann Rheum Dis. 1995;54(2):100–106. doi: 10.1136/ard.54.2.100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schwarzer AC, Wang SC, O'Driscoll D, Harrington T, Bogduk N, Laurent R. The ability of computed tomography to identify a painful zygapophysial joint in patients with chronic low back pain. Spine (Phila Pa 1976) 1995;20(8):907–912. doi: 10.1097/00007632-199504150-00005. [DOI] [PubMed] [Google Scholar]
- 14.Goode AP, Carey TS, Jordan JM. Low back pain and lumbar spine osteoarthritis: how are they related? Curr Rheumatol Rep. 2013;15(2):305. doi: 10.1007/s11926-012-0305-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Varlotta GP, Lefkowitz TR, Schweitzer M, et al. The lumbar facet joint: a review of current knowledge: part 1: anatomy, biomechanics, and grading. Skeletal Radiol. 2011;40(1):13–23. doi: 10.1007/s00256-010-0983-4. [DOI] [PubMed] [Google Scholar]
- 16.Eubanks JD, Lee MJ, Cassinelli E, Ahn NU. Prevalence of lumbar facet arthrosis and its relationship to age, sex, and race: an anatomic study of cadaveric specimens. Spine (Phila Pa 1976) 2007;32(19):2058–2062. doi: 10.1097/BRS.0b013e318145a3a9. [DOI] [PubMed] [Google Scholar]
- 17.Kuorinka I, Jonsson B, Kilbom A, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–237. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 18.Dovrat E, Katz-Leurer M. Cold exposure and low back pain in store workers in Israel. Am J Ind Med. 2007;50(8):626–631. doi: 10.1002/ajim.20488. [DOI] [PubMed] [Google Scholar]
- 19.Ghaffari M, Alipour A, Jensen I, Farshad AA, Vingard E. Low back pain among Iranian industrial workers. Occup Med (Lond) 2006;56(7):455–460. doi: 10.1093/occmed/kql062. [DOI] [PubMed] [Google Scholar]
- 20.Pathria M, Sartoris DJ, Resnick D. Osteoarthritis of the facet joints: accuracy of oblique radiographic assessment. Radiology. 1987;164(1):227–230. doi: 10.1148/radiology.164.1.3588910. [DOI] [PubMed] [Google Scholar]
- 21.Weishaupt D, Zanetti M, Boos N, Hodler J. MR imaging and CT in osteoarthritis of the lumbar facet joints. Skeletal Radiol. 1999;28(4):215–219. doi: 10.1007/s002560050503. [DOI] [PubMed] [Google Scholar]
- 22.Lewin T. Osteoarthritis in lumbar synovial joints: a morphologic study. Acta Orthop Scand Suppl. 1964:Suppl 73:1–Suppl 73:112. doi: 10.3109/ort.1964.35.suppl-73.01. [DOI] [PubMed] [Google Scholar]
- 23.Kalichman L, Hunter DJ. Lumbar facet joint osteoarthritis: a review. Semin Arthritis Rheum. 2007;37(2):69–80. doi: 10.1016/j.semarthrit.2007.01.007. [DOI] [PubMed] [Google Scholar]
- 24.Fujiwara A, Tamai K, Yamato M, et al. The relationship between facet joint osteoarthritis and disc degeneration of the lumbar spine: an MRI study. Eur Spine J. 1999;8(5):396–401. doi: 10.1007/s005860050193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fujiwara A, Lim TH, An HS, et al. The effect of disc degeneration and facet joint osteoarthritis on the segmental flexibility of the lumbar spine. Spine (Phila Pa 1976) 2000;25(23):3036–3044. doi: 10.1097/00007632-200012010-00011. [DOI] [PubMed] [Google Scholar]
- 26.Ashton IK, Ashton BA, Gibson SJ, Polak JM, Jaffray DC, Eisenstein SM. Morphological basis for back pain: the demonstration of nerve fibers and neuropeptides in the lumbar facet joint capsule but not in ligamentum flavum. J Orthop Res. 1992;10(1):72–78. doi: 10.1002/jor.1100100109. [DOI] [PubMed] [Google Scholar]
- 27.Yang KH, King AI. Mechanism of facet load transmission as a hypothesis for low-back pain. Spine (Phila Pa 1976) 1984;9(6):557–565. doi: 10.1097/00007632-198409000-00005. [DOI] [PubMed] [Google Scholar]
- 28.Tischer T, Aktas T, Milz S, Putz RV. Detailed pathological changes of human lumbar facet joints L1-L5 in elderly individuals. Eur Spine J. 2006;15(3):308–315. doi: 10.1007/s00586-005-0958-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gries NC, Berlemann U, Moore RJ, Vernon-Roberts B. Early histologic changes in lower lumbar discs and facet joints and their correlation. Eur Spine J. 2000;9(1):23–29. doi: 10.1007/s005860050004. [DOI] [PMC free article] [PubMed] [Google Scholar]