

Abstract
The aim of this article was to analyze the theories underpinning dental fear, anxiety and phobias. To be included, articles must have been published between the years of 1949 and 2013 concerning fears and phobias within dentistry and/or psychiatry. Of 200 articles originally under review, 140 were included and reviewed by the authors.Five specific pathways relating to dental fear and anxiety were identified; Cognitive Conditioning, Informative, Visual Vicarious, Verbal Threat, and Parental. Eight currently accepted management techniques across all dental disciplines for dental fear and anxiety were identified. Further research is required to identify clinical diagnosis and treatment for fears originating from different pathways.
Keywords: Dentistry, Fear and anxiety, Phobia, Origin, Therapies and management
Core tip: (1) 5 pathways to the origin of dental fear and anxiety have been identified in this review: Cognitive Conditioning, Informative, Visual Vicarious, Verbal Threat, and Parental; (2) Development of fear and anxiety may be unique for each individual, with patients often associating fear to a combination of factors (Pathways); and (3) Management of fear and anxiety should include an understanding of the origins of dental fear.
INTRODUCTION
Odontophobia (dental fear) is a “unique phobia with special psychosomatic components that impact on the dental health of the odontophobic persons”[1]. For some individuals, dental fear may be so great that normal life is impaired. In these instances, the individual experiences fear or anxiety that is out of proportion to the actual danger present in the situation. This often leads to avoidance behavior, and clinically significant levels of distress or impaired functioning[2]. Such avoidance behavior is well known by any dentist who has treated patients with high levels of dental fear before. In Australia, people with higher levels of dental fear tend to avoid the dentist and have irregular attendance records, usually only seeking treatment when symptomatic[3,4]. This data is consistent with other studies that noted that, although patients booked appointments, they did not keep their appointment or prematurely cancelled their appointments out of fear[5-12].
The incidence of dental fear and anxiety appears to be relatively consistent throughout the world, with some sub-groups reporting higher levels than others. An Australian study reported that 16.1% of individuals experienced high levels of dental fear, where adults between the ages of 40 and 64 years reported a higher incidence of dental fear, and females of any age were reportedly more afraid of the dentist than males were[4]. Of note, people from low socioeconomic status (SES) groups reported a generally higher level of dental fear than those individuals from high SES groups[4]. The reported incidence of high dental fear and anxiety was a little lower in an Icelandic study, at only 10%[11], but slightly higher in a Singaporean population, at 17.1%[12]. A cross-cultural study of Chinese and Danish patients reported moderate to high dental fear in 30% of Chinese and 15% of Danish participants[10]. In 2009, a study of dental fear prevalence in 1959 Netherlands reported 24.3% of the participants had moderate to high dental fear[13]. Dental fear studies on German populations have reported a mean Dental Anxiety Score (DAS) of 8.6[14] and a dental phobia incidence of 11%[15]. The highest prevalence of dental fear appears to be in Japan, where a study of 3041 students and adults reported that 42.1% had high dental fear[16].
The overall effect of dental fear and anxiety appears to be multifaceted, such that the individual not only avoids their dental appointments but also tends to have worse oral health[17]. The extent to which this is a causal relationship is unknown. An understanding of the factors underlying the etiology and maintenance of dental anxiety may assist dentists and researchers in developing interventions designed to reduce dental avoidance behaviors. In turn, this will contribute to improvements in oral health. Mehrstedt et al[18] (2004) noted that dental fears were negatively linked to quality of life with respect to psychological well-being, social functioning, and vitality. This finding indicates that the link between dental fear and perceived negative quality of life is multifaceted. Some early Scandinavian studies reported on the malicious circle of dental anxiety and fear, whereby fear and avoidance lead to premature cancellation of dental appointments and further worsening of oral health conditions[2,6,19,20]. A qualitative study by Moore et al[21] (2004) reported on the contributing role that embarrassment plays in dental phobia. Among other things, these researchers analyzed the social powerlessness associated with the embarrassment that arises from poor oral health. In this study, the authors concluded that patients may be so embarrassed by their poor oral health/hygiene that they avoid seeing the dentist out of fear of being reproached[1,21]. Understanding the extremely complex psychology of dental fear is essential in the prevention and treatment of dental anxiety, fear and phobias[21].
In order to understanding the extremely complex psychology of dental fear it is essential to understanding possible pathways of dental fear and anxiety. This study identified relevant studies using Medline Database (Medline/PubMed). The search covered the period 1900 to 2014, including only articles written in English. Search terms included “dental fear and anxiety,” “cognitive,” “informative,” “verbal threat,” “vicarious,” “parental,” and “origin of fear.” A total of 300 references were retrieved from the database search. Only articles directly relating to the management, origin of fear, and dental fear theories were evaluated to understand the pathways of fear and anxiety in dentistry. Of the three hundred retrieved references, only 137 related to fear and anxiety in dentistry, however only 10 related specifically to origins of fear and anxiety in dentistry. The aim of this review is to highlight the possible pathways of fear and anxiety in dentistry and not to analysis the actual experience of fear and anxiety.
ETIOLOGY OF GENERAL FEAR AND ANXIETY
Processes known to contribute to the etiology of dental fear and phobia include a variety of genetic, behavioral, and cognitive factors. An individual’s dental fear/phobia is likely to have been created by involving a multitude of factors.
Genetic vulnerability
Individuals with specific phobias, including odontophobia, may have inherited genetic vulnerability factors that predispose them to anxiety in general or certain phobias specifically. While individuals with dental phobia do not directly inherit the phobia itself, genetic vulnerability factors may interact with other etiological elements that cause the phobia[22,23]. Controversy over the reliability of phylogenetic origin of fear arises in relation to a study of 173 Swedish twins, which reported that whilst “phenotypic correlations were moderate,” they were found to be counterintuitive to the electrophysical skin conductance response (SCR)[23]. In summary, it has been suggested that although genetics can predict some factors related to dental fear, it appears to be distally and not strongly related to the actual development of phobic symptom[24-26].
Negative affectivity/anxiety vulnerability
Negative affectivity refers to a vulnerability to experiencing negative emotional states. Negative affectivity appears to be a stable personality trait that predisposes individuals to a range of psychological disorders, including phobias[27]. The relationship between negative affectivity and dental phobia has not yet been established.
Preparedness
Through the process of natural selection, individuals who readily acquired fear and avoidance responses to genuinely dangerous situations (e.g., dangerous animals, storms, heights, small spaces, etc.) have passed on this tendency to their progeny[28]. As such, the human species is “prepared” to more readily acquire fear reactions to stimuli that may have posed a genuine danger to our ancestors[28,29]. Dental phobia may be part of an evolutionarily beneficial tendency to protect the body envelope from intrusion by foreign (non-nutritional) objects.
Cognitive conditioning (pavlovian)
Classical (or pavlovian) conditioning refers to the process by which a previously neutral stimulus acquires the ability to directly elicit a response through pairing this stimulus with another unconditioned stimulus (US) that elicits the same response[30-33]. For example, an individual who experiences a painful procedure (and the unconditioned response of anxiety/fear) during a dental visit may acquire a conditioned association between the dentist (the conditioned stimulus) and anxiety/fear (the conditioned response)[34-37]. Re-presentation of the conditioned stimulus (the dentist or related stimuli) is then able to elicit the conditioned response of anxiety during the patient’s next dental consultation.
Operant conditioning
Operant conditioning refers to a process whereby the frequency of a particular behavior (“operant”) is modified through the consequences that follow the behavior. Certain behaviors may be “reinforced” (i.e., increased in frequency) through their association with positive consequences (“positive reinforcement”) or through the removal of negative consequences (“negative reinforcement”)[30,34,35,38,39]. Alternatively, behaviors may be “punished” (i.e., reduced in frequency) if they lead to negative consequences (“positive punishment”) or the removal of positive consequences (“negative punishment”)[38]. For phobias, the process of positive punishment (e.g., pain and anxiety that occurs during a visit to the dentist) and negative reinforcement (e.g., the reduction in anxiety that results when the individual avoids the dentist) are thought to be most important, and these comprise Mowrer’s two-factor model of phobia acquisition and maintenance[40].
Vicarious
In addition to direct contributors to phobia acquisition, Rachman[41] (1978) proposes that individuals may also acquire phobic responses indirectly. One such pathway has been called vicarious experience or vicarious conditioning. In vicarious conditioning, the individual acquires a fear response through seeing the fearful experience of others. In dental phobia, for example, a child who observes a fear response of a parent attending the dentist may learn indirectly that the situation poses a significant threat.
