

Abstract
Background
We have constructed a simple, inexpensive simulation model for ultrasound guided nerve blocks. To date there are no low cost, high fidelity models for nerve block simulations. The models that do exist are expensive and vaguely resemble actual anatomy. As ultrasound guided nerve blocks become more common in medical education it is essential to develop better training models to help increase the comfort level of the individual provider and increase the chances for success during live-patient procedures [Anaesth Intensive Care 37: 824-829, 2009].
Methods
The nerve block model was produced with a single pork loin with pressure-injected ultrasound gel through both CAT 5 cable and IV tubing inserted length-wise into the pork loin.
Results
Our nerve block model had a realistic, life-like feel simulating human tissue.
Conclusion
This ultrasound nerve block model was inexpensive with life-like feel allowing resident trainees to develop more confidence and tactile skill to increase the chance for success.
Keywords: Regional anesthesia, Ultrasound, Phantom model, Nerve block
Background
For decades regional anesthesia has traditionally been taught using anatomic guidance where the patient was the model for trainees [1],[2]. In the modern era of medicine this is no longer an acceptable practice [1],[3]. Previous studies have shown that after simulation training, the novice can be more comfortable and more successful in executing the neuraxial blocks. First reported by La Grange and colleagues in 1978 as a way to decrease the complication rate of supraclavicular brachial plexus blocks [4]. Since then innumerable studies have shown better avoidance of side effects, reduction in medication load, faster onset of anesthesia, longer duration of blocks, and improved quality of blocks [5]. Despite the known advantages of simulated nerve blocks, the models have primarily been expensive low fidelity gelatin-type models.
Given the importance of simulation of training and the known improved outcomes, we developed an easy to create ultrasound model that can facilitate regional nerve blocks, as well as intravenous access [2]. The procedure for creating the phantom model are in the Appendix.
Methods
Using a similar method for epidural nerve block, we used a block of pork loin, CAT 5 ethernet cable, IV tubing, and ultrasound gel to create the phantom. Using a method for preservation previously described [3], we used hand sanitizer to preserve the pork loin overnight. Once preserved, we used long Kelly clamps to length-wise puncture the pork loin a single time through the center to grasp the ethernet cable and the intravenous tubing. Afterward, both the IV tubing and ethernet cable were pressure injected with ultrasound gel until it was expressed from the free end. We then clamped the ends of the IV tubing and ethernet cable with straight Kelly clamps to contain the gel Figures 1 and 2.
Figure 1.
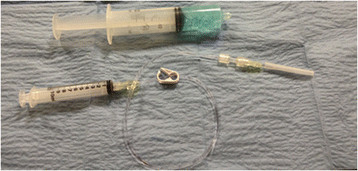
Supplies needed.
Figure 2.
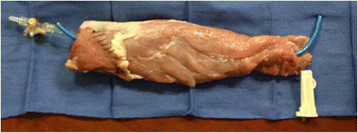
Completed nerve block model.
Results and discussion
This produced a high fidelity model that was used multiple times for regional neuraxial blocks. The tissue was kept viable for a couple of weeks, as long as cooled afterward and kept wrapped to maintain the preservation effect. The total cost was nearly $25 USD. The low cost and reproducibility of the model make it an easy and cost-effective method of simulation.
Although the model produced a great simulation model and prolonged use, it is limited by a definite shelf life when compared to commercial phantom models. However, this pork-loin model did give a more realistic tactile feel when compared to gelatine-type phantoms as well more realistic visual imaging during dynamic neuraxial block practice. We hope the use of high fidelity simulators for ultrasound guided regional anesthesia will lead to greater provider confidence and ultimately increased patient safety Figures 3 and 4.
Figure 3.

Ultrasonographic image of the nerve and artery.
Figure 4.

Ultrasound guided nerve block.
Conclusions
This nerve block model produced a life-like simulation for nerve block and vascular access. Using tools and equipment readily available, the pork loin was used repeatedly by resident trainees. The tissue felt life-like during the initial skin puncture and through the fascial planes. The CAT5 “nerve” was a good simulation for injecting local anesthetic and produced the “donut sign” of hypo echoic fluid around the nerve. Because the “nerve” was metallic wiring, it produced some posterior shadowing that limited the ability to visualize the posterior site of needle insertion or fluid spread; however, injecting the local anesthetic was visualized along the plane of the “nerve” similar to human tissue. Vascular access was practiced with hollow-bore metal needles to allow the feel of fluid aspiration and visualization and repositioning of the needle during dynamic ultrasound. Plastic vascular catheter placement was limited by the thickness of the IV tubing used.
Despite these limitations to posterior visualization and plastic catheter placement, this model will allow safe, more life-like, pain-free practice of neuraxial block and vascular access before attempting on patients to improve the chances for success.
Appendix
Pork-Loin Neuraxial Model
Ingredients:
Store-bought Pork Loin
1 CAT 5 ethernet cable cut longer than Pork Loin
1 Peripheral IV tubing cut longer than Pork Loin
10 cc syringe and Starter IV connector to pressure inject
Ultrasound gel
1 Straight Kelly Clamp
1 Long Kelly Clamp
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
All authors contributed to model design, execution, and manuscript preparation. All authors read and approved the final manuscript.
Contributor Information
Scott Sparks, Email: sparkyur@gmail.com.
David Evans, Email: evansdp@me.com.
Don Byars, Email: don.byars@gmail.com.
Acknowledgement
We thank Karianne Sparks and Lindsey Solovey, RDMS for manuscript preparation.
References
- White SM. The ethics of anaesthesia learning curves. Anaesth Intensive Care. 2009;37:824–829. doi: 10.1177/0310057X0903700503. [DOI] [PubMed] [Google Scholar]
- Marhofer P, Greher M, Kapral S. Ultrasound guidance in regional anaesthesia. Br J Anaesth. 2005;94:7–17. doi: 10.1093/bja/aei002. [DOI] [PubMed] [Google Scholar]
- Hocking G, Gilmour F, Mitchell C (2010) Porcine phantom for ultrasound-guided neuraxial blockade. British J of Anaesthesia, Online 28 January 2010.
- La Grange P, Foster PA, Pretorius LK. Application of the Doppler ultrasound bloodflow detector in supraclavicular brachial plexus block. British J Anaesth. 1978;50:965–967. doi: 10.1093/bja/50.9.965. [DOI] [PubMed] [Google Scholar]
- Xu D, Abbas S, Chan VW. Ultrasound phantom for hands-on practice. Reg Anesth Pain Med. 2005;30:593–594. doi: 10.1097/00115550-200511000-00026. [DOI] [PubMed] [Google Scholar]