Verbal threat
Rachman[36] (1977) proposed a second indirect pathway to phobia acquisition referred to as “verbal transmission”. In this process, the individual acquires a fear or phobia through learning about the dangerousness of a situation from others without observing it directly[36]. In dental phobia, for example, an individual may hear stories from others about traumatic or painful experiences that they have had during dental treatment, which may lead to a learned fear of dental procedures[42].
Cognitive content
There are a range of cognitions that have been identified as important in the acquisition and maintenance of anxiety disorders, including specific phobias. These include a set of ideas about the probability (e.g., “If I go to the dentist it will definitely be painful”) and severity (e.g., “If I go to the dentist the pain will be excruciating”) of negative outcomes[43]. Additionally, individuals may hold beliefs about their inability to cope in the face of an aversive outcome (e.g., “If I am in pain at the dentist, it will be unbearable”)[44].
Cognitive biases
In addition to the content of cognition, phobias are associated with biases in the process of cognition[43]. For example, individuals with anxiety disorders such as phobias are known to have memory biases in which memories of threat-consistent experiences and information are more readily retrieved[45]. Although the link between cognitive bias and dental fear and anxiety is plausible, no research has yet been done to confirm this.
CURRENT KNOWLEDGE OF DENTAL FEAR: WHAT WE KNOW RIGHT NOW
Current literature on dental fear is limited relative to other fields. Specifically, most of our understanding surrounding dental fear is based on results from two meta-analyses; one of which focuses on adults, while the other on children and adolescents.
In a meta-analysis of 32 articles on dental behavior management problems, Klingberg et al[46] (2007) reported that children and adolescents were expected to experience mild fear and anxiety. This fear and anxiety only becomes a concern if it is “disproportionate to the actual threat and daily functioning becomes impaired”, a definition very similar to the DSM-IV. However, this research also noted that the third criterion for dental phobia (recognition that the fear is unreasonable or excessive) does not always apply to children. This is a reasonable argument, as coping with pain and anxiety requires a high level of cognitive function and self-control that a young child might not have yet developed. However, one must attempt to separate general fearfulness (an anxiety-related personality trait) from a specific fear because both are capable of presenting as an acute fear reaction (e.g., screaming at the sight of a drill). This distinction can be difficult to make if the parent-child relationship is synergistically inflating the dental fear. Research demonstrates that the dental fear of a child who is 8 years or younger is significantly related to the dental fear of the parent[47]. However, in children older than 8, the relationship is less clear. In addition, it was noted that girls presented as more anxious and harder to manage than boys, supporting the current accepted relationship between anxiety disorders and gender in children and adolescents[48]. However, particular fears changed as the child grew older, such that one-year-old had separation anxiety but primary school children had more social anxieties, demonstrating a positive development of metacognition. Also, younger children were more likely to have more fears of higher intensity. However, there is inconclusive evidence regarding the origin of fear among children and adolescents due to the gap in the literature examining this cohort. In their review, Klingberg et al (2007) did, however, agree on 3 distinct, yet commonly occurring causes for dental fear in children (not including neuropsychiatric disorders): (1) Some children’s past “negative experiences with dental care” was the origin of their dental behavior management problems; (2) Other children were “genetically prone to react with fear…to threatening situations”; and (3) Other children still reacted to frustrating demands (e.g., sitting still) with anger[46].
The first represents direct trauma from treatment[36], while the second and third are officially undefined at present and require further investigation. It must be noted that parental dental fear has an effect on the child’s dental fear[47,49]. Making it an important part of the conceptualization of an individual’s dental phobia.
With regard to adults, it is generally accepted that the patient developed fear either due to personal trauma from a dental treatment or because of some form of psychological disorder or constitutional vulnerability. Yet, few studies analyze the actual pathway or origin of fear adults experience with regard to dental fear. However, it is possible that some of these origins may apply directly to dental fear[50] (Figure 1). Originally Watson et al[33] (1920) and Rachman[41] (1978) purported that specific fears were condition-based, vicarious, or based on information learning. Between the 1920s and 1970s, these theories dominated the discipline of fear and anxiety management and diagnosis. In 1970, Seligman proposed that mankind is prepared by evolution to associate certain situations (previously encountered by ancestors) with particular outcomes, and thus the mind reacts to these situations by instigating fear (See Figure 1: Preparedness framework)[51]. In 2001, Mineka et al[28,52] suggested that the amygdala and hippocampus were responsible creating generalized fear responses. Analogous to this and supporting Seligman’s theory, Poulton et al[53,54] (2002) posited that evolutionarily associated fears can manifest without a stimulus. Among these theories, the associative and non-associative theories are the most distinctive. Menzies et al[55,56] (1993a) first described the associative theory in relation to water phobia, where fears occur in response to a bad experience (CS), while non-associative fears are innate (US). In addition, Muris et al[57] posited that parental modeling contributes to the fearfulness found in children. Here, the trait anxiety was related to that of both parents (Mother: r = 0.34, P < 0.05, Father: r = 0.31, P < 0.05), but the act of being fearful was only related to mother’s fearfulness (r = 0.56, P < 0.001)[57]. Klingberg et al[58] also supported the notion of maternal dental fear impacting the development of dental fear in children.
Figure 1.
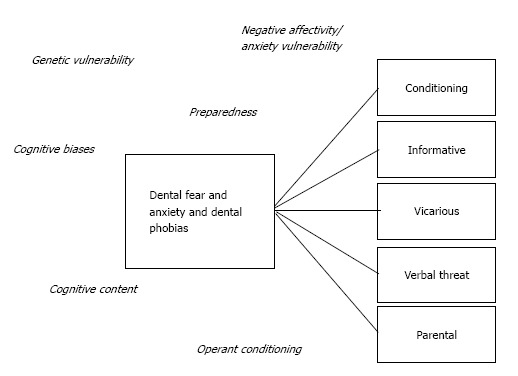
Pathways of fear in dentistry with background influences.
Of these theories, there are 5 pathways that are thought to specifically relate to dental fear and anxiety: Cognitive Conditioning, Vicarious, Verbal Threat, Informative, and Parental (Figure 1). These five pathways are discussed further in this article but it is important to note that a single or a combination of background factors disused in the etiology of general fear and anxiety may affect these pathways.
Conditioning pathway
Conditioning is a process where the participant learns through personal experience that the event or stimulus heralds a detrimental outcome[50,59]. Pioneers in early conditioning research Watson et al[60] (1917) who theorized that in infancy there are limited emotional reaction patterns (e.g., fear, rage, love) and that there must be some stimuli which are associated with these. Watson et al[33] (1920) then performed experimental work on an infant, analyzing directly conditioned emotional responses. Their results showed that the non-fear-inducing stimuli elicited a fearful emotional response when the fear-inducing and non-fear-inducing stimuli were shown together, and when the non-fear-inducing stimuli was shown on its own later[33]. In 1927, Pavlov[32] published his seminal paper on “Conditioned Reflexes,” which perhaps represents the first in-depth and detailed experiment on the development of conditioning. Pavlov[32] identified that animals can learn to associate a conditioned stimuli with a new non-conditioned stimuli so that the non-conditioned stimuli causes a conditioned response. Here, the animals (dogs) began to associate food and salivating with the sound of a bell. Thus, anytime the bell sounded, the dogs salivated[32]. In a similar attempt to replicate physiological responses during fear, Rachman[41] (1978) then successfully demonstrated that physiological responses, such as sweating and increased heart rate, occur when individuals experience fear. Such responses are evident in odontophobic patients, where heart rate, breathing, and sweating all increase due to fear associated with dental environments and dental stimuli[19,61-63]. In addition, many individuals report painful past experiences being the cause for their subsequent dental fear[44,64-66]. Researchers[67] have indeed found a “strong direct relationship between severity of trauma-related symptomatology and severity of dental anxiety where the shared variance was 38%”[67]. Thus, it can be proposed that the majority of dental fears are reactions to stressful experiences that provoke anxiety in the individual[36,68-70]. In summary, the conditioning pathway appears to be the most commonly utilized pathway by patients.
Informative pathway
The informative pathway is another indirect pathway for fear acquisition, which does not require the presence of an unconditioned stimulus. As far back as 1977, Rachman discussed the relevance of the informative pathway in so much as child-rearing involved information giving[36]. Rachman[36] noted that the instructional process of child rearing may lead to biases for commonly encountered fears. Such a dynamic could help explain childhood dental anxiety, where children learn to fear the dental environment from dental phobic elders, negative connotations advertised by media (e.g., television, movies), and friends with personal negative experiences.
Vicarious pathway
The vicarious pathway is an indirect pathway for fear acquisition that does not require the presence of an unconditioned stimulus. It has been acknowledged in the literature that people with extreme dental fear avoid the dentist[3,4,17,33,71-78]. In a recent Australian study using Armfield’s Index of Dental Anxiety and Fear (IDAF), it was found that participants who indicated extreme dental fear were marginally more likely not to undertake an oral examination, here females exhibited significantly higher dental fear than males[4,71]. Whether this fear is purely conditioned or vicarious is not yet fully understood[76]. Conceivably, one of the most renowned contributions to the theory of “vicarious conditioning in phobia acquisition”[50] was by a pair of researchers[38,52,79] whose experiments provided convincing evidence that fear can be learned vicariously[36,69,80]. By utilizing this vicarious pathway, it is plausible to suggest that vicarious learning could be contributing to pediatric fears, whereby expressions of fear by elders at the dentist in front of children leads to fear acquisition in the children[81,82].
Verbal threat pathway
The verbal threat pathway presents another indirect pathway for fear acquisition that does not require the presence of an unconditioned stimulus. To explain the origin of a fear that is not seen or experienced, it is essential to understand the “emotion” of fear. Research[83] has suggested that emotions arise because of three factors: verbal cognition, behavior changes, and physiological states. This “emotion” is known as the “tripartite,” and appears to govern onset and origin of fears generated by the verbal threat pathway[83-87]. Many articles examining the effects that “word of mouth” information has upon children and acquisition of fear[81,82,84-86,88-97] note that children become fearful of a stimulus or situation when they hear or read that it may be dangerous. To control for bias, all studies were done on medically healthy children, aged 6-13 years. The majority of participants (88.9%) demonstrated that self-reported fears increase as children were given violent/dangerous/threatening information about a particular stimulus, irrespective of its actual threat[85,86,92-94]. Simultaneously, it has been found that giving positive information results in a decrease in children’s self-reported fear[89,91]. Similar research on children ages 7-9 years found that when given verbal information about a “monster, “children’s fear-beliefs changed. However, these fear-beliefs only changed when information came from an adult[96]. In short, one interpretation of the verbal threat pathway is that fear is induced when an authority figure threatens an individual with a painful experience. In the case of dental fear, painful and/or negative experiences are linked to dental visits. Although perhaps within strict psychological terminology the informative and verbal threat pathways are similar. Within odontophobia the two pathways differ in that the verbal threat pathway occurs when a “visit to the dentist” is literally used as a form of punishment for bad behavior. This does not occur in the informative pathway.
Parental pathway
The parental modeling pathway presents another indirect pathway for fear acquisition that does not require an US. The concept of parental modeling is supported by research[69] demonstrating that in a sample of 40 children between the ages of 9 and 12 years, children’s fear was positively related to their mother’s dental fear. Specifically, mothers who expressed heightened levels of fear in front of their children were more likely to have fearful children. Conversely, mothers who did not frequently express fear had less fearful children[69]. These findings are consistent with another study showing that most adults attributed the origin of their fears to informative and vicarious factors occurring in childhood (56% and 39%, respectively) more so than to cognitive model events (37%)[84]. Given that the majority of heightened levels of fear in some children was a consequence of an amalgamation of different learning dynamics[69], it has been suggested that “fear is more likely to develop as a result of synergistic effects of various sources or origins”[56]. However, one must note that any relationship between parent and child fears may also be due to the informative or vicarious pathways because they are all linked in some way. Again, strict psychological terminology may not necessarily differentiate between the parental and vicarious pathways. However within odontophobia individuals utilizing the parental pathway had their sole influence of odontophobia from their parents’ expression of fear, whereas the vicarious pathway is multifaceted. Further investigation is needed to identify criteria for each pathway’s application.
MEASUREMENT INSTRUMENTS AND DIAGNOSTIC CATEGORIES OF DENTAL FEAR AND ANXIETY
Measures of dental anxiety (Pre-1990)
The first widely accepted questionnaire for assessing dental fear was the Phobic Origins Questionnaire (POQ). Out of the 10 items, the first 9 required the participant to make a binary Yes/No response[98,99]. Following the POQ, a 16-item self-report questionnaire referred to as the Origins Questionnaire (OQ)[56,100] became popular. This measure also examined individuals’ history in relation to their phobia[55,56]. However, as several studies have indicated[56,101-103], the POQ is inherently biased towards conditioning models. It was found that the POQ indicated conditioning was the primary origin for fear 56%-78% of the time, while the vicarious pathway accounted for 17%-42%[104]. Additionally, given that the control group for this research[99] consisted of only analogue cases of mild and low level fear by different researchers[77,105-107], it cannot be confirmed that this research represents the general populations’ origins of fear. Numerous other researchers have criticized the POQ, noting that the authors wrongly systematized frightening stimuli to relate to the cognitive model origin, even though no unconditioned stimulus was described by participants[55,56,108,109]. Consequently, the construct validity and convergent validity of the POQ was found to be very poor[55,56,100,101,103,110,111].
Measures of dental anxiety (Post 1990)
As dental fear can be difficult to define and measure effectively[103,109], research began to create a more practical, reliable, and theoretically efficacious dental fear measurement. Research found that the Index of Dental Anxiety and Fear (IDAF-4C+), developed by Jason Armfield presented strong statistically significant correlations with previous measures of dental fear (Corah’s DAS, 1969). Armfield’s reasoning for creating a new dental fear scale was due to problems with existing scales such as Kleinknecht’s Dental Fear Survey (DFS, 1973), Stouthard’s Dental Anxiety Inventory Short-Form (DAI-S, 1993), the Modified Dental Anxiety Scale (MDAS, 1995), and the Hierarchical Anxiety Questionnaire (HAQ, 1999). Problems associated with these measures were that they were too long, measured fear-related stimuli rather than fear itself, and had poor construct validity[71,77,112,113].
Consisting of 3 modules, each with 8 items, the IDAF-4C+ analyzes emotional, behavioral, physiological, and cognitive responses related to dental fear[66,113]. Each module uses a Likert scale ranging from 1-5, where 1 represents “strongly disagree” and 5 represents “strongly agree.” Utilizing an exploratory analysis, “all items showed good internal consistency (Cronbach’s alpha = 0.94) and test-retest reliability at 4 mo review (r = 0.82)”[71,114]. With regard to phobia diagnoses, positive results were found with regard to the convergent and predictive validity of the IDAF-4C+ when compared to Corah’s DAS, Eta2 = 0.154 and 0.060, respectively[71].
Diagnostic categories of dental fear
Individuals who are classified as “dentally anxious,” tend not to have qualities that can be catalogued. As such, they differ in their origin of fear, specific fear stimulus, age of onset, as well as the bodily reactions and psychological reactions that manifest in response to fear-related stimuli. The etiology of dental fear is wide-ranging and can be attributed to personal traumatic experiences (conditioning)[38], threats of dental visits as punishment (verbal threat pathway)[86,93], and fear through observing pain in loved ones and others (vicarious pathway) to name a few[50,99,115,116]. Moreover, at times, dental fear has been shown to be part of a larger “set” of fears such as arachnophobia and claustrophobia, and fears of mutilation and suffocation. Consequently, there has been debate on whether dental anxiety is a “simple” CS, or a component of a “set” of fears and mood or anxiety disorders[117]. Previous and well documented research has described these two variations of dental fear as exogenous and endogenous[118].
A group of researchers, well known for their clinical experience, developed a richer, more detailed classification system for dental fear. Their system, known as the Seattle System, mirrored the origin and the main stimuli of fear surrounding dental anxiety and phobias[116]. Essentially, the Seattle System can be used to classify individuals with respect to the severity of the psychological phobia relative to dentistry and the dentist as a person, based on a range of mean scores that represent different levels of dental fear. These mean scores have been applied to a number of questionnaires [i.e., DAS, Fear Survey Schedule II (FSSII), Spielberger Trait Anxiety Index (STA), Anxiety Sensitivity Index (ASI), Emotional Control Questionnaire (ECQ), General Health Questionnaire (GHQ), Fear of Pain Scale (FPS), and Mutilation Questionnaire (MQ)]. The Seattle System consists of four diagnostic elements: (1) simple CS of specific dental stimuli; (2) anxiety about somatic reactions during dental treatment; (3) patients with a generalized anxiety state and multi-phobic symptoms; and (4) distrust of dental personnel[116,119]. Despite the fact that the classification was originally designed for pragmatic academic purposes, it has shown to hold some evidence of psychologically valid identifications of dental anxiety subtypes[19]. Of note is the qualitative evaluation component of the Seattle System, which consists of in-depth interviews that give a more thorough understanding of the true multi-phobic nature that dental fear can present with[19]. Indeed, subjects with type 4 Seattle fear were further split into 3 subgroups, which met the criteria for distinct uniqueness, internal consistency, and distinct response to treatment type as proposed by earlier researchers[120].
Roughly comparable results were reported three years later utilizing the DSM-III-TR criteria for simple dental phobia (code 300.29-Specific phobia)[121]. However, although the results did not support the theory that the Seattle System corresponds to the DSM-III-TR, as proposed three years earlier[19], the researchers proposed that dentally anxious subjects should be calibrated for fear using a distinct method that differs from that for psychiatric mood and personality disorders[121]. Then, just before the turn of the century, newly published research brought to light some intriguing facts regarding the Seattle System[119]. Here, it was proposed that the Seattle System was valid from a psychological perspective in addition to being a well-rounded tool for clinical diagnosis (Table 1). Accordingly, they discovered that some participants in the older age brackets were of type 3 fear (Seattle System), indicating that those with simple phobias are able to recover in time, while those individuals with more complex multiphasic conditions may require psychological treatment[119].
Table 1.
Seattle system diagnostic criteria for dental phobia
| Fear type | Diagnostic Item | Classification of fear |
| Type 1 | Fear of dental procedures | Simple conditioned phobia |
| Type 2 | Fear of fainting, panic attack, heart attack | Fear of catastrophe |
| Type 3 | Nervous person in general | Generalized anxiety |
| Type 4 | Distrust of dentists | Fear of dentists |
| Subclass a | →High fear of dental procedures | |
| Subclass b | →Generally anxious | |
| Subclass c | →Fearful of dental catastrophes |
CURRENT MANAGEMENT TECHNIQUES FOR DENTAL FEAR AND ANXIETY (CBT)
With regard to treatment of dental fear and anxiety, there a number of possible avenues to explore with patients, including pre-treatment anxiety questionnaires, cognitive behavioral therapy (CBT), relaxation therapy, computer-assisted relaxation learning (CARL), hypnotherapy (HT), group therapy (GT), individual systematic desensitization (ISD), pharmacological, flooding (implosion), and swallowing relaxation. These forms of treatment are essentially a form of counter conditioning to reverse the fear into a state of acceptance and calm.
Pre-treatment anxiety questionnaires
To date, only one study exists as to general dentists’ use of pre-treatment anxiety questionnaires to assess patient anxiety before treatment. A study of United Kingdom dentists reported that only 20% of the dentists surveyed used adult anxiety questionnaires, and only 17% formally assessed children’s levels of fear and anxiety[122]. Interestingly the study reported that when treating adults, male dentist used pre-treatment fear surveys more often than female dentist (P < 0.05)[122]. The authors believe that these pre-treatment surveys can help enhance patient care; however it would be interesting to evaluate the current utilization rate of these anxiety surveys and methods to encourage this practice.
Individual systematic desensitization and group therapy
Individual systematic desensitization (ISD) is a behavioral therapy whereby individuals are gradually exposed or incrementally exposed to fearful stimuli. In this process, the individual must first identify and accept the fear-related stimulus; second, the individual must learn to employ a relaxation or coping technique; and finally, the individual must utilize the learned relaxation or coping strategy to react and overcome the fearful stimulus. In 2002, Moore et al[123] compared GT and ISD (as well as HT) and found that after 3 years, 65.5% of patients’ with ISD and 69.6% with GT maintained dental appointments (although these results were not significant). In this work, the ISD was a combination of muscle relaxation therapy and video reel exposures (looped) of threatening dental situations and instruments with intermittent tension awareness training and breath control lessons. GT involved groups of patients meeting for seven 2-h sessions led by a dentist, dental assistant, and successful former patient. Video desensitization reels were also played and a final demonstration of injection and drilling was performed at the last session. Unfortunately, Moore et al[123] (2002) did not identify the origin of fear for the participants. Thus, the current results cannot be extrapolated to the pathways and further research is needed.
Flooding/implosion
Flooding is a form of desensitization for treating phobias when the patient has a directly conditioned origin of fear (Origin 2). In flooding therapy, the patient is subjected to repeated exposure of fear-inducing stimuli until they no longer show a fear response, causing termination of the CR[124]. Implosion is used for either indirect conditioned or non-conditioned origins of fear (Origins 1 and 3) that may be imagined. However, the technique of flooding has not been examined in the literature since Mathews et al[125] in 1977. In this work, Mathews et al[126] report that among subjects who attended 2 or more flooding sessions, 48% successfully completed dental treatment 2 mo later. No further investigations appear to have been performed on this technique; this might be due to the highly anxiety-inducing nature of the treatment.
Cognitive behavioral therapy
Cognitive behavioral therapy (CBT) is a psychotherapeutic approach to address dysfunctional emotions and negative behaviors and cognitions using a series of goal-oriented sessions. Davies et al[126] (2011) found that of 21 patients offered CBT to overcome their dental fear as opposed to using sedation, 90% continued to be able to attend dental appointments without sedation ten years later. Current research appears to support CBT and relaxation therapy for treatment of directly conditioned fears (Origin 2)[127,128].
Relaxation therapy
Relaxation therapy is a diverse set of practices aimed at eliciting a relaxation response, including a reduction in overall physical arousal symptoms. The phobic individual implements a particular mental relaxation technique (e.g., slow breathing, counting, relaxation swallowing) to reduce stress. ten Berge et al[129] (2001) reported that parents play a more secondary role in treatment of child dental fear and anxiety. Results seem to suggest that CBT is more effective but should be combined with parental guidance in treatment of pediatric dental fear. Extrapolating this data, a combination of CBT and relaxation guidance may provide effective treatment of parental modeling dental fears (Origin 1).
Computer-assisted relaxation learning
A recent development in the treatment of dental fear, computer-assisted relaxation learning (CARL) is a self-paced treatment for dental phobic individuals for treating needle phobia. The program begins by introducing its purpose, followed by activities and videos on how to cope with their fear. The program is based on the theory of systematic desensitization and in a recent study in 2013, researchers compared CARL to information pamphlets (control) in a block randomized study[130]. The authors reported that CARL significantly reduced self-reported general and injection-specific dental anxiety (P < 0.001)[131]. After the intervention, twice as many CARL participants (35.3%) vs controls (17.6%) were comfortable enough to receive an injection though not significant (12 of 34)[131]. Participants’ origins of fear were not assessed, thus it cannot currently be determined which pathways were involved, and further research is required. However, as CARL is self-paced, it may perhaps aid in treating patients who wish to learn to cope without therapists, thereby improving access to oral health care.
Hypnotherapy
Perhaps one of the least understood treatments for dental fear is hypnotherapy (HT). HT attempts to create a state of unconscious change, whereby the individual forms new responses, attitudes, and behaviors to previously feared stimuli. Few studies have analyzed the clinical effectiveness of hypnotherapy. In 1995, research reported that when compared to psychophysiological therapies such as CBT, HT did not significantly reduce dental fear[132]. Researchers purported that this was because some people were put off by the concept of hypnotherapy and were not fully receptive to the therapy[132]. Some years later, Moore et al[123] (2002) found that although 54.5% of HT patients were able to maintain regular dental appointments, at 3 years post treatment, there was no difference between the HT, GT, or ISD groups.
Pharmacological
The use of nitrous oxide (NO) and benzodiazepines in dentistry has long been employed to reduce anxiety. NO has often been compared to the effectiveness of CBT and relaxation therapies. For example, Willumsen et al[133] (2001) reported no significant differences between NO and CBT or applied relaxation therapy. They suggested that in the short term, either treatment was effective. Interestingly the study reported a 95% of participants attended rate a year later, with the greatest reduction in dental fear observed in the relaxation therapy group[130]. While all groups reported normal levels of dental fear (as per Corah’s DAS) one year later[130], analysis of benzodiazepines when combined with ISD did not reduce overall therapy time and was not advantageous for treating injection phobia[134]. The studies did note that the results might have been skewed by the fact that each participant’s dental fear might have different origins. Thus, research is required to determine whether certain origins of fear and pathways are more receptive to pharmacological agents than others are.
CONCLUSION
The present article has highlighted the possible types of dental fear, their origins in dentistry and current knowledge on management of patient with fear and anxiety. There is, however, a lack of knowledge of the effects of demographics, causal factors, ethnicity, and treatment modalities relative to the origin and pathways of fear in dentistry. Understanding, the origin of a patient’s fears and anxiety could help enhance patient management and care.
Footnotes
P- Reviewer: Lopez-Jornet P, Oji C S- Editor: Ji FF L- Editor: A E- Editor: Lu YJ
References
- 1.Moore R, Birn H. [Phenomenon of dental fear] Tandlaegebladet. 1990;94:34–41. [PubMed] [Google Scholar]
- 2.Moore R, Brødsgaard I. Differential diagnosis of odontophobic patients using the DSM-IV. Eur J Oral Sci. 1995;103:121–126. doi: 10.1111/j.1600-0722.1995.tb00129.x. [DOI] [PubMed] [Google Scholar]
- 3.Armfield JM, Stewart JF, Spencer AJ. The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health. 2007;7:1. doi: 10.1186/1472-6831-7-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Armfield JM, Spencer AJ, Stewart JF. Dental fear in Australia: who’s afraid of the dentist? Aust Dent J. 2006;51:78–85. doi: 10.1111/j.1834-7819.2006.tb00405.x. [DOI] [PubMed] [Google Scholar]
- 5.Gross PR. Is pain sensitivity associated with dental avoidance? Behav Res Ther. 1992;30:7–13. doi: 10.1016/0005-7967(92)90090-4. [DOI] [PubMed] [Google Scholar]
- 6.Berggren U, Meynert G. Dental fear and avoidance: causes, symptoms, and consequences. J Am Dent Assoc. 1984;109:247–251. doi: 10.14219/jada.archive.1984.0328. [DOI] [PubMed] [Google Scholar]
- 7.Australian Research Centre for Population Oral Health. The avoidance and delaying of dental visits in Australia. Australia: University of Adelaide; 2012. pp. 1–5. [DOI] [PubMed] [Google Scholar]
- 8.Pohjola V, Mattila AK, Joukamaa M, Lahti S. Anxiety and depressive disorders and dental fear among adults in Finland. Eur J Oral Sci. 2011;119:55–60. doi: 10.1111/j.1600-0722.2010.00795.x. [DOI] [PubMed] [Google Scholar]
- 9.Mellor AC. Dental anxiety and attendance in the north-west of England. J Dent. 1992;20:207–210. doi: 10.1016/0300-5712(92)90077-p. [DOI] [PubMed] [Google Scholar]
- 10.Schwarz E, Birn H. Dental anxiety in Danish and Chinese adults--a cross-cultural perspective. Soc Sci Med. 1995;41:123–130. doi: 10.1016/0277-9536(94)00288-5. [DOI] [PubMed] [Google Scholar]
- 11.Ragnarsson E. Dental fear and anxiety in an adult Icelandic population. Acta Odontol Scand. 1998;56:100–104. doi: 10.1080/00016359850136067. [DOI] [PubMed] [Google Scholar]
- 12.Chellappah NK, Vignehsa H, Milgrom P, Lam LG. Prevalence of dental anxiety and fear in children in Singapore. Community Dent Oral Epidemiol. 1990;18:269–271. doi: 10.1111/j.1600-0528.1990.tb00075.x. [DOI] [PubMed] [Google Scholar]
- 13.Oosterink FM, de Jongh A, Hoogstraten J. Prevalence of dental fear and phobia relative to other fear and phobia subtypes. Eur J Oral Sci. 2009;117:135–143. doi: 10.1111/j.1600-0722.2008.00602.x. [DOI] [PubMed] [Google Scholar]
- 14.Kunzelmann KH, Dünninger P. Dental fear and pain: effect on patient’s perception of the dentist. Community Dent Oral Epidemiol. 1990;18:264–266. doi: 10.1111/j.1600-0528.1990.tb00073.x. [DOI] [PubMed] [Google Scholar]
- 15.Enkling N, Marwinski G, Jöhren P. Dental anxiety in a representative sample of residents of a large German city. Clin Oral Investig. 2006;10:84–91. doi: 10.1007/s00784-006-0035-6. [DOI] [PubMed] [Google Scholar]
- 16.Weinstein P, Shimono T, Domoto P, Wohlers K, Matsumura S, Ohmura M, Uchida H, Omachi K. Dental fear in Japan: Okayama Prefecture school study of adolescents and adults. Anesth Prog. 1992;39:215–220. [PMC free article] [PubMed] [Google Scholar]
- 17.Aartman IH, de Jongh A, Makkes PC, Hoogstraten J. Dental anxiety reduction and dental attendance after treatment in a dental fear clinic: a follow-up study. Community Dent Oral Epidemiol. 2000;28:435–442. doi: 10.1034/j.1600-0528.2000.028006435.x. [DOI] [PubMed] [Google Scholar]
- 18.Mehrstedt M, Tönnies S, Eisentraut I. Dental fears, health status, and quality of life. Anesth Prog. 2004;51:90–94. [PMC free article] [PubMed] [Google Scholar]
- 19.Moore R, Brødsgaard I, Birn H. Manifestations, acquisition and diagnostic categories of dental fear in a self-referred population. Behav Res Ther. 1991;29:51–60. doi: 10.1016/s0005-7967(09)80007-7. [DOI] [PubMed] [Google Scholar]
- 20.Berggren U, Carlsson SG, Gustafsson JE, Hakeberg M. Factor analysis and reduction of a Fear Survey Schedule among dental phobic patients. Eur J Oral Sci. 1995;103:331–338. doi: 10.1111/j.1600-0722.1995.tb00035.x. [DOI] [PubMed] [Google Scholar]
- 21.Moore R, Brødsgaard I, Rosenberg N. The contribution of embarrassment to phobic dental anxiety: a qualitative research study. BMC Psychiatry. 2004;4:10. doi: 10.1186/1471-244X-4-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gregory AM, Eley TC. Genetic influences on anxiety in children: what we’ve learned and where we’re heading. Clin Child Fam Psychol Rev. 2007;10:199–212. doi: 10.1007/s10567-007-0022-8. [DOI] [PubMed] [Google Scholar]
- 23.Hettema JM, Annas P, Neale MC, Fredrikson M, Kendler KS. The genetic covariation between fear conditioning and self-report fears. Biol Psychiatry. 2008;63:587–593. doi: 10.1016/j.biopsych.2007.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fyer AJ, Mannuzza S, Chapman TF, Martin LY, Klein DF. Specificity in familial aggregation of phobic disorders. Arch Gen Psychiatry. 1995;52:564–573. doi: 10.1001/archpsyc.1995.03950190046007. [DOI] [PubMed] [Google Scholar]
- 25.Rose RJ, Miller JZ, Pogue-Geile MF, Cardwell GF. Twin-family studies of common fears and phobias. Prog Clin Biol Res. 1981;69 Pt B:169–174. [PubMed] [Google Scholar]
- 26.Skre I, Onstad S, Torgersen S, Philos DR, Lygren S, Kringlen E. The heritability of common phobic fear: a twin study of a clinical sample. J Anxiety Disord. 2000;14:549–562. doi: 10.1016/s0887-6185(00)00049-9. [DOI] [PubMed] [Google Scholar]
- 27.Kressin NR, Spiro A, Skinner KM. Negative affectivity and health-related quality of life. Med Care. 2000;38:858–867. doi: 10.1097/00005650-200008000-00009. [DOI] [PubMed] [Google Scholar]
- 28.Mineka S, Ohman A. Phobias and preparedness: the selective, automatic, and encapsulated nature of fear. Biol Psychiatry. 2002;52:927–937. doi: 10.1016/s0006-3223(02)01669-4. [DOI] [PubMed] [Google Scholar]
- 29.Seligman MEP. Phobias and Preparedness. Behav Ther. 1971;2:307–320. [Google Scholar]
- 30.Wolpe J. The dichotomy between classical conditioned and cognitively learned anxiety. J Behav Ther Exp Psychiatry. 1981;12:35–42. doi: 10.1016/0005-7916(81)90027-6. [DOI] [PubMed] [Google Scholar]
- 31.Hosoba T, Iwanaga M, Seiwa H. The effect of UCS inflation and deflation procedures on ‘fear’ conditioning. Behav Res Ther. 2001;39:465–475. doi: 10.1016/s0005-7967(00)00025-5. [DOI] [PubMed] [Google Scholar]
- 32.Kryukov VI. Towards a unified model of pavlovian conditioning: short review of trace conditioning models. Cogn Neurodyn. 2012;6:377–398. doi: 10.1007/s11571-012-9195-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Watson JB, Rayner R. Conditioned Emotional Reactions. J Exp Psychol. 1920;3:1–14. doi: 10.1037//0003-066x.55.3.313. [DOI] [PubMed] [Google Scholar]
- 34.Mineka S, Keir R. The effects of flooding on reducing snake fear in rhesus monkeys: 6-month follow-up and further flooding. Behav Res Ther. 1983;21:527–535. doi: 10.1016/0005-7967(83)90044-x. [DOI] [PubMed] [Google Scholar]
- 35.Hugdahl K. Direction of changes in the cardiac component in a Pavlovian conditioning paradigm with variations in CS- and UCS-contents. Biol Psychol. 1979;9:91–102. doi: 10.1016/0301-0511(79)90056-5. [DOI] [PubMed] [Google Scholar]
- 36.Rachman S. The conditioning theory of fear-acquisition: a critical examination. Behav Res Ther. 1977;15:375–387. doi: 10.1016/0005-7967(77)90041-9. [DOI] [PubMed] [Google Scholar]
- 37.Merckelbach H, Arntz A, de Jong P. Conditioning experiences in spider phobics. Behav Res Ther. 1991;29:333–335. doi: 10.1016/0005-7967(91)90068-e. [DOI] [PubMed] [Google Scholar]
- 38.Cook M, Mineka S. Observational conditioning of fear to fear-relevant versus fear-irrelevant stimuli in rhesus monkeys. J Abnorm Psychol. 1989;98:448–459. doi: 10.1037//0021-843x.98.4.448. [DOI] [PubMed] [Google Scholar]
- 39.Wolpe J, Lande SD, McNally RJ, Schotte D. Differentiation between classically conditioned and cognitively based neurotic fears: two pilot studies. J Behav Ther Exp Psychiatry. 1985;16:287–293. doi: 10.1016/0005-7916(85)90002-3. [DOI] [PubMed] [Google Scholar]
- 40.Mowrer OH. Learning theory and the symbolic processes. London: UK; 1960. Available from: http://www.abebooks.co.uk/Learning-Theory-Symbolic-Process-Mowrer-O.H/857643055/bd. [Google Scholar]
- 41.Rachman S. Fear and Courage. San Francisco: Freeman; 1978. Available from: http://trove.nla.gov.au/work/11583705?selectedversion=NBD1120715. [Google Scholar]
- 42.Askew C, Field AP. The vicarious learning pathway to fear 40 years on. Clin Psychol Rev. 2008;28:1249–1265. doi: 10.1016/j.cpr.2008.05.003. [DOI] [PubMed] [Google Scholar]
- 43.Carrillo-Díaz M, Crego A, Armfield J, Romero M. The moderating role of dental expectancies on the relationship between cognitive vulnerability and dental fear in children and adolescents. Community Dent Oral Epidemiol. 2013;41:269–278. doi: 10.1111/cdoe.12009. [DOI] [PubMed] [Google Scholar]
- 44.Carrillo-Diaz M, Crego A, Armfield JM, Romero-Maroto M. Treatment experience, frequency of dental visits, and children’s dental fear: a cognitive approach. Eur J Oral Sci. 2012;120:75–81. doi: 10.1111/j.1600-0722.2011.00921.x. [DOI] [PubMed] [Google Scholar]
- 45.Waters AM, Wharton TA, Zimmer-Gembeck MJ, Craske MG. Threat-based cognitive biases in anxious children: comparison with non-anxious children before and after cognitive behavioural treatment. Behav Res Ther. 2008;46:358–374. doi: 10.1016/j.brat.2008.01.002. [DOI] [PubMed] [Google Scholar]
- 46.Klingberg G, Broberg AG. Dental fear/anxiety and dental behaviour management problems in children and adolescents: a review of prevalence and concomitant psychological factors. Int J Paediatr Dent. 2007;17:391–406. doi: 10.1111/j.1365-263X.2007.00872.x. [DOI] [PubMed] [Google Scholar]
- 47.Themessl-Huber M, Freeman R, Humphris G, MacGillivray S, Terzi N. Empirical evidence of the relationship between parental and child dental fear: a structured review and meta-analysis. Int J Paediatr Dent. 2010;20:83–101. doi: 10.1111/j.1365-263X.2009.00998.x. [DOI] [PubMed] [Google Scholar]
- 48.Pine DS, Klein RG. Anxiety Disorders. In: Rutter’s Child and Adolescent Psychiatry, Rutter M., editors. Oxford UK: Blackwell Publishing Ltd; 2009. [Google Scholar]
- 49.ten Berge M, Veerkamp JS, Hoogstraten J, Prins PJ. Childhood dental fear in relation to parental child-rearing attitudes. Psychol Rep. 2003;92:43–50. doi: 10.2466/pr0.2003.92.1.43. [DOI] [PubMed] [Google Scholar]
- 50.Coelho MC, Purkis H, The Origins of Specific Phobias: Influential Theories and current Perspectives. RGP. 2009;13:335–348. [Google Scholar]
- 51.Seligman MEP. On the generality of the laws of learning. Psychological Review. 1970;77:406–418. [Google Scholar]
- 52.Mineka S, Ohman A. Born to fear: non-associative vs associative factors in the etiology of phobias. Behav Res Ther. 2002;40:173–184. doi: 10.1016/s0005-7967(01)00050-x. [DOI] [PubMed] [Google Scholar]
- 53.Poulton R, Menzies RG. Fears born and bred: toward a more inclusive theory of fear acquisition. Behav Res Ther. 2002;40:197–208. doi: 10.1016/s0005-7967(01)00052-3. [DOI] [PubMed] [Google Scholar]
- 54.Poulton R, Menzies RG. Non-associative fear acquisition: a review of the evidence from retrospective and longitudinal research. Behav Res Ther. 2002;40:127–149. doi: 10.1016/s0005-7967(01)00045-6. [DOI] [PubMed] [Google Scholar]
- 55.Menzies RG, Clarke JC. The etiology of childhood water phobia. Behav Res Ther. 1993;31:499–501. doi: 10.1016/0005-7967(93)90131-d. [DOI] [PubMed] [Google Scholar]
- 56.Menzies RG, Clarke JC. The etiology of fear of heights and its relationship to severity and individual response patterns. Behav Res Ther. 1993;31:355–365. doi: 10.1016/0005-7967(93)90093-a. [DOI] [PubMed] [Google Scholar]
- 57.Muris P, Steerneman P, Merckelbach H, Meesters C. The role of parental fearfulness and modeling in children’s fear. Behav Res Ther. 1996;34:265–268. doi: 10.1016/0005-7967(95)00067-4. [DOI] [PubMed] [Google Scholar]
- 58.Klingberg G, Berggren U, Carlsson SG, Noren JG. Child dental fear: cause-related factors and clinical effects. Eur J Oral Sci. 1995;103:405–412. doi: 10.1111/j.1600-0722.1995.tb01865.x. [DOI] [PubMed] [Google Scholar]
- 59.Brush RF, Overmier BJ. Affect conditioning and cognition: Essays on the determinants of behavior. Hillsdale (NJ): Lawrence Erlbaum Associates; 1985. [Google Scholar]
- 60.Morgan JB, Watson JB. Emotional reactions and psychological experimentation. By John B. Watson and J. J. B. Morgan, 1917. Am J Psychol. 1917;100:510–537. [PubMed] [Google Scholar]
- 61.Carter A. Development of a Dental Fear Questionnaire: the role of Ethnicity in Endodontic Fear and Anxiety. Gold Coast (Australia): Doctoral Dissertation, School of Dentistry and Oral Health, Griffith University; 2012. [Google Scholar]
- 62.Ost LG, Hugdahl K. Acquisition of blood and dental phobia and anxiety response patterns in clinical patients. Behav Res Ther. 1985;23:27–34. doi: 10.1016/0005-7967(85)90139-1. [DOI] [PubMed] [Google Scholar]
- 63.Kudo T, Mishima R, Yamamura K, Mostafeezur R, Zakir HM, Kurose M, Yamada Y. Difference in physiological responses to sound stimulation in subjects with and without fear of dental treatments. Odontology. 2008;96:44–49. doi: 10.1007/s10266-008-0086-z. [DOI] [PubMed] [Google Scholar]
- 64.Watkins CA, Logan HL, Kirchner HL. Anticipated and experienced pain associated with endodontic therapy. J Am Dent Assoc. 2002;133:45–54. doi: 10.14219/jada.archive.2002.0020. [DOI] [PubMed] [Google Scholar]
- 65.van Wijk AJ, Hoogstraten J. Experience with dental pain and fear of dental pain. J Dent Res. 2005;84:947–950. doi: 10.1177/154405910508401014. [DOI] [PubMed] [Google Scholar]
- 66.Armfield JM. Towards a better understanding of dental anxiety and fear: cognitions vs. experiences. Eur J Oral Sci. 2010;118:259–264. doi: 10.1111/j.1600-0722.2010.00740.x. [DOI] [PubMed] [Google Scholar]
- 67.De Jongh A, van der Burg J, van Overmeir M, Aartman I, van Zuuren FJ. Trauma-related sequelae in individuals with a high level of dental anxiety. Does this interfere with treatment outcome? Behav Res Ther. 2002;40:1017–1029. doi: 10.1016/s0005-7967(01)00081-x. [DOI] [PubMed] [Google Scholar]
- 68.Hakeberg M, Berggren U. Dimensions of the Dental Fear Survey among patients with dental phobia. Acta Odontol Scand. 1997;55:314–318. doi: 10.3109/00016359709114970. [DOI] [PubMed] [Google Scholar]
- 69.Ollendick TH, King NJ. Origins of childhood fears: an evaluation of Rachman’s theory of fear acquisition. Behav Res Ther. 1991;29:117–123. doi: 10.1016/0005-7967(91)90039-6. [DOI] [PubMed] [Google Scholar]
- 70.Stabholz A, Peretz B. Dental anxiety among patients prior to different dental treatments. Int Dent J. 1999;49:90–94. doi: 10.1111/j.1875-595x.1999.tb00514.x. [DOI] [PubMed] [Google Scholar]
- 71.Armfield JM. Development and psychometric evaluation of the Index of Dental Anxiety and Fear (IDAF-4C+) Psychol Assess. 2010;22:279–287. doi: 10.1037/a0018678. [DOI] [PubMed] [Google Scholar]
- 72.Berggren U. General and specific fears in referred and self-referred adult patients with extreme dental anxiety. Behav Res Ther. 1992;30:395–401. doi: 10.1016/0005-7967(92)90051-h. [DOI] [PubMed] [Google Scholar]
- 73.Domoto PK, Weinstein P, Melnick S, Ohmura M, Uchida H, Ohmachi K, Hori M, Okazaki Y, Shimamoto T, Matsumura S. Results of a dental fear survey in Japan: implications for dental public health in Asia. Community Dent Oral Epidemiol. 1988;16:199–201. doi: 10.1111/j.1600-0528.1988.tb01753.x. [DOI] [PubMed] [Google Scholar]
- 74.Locker D, Liddell A, Dempster L, Shapiro D. Age of onset of dental anxiety. J Dent Res. 1999;78:790–796. doi: 10.1177/00220345990780031201. [DOI] [PubMed] [Google Scholar]
- 75.Armfield JM, Slade GD, Spencer AJ. Are people with dental fear under-represented in oral epidemiological surveys? Soc Psychiatry Psychiatr Epidemiol. 2009;44:495–500. doi: 10.1007/s00127-008-0454-6. [DOI] [PubMed] [Google Scholar]
- 76.Armfield JM, Slade GD, Spencer AJ. Cognitive vulnerability and dental fear. BMC Oral Health. 2008;8:2. doi: 10.1186/1472-6831-8-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Kleinknecht RA, Thorndike RM, McGlynn FD, Harkavy J. Factor analysis of the dental fear survey with cross-validation. J Am Dent Assoc. 1984;108:59–61. doi: 10.14219/jada.archive.1984.0193. [DOI] [PubMed] [Google Scholar]
- 78.Lindsay SJ, Wege P, Yates J. Expectations of sensations, discomfort and fear in dental treatment. Behav Res Ther. 1984;22:99–108. doi: 10.1016/0005-7967(84)90098-6. [DOI] [PubMed] [Google Scholar]
- 79.Cook M, Mineka S. Selective associations in the observational conditioning of fear in rhesus monkeys. J Exp Psychol Anim Behav Process. 1990;16:372–389. [PubMed] [Google Scholar]
- 80.Smith TA, Heaton LJ. Fear of dental care: are we making any progress? J Am Dent Assoc. 2003;134:1101–1108. doi: 10.14219/jada.archive.2003.0326. [DOI] [PubMed] [Google Scholar]
- 81.Field AP. Watch out for the beast: fear information and attentional bias in children. J Clin Child Adolesc Psychol. 2006;35:431–439. doi: 10.1207/s15374424jccp3503_8. [DOI] [PubMed] [Google Scholar]
- 82.Field AP, Cartwright-Hatton S, Reynolds S, Creswell C. Future directions for child anxiety theory and treatment. Cognition and Emotion. 2008;22:385–394. [Google Scholar]
- 83.Field AP . Lang. The cognitive psychopathology of emotion: Fear and anxiety, in Anxiety and the anxiety disorders. In: Tuma A, Maser J, editors. Hillsdale (NJ): Lawrence Erlbaum Associates; 1985. pp. 131–170. [Google Scholar]
- 84.Field AP, Ball JE, Kawycz NJ, Moore H. Parent-child relations and the verbal information pathway to fear in children: Two preliminary experiments. Behavioural and Cognitive Psychotherapy. 2007;35:473–486. [Google Scholar]
- 85.Field A, Lawson J. The verbal information pathway to fear and subsequent causal learning in children. Cognition and Emotion. 2008;22:459–479. [Google Scholar]
- 86.Field AP, Lawson J, Banerjee R. The verbal threat information pathway to fear in children: the longitudinal effects on fear cognitions and the immediate effects on avoidance behavior. J Abnorm Psychol. 2008;117:214–224. doi: 10.1037/0021-843X.117.1.214. [DOI] [PubMed] [Google Scholar]
- 87.Muris P, Field AP. The role of verbal threat information in the development of childhood fear. “Beware the Jabberwock!”. Clin Child Fam Psychol Rev. 2010;13:129–150. doi: 10.1007/s10567-010-0064-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Adelaide TUO. Dr Jason Armfield, Senior Research Fellow. Available from: http: //www.arcpoh.adelaide.edu.au/people/html/jason.html [retrieved 11/09/13]
- 89.Field AP, Graham D. Anxiety disorders in children and adolescents: research, assessment and intervention. In: conditioning models of childhood anxiety., editor. Silverman WK, Treffers PA, editors. Cambridge (UK): Cambridge University Press; 2001. pp. 187–211. [Google Scholar]
- 90.Field AP, Hamilton SJ, Knowles KA, Plews EL. Fear information and social phobic beliefs in children: a prospective paradigm and preliminary results. Behav Res Ther. 2003;41:113–123. doi: 10.1016/s0005-7967(02)00050-5. [DOI] [PubMed] [Google Scholar]
- 91.Field AP, Lawson J. Fear information and the development of fears during childhood: effects on implicit fear responses and behavioural avoidance. Behav Res Ther. 2003;41:1277–1293. doi: 10.1016/s0005-7967(03)00034-2. [DOI] [PubMed] [Google Scholar]
- 92.Field A, Lester KJ. Learning of information processing biases in anxious children and adolescents. In: Information processing biases and anxiety: A developmental perspective., editor. Hadwin J, Field A, editors. Chichester (UK): Wiley and Sons Ltd; 2010. [Google Scholar]
- 93.Van Kraaij C, Breukink E, Rollema HS, Siezen RJ, Demel RA, De Kruijff B, Kuipers OP. Influence of charge differences in the C-terminal part of nisin on antimicrobial activity and signaling capacity. Eur J Biochem. 1997;247:114–120. doi: 10.1111/j.1432-1033.1997.00114.x. [DOI] [PubMed] [Google Scholar]
- 94.Field AP, Schorah H. The verbal information pathway to fear and heart rate changes in children. J Child Psychol Psychiatry. 2007;48:1088–1093. doi: 10.1111/j.1469-7610.2007.01772.x. [DOI] [PubMed] [Google Scholar]
- 95.Field AP, Storksen-Coulson H. The interaction of pathways to fear in childhood anxiety: a preliminary study. Behav Res Ther. 2007;45:3051–3059. doi: 10.1016/j.brat.2007.09.001. [DOI] [PubMed] [Google Scholar]
- 96.Field AP, Argyris NG, Knowles KA. Who’s afraid of the big bad wolf: a prospective paradigm to test Rachman’s indirect pathways in children. Behav Res Ther. 2001;39:1259–1276. doi: 10.1016/s0005-7967(00)00080-2. [DOI] [PubMed] [Google Scholar]
- 97.Field A, Lester K, Cartwright-Hatton S. Cognitive-behavioral processes in the intergenerational transmission of fear to children. USA: Annual congress of the association for the advancement of behavior and cognitive therapy; 2008. [Google Scholar]
- 98.Antony MM, Orsillo SM, Roemer L. Practitioners guide to emperically based measures of anxiety. 1st ed. New York (USA): Springer; 2001. [Google Scholar]
- 99.Ost LG, Hugdahl K. Acquisition of phobias and anxiety response patterns in clinical patients. Behav Res Ther. 1981;19:439–447. doi: 10.1016/0005-7967(81)90134-0. [DOI] [PubMed] [Google Scholar]
- 100.Kirkby KC, Menzies RG, Daniels BA, Smith KL. Aetiology of spider phobia: classificatory differences between two origins instruments. Behav Res Ther. 1995;33:955–958. doi: 10.1016/0005-7967(95)00010-u. [DOI] [PubMed] [Google Scholar]
- 101.Menzies RG, Clarke JC. Retrospective studies of the origins of phobias: A review. Anxiety, Stress and Coping: An International Journal. 1994;7:305–318. [Google Scholar]
- 102.McNeil DW, Rainwater AJ. Development of the Fear of Pain Questionnaire--III. J Behav Med. 1998;21:389–410. doi: 10.1023/a:1018782831217. [DOI] [PubMed] [Google Scholar]
- 103.Menzies RG, Kirkby K, Harris LM. The convergent validity of the Phobia Origins Questionnaire (POQ): a review of the evidence. Behav Res Ther. 1998;36:1081–1089. doi: 10.1016/s0005-7967(98)00067-9. [DOI] [PubMed] [Google Scholar]
- 104.Merckelbach H, van Hout W, van den Hout MA, Mersch PP. Psychophysiological and subjective reactions of social phobics and normals to facial stimuli. Behav Res Ther. 1989;27:289–294. doi: 10.1016/0005-7967(89)90048-x. [DOI] [PubMed] [Google Scholar]
- 105.Fazio AF. Implosive therapy with semiclinical phobias. J Abnorm Psychol. 1972;80:183–188. doi: 10.1037/h0033568. [DOI] [PubMed] [Google Scholar]
- 106.Kleinknecht RD. The origins and remission of fear in a group of tarantula enthusiasts. Behav Res Ther. 1982;20:437–443. [Google Scholar]
- 107.Rimm DC, Janda LH, Lancaster DW, Nahl M, Dittmar K. An exploratory investigation of the origin and maintenance of phobias. Behav Res Ther. 1977;15:231–238. doi: 10.1016/0005-7967(77)90020-1. [DOI] [PubMed] [Google Scholar]
- 108.Marks IM. Fears phobias and rituals: Panic, anxiety and their disorders. New York: Oxford Univeristy Press; 1987. [Google Scholar]
- 109.Mattick R. Nature and treatment of social phobia: Unpublished Doctoral Dissertation. Syndey: University of New South Wales; 1987. [Google Scholar]
- 110.Menzies RG. The origins of specific phobias in a mixed clinical sample: Classificatory differences between two origins instruments. J ANXIETY. DISORD. 1996;10:347–354. [Google Scholar]
- 111.Withers RD, Deane FP. Origins of common fears: effects on severity, anxiety responses and memories of onset. Behav Res Ther. 1995;33:903–915. doi: 10.1016/0005-7967(95)00044-x. [DOI] [PubMed] [Google Scholar]
- 112.Schuurs AH, Hoogstraten J. Appraisal of dental anxiety and fear questionnaires: a review. Community Dent Oral Epidemiol. 1993;21:329–339. doi: 10.1111/j.1600-0528.1993.tb01095.x. [DOI] [PubMed] [Google Scholar]
- 113.Armfield JM. How do we measure dental fear and what are we measuring anyway? Oral Health Prev Dent. 2010;8:107–115. [PubMed] [Google Scholar]
- 114.Armfield JM. Australian population norms for the Index of Dental Anxiety and Fear (IDAF-4C) Aust Dent J. 2011;56:16–22. doi: 10.1111/j.1834-7819.2010.01279.x. [DOI] [PubMed] [Google Scholar]
- 115.Milgrom P, Fiset L, Melnick S, Weinstein P. The prevalence and practice management consequences of dental fear in a major US city. J Am Dent Assoc. 1988;116:641–647. doi: 10.14219/jada.archive.1988.0030. [DOI] [PubMed] [Google Scholar]
- 116.Milgrom P. Treating Fearful Dental Patients: A Patient Management Handbook. Reston (Va): Reston Pub. Co; 1985. [Google Scholar]
- 117.McNeil DW, Berryman ML. Components of dental fear in adults? Behav Res Ther. 1989;27:233–236. doi: 10.1016/0005-7967(89)90041-7. [DOI] [PubMed] [Google Scholar]
- 118.Weiner AA, Sheehan DV. Etiology of dental anxiety: psychological trauma or CNS chemical imbalance? Gen Dent. 1990;38:39–43. [PubMed] [Google Scholar]
- 119.Locker D, Liddell A, Shapiro D. Diagnostic categories of dental anxiety: a population-based study. Behav Res Ther. 1999;37:25–37. doi: 10.1016/s0005-7967(98)00105-3. [DOI] [PubMed] [Google Scholar]
- 120.Sheehan DV, Sheehan KH. The classification of phobic disorders. Int J Psychiatry Med. 1983;12:243–266. doi: 10.2190/lna4-1u6e-9wtw-31ju. [DOI] [PubMed] [Google Scholar]
- 121.Roy-Byrne PP, Milgrom P, Khoon-Mei T, Weinstein P, Katon W. Psychopathology and psychiatric diagnosis in subjects with dental phobia. JAD. 1994;8:19–31. [Google Scholar]
- 122.Dailey YM, Humphris GM, Lennon MA. The use of dental anxiety questionnaires: a survey of a group of UK dental practitioners. Br Dent J. 2001;190:450–453. doi: 10.1038/sj.bdj.4801000. [DOI] [PubMed] [Google Scholar]
- 123.Moore R, Brødsgaard I, Abrahamsen R. A 3-year comparison of dental anxiety treatment outcomes: hypnosis, group therapy and individual desensitization vs. no specialist treatment. Eur J Oral Sci. 2002;110:287–295. doi: 10.1034/j.1600-0722.2002.21234.x. [DOI] [PubMed] [Google Scholar]
- 124.American Psychological Association. APA Dictionary of Psychology. USA: APA; 2006. [Google Scholar]
- 125.Mathews A, Rezin V. Treatment of dental fears by imaginal flooding and rehearsal of coping behaviour. Behav Res Ther. 1977;15:321–328. doi: 10.1016/0005-7967(77)90063-8. [DOI] [PubMed] [Google Scholar]
- 126.Davies JG, Wilson KI, Clements AL. A joint approach to treating dental phobia: a re-evaluation of a collaboration between community dental services and specialist psychotherapy services ten years on. Br Dent J. 2011;211:159–162. doi: 10.1038/sj.bdj.2011.674. [DOI] [PubMed] [Google Scholar]
- 127.Lundgren J, Carlsson SG, Berggren U. Relaxation versus cognitive therapies for dental fear--a psychophysiological approach. Health Psychol. 2006;25:267–273. doi: 10.1037/0278-6133.25.3.267. [DOI] [PubMed] [Google Scholar]
- 128.Berggren U, Hakeberg M, Carlsson SG. Relaxation vs. cognitively oriented therapies for dental fear. J Dent Res. 2000;79:1645–1651. doi: 10.1177/00220345000790090201. [DOI] [PubMed] [Google Scholar]
- 129.ten Berge M, Veerkamp JS, Hoogstraten J, Prins PJ. Parental beliefs on the origins of child dental fear in The Netherlands. ASDC J Dent Child. 2001;68:51–54, 12. [PubMed] [Google Scholar]
- 130.Willumsen T, Vassend O, Hoffart A. One-year follow-up of patients treated for dental fear: effects of cognitive therapy, applied relaxation, and nitrous oxide sedation. Acta Odontol Scand. 2001;59:335–340. doi: 10.1080/000163501317153167. [DOI] [PubMed] [Google Scholar]
- 131.Heaton LJ, Leroux BG, Ruff PA, Coldwell SE. Computerized dental injection fear treatment: a randomized clinical trial. J Dent Res. 2013;92:37S–42S. doi: 10.1177/0022034513484330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Stivala F, Bonina F, Iacona G, Cordopatri F, Mazzone G. [Effects of lymphocyte stimulation in vitro of alkaline salts of some aroyl-hydrazino-carbodithioic acids and 1,3,4-oxadiazole derivatives: preliminary research] Boll Soc Ital Biol Sper. 1978;54:1264–1270. [PubMed] [Google Scholar]
- 133.Willumsen T, Vassend O, Hoffart A. A comparison of cognitive therapy, applied relaxation, and nitrous oxide sedation in the treatment of dental fear. Acta Odontol Scand. 2001;59:290–296. doi: 10.1080/000163501750541156. [DOI] [PubMed] [Google Scholar]
- 134.Coldwell SE, Wilhelm FH, Milgrom P, Prall CW, Getz T, Spadafora A, Chiu IY, Leroux BG, Ramsay DS. Combining alprazolam with systematic desensitization therapy for dental injection phobia. J Anxiety Disord. 2007;21:871–887. doi: 10.1016/j.janxdis.2007.01.001. [DOI] [PubMed] [Google Scholar]