

Abstract
The purposes of the present study were to investigate if a) shuttle-run sprint training performed in a normobaric hypoxia chamber of limited size (4.75x2.25m) is feasible, in terms of producing the same absolute training load, when compared to training in normoxia, and b) if such training improves the repeated sprint ability (RSA) and the Yo-Yo intermittent recovery (YYIR) test outcome in young elite soccer players. Players of an elite soccer training Centre (age: 15.3 ± 0.5 years, height: 1.73 ± 0.07 m, body mass: 62.6 ± 6.6 kg) were randomly assigned to a hypoxia or a normoxia training group. Within a 5-week period, players, who were not informed about the hypoxia intervention, performed at least 7 sessions of identical shuttle-run sprint training either in a normal training room (FiO2 = 20.95%) or in a hypoxic chamber (FiO2 = 14.8%; approximately 3300m), both equipped with the same floor. Each training session comprised 3 series of 5x10s back and forth sprints (4.5m) performed at maximal intensity. Recovery time between repetitions was 20s and between series 5min. Before and after the training period the RSA (6 x 40m shuttle sprint with 20 s rest between shuttles) and the YYIR test were performed. The size of the chamber did not restrict the training intensity of the sprint training (both groups performed approximately 8 shuttles during 10s). Training in hypoxia resulted in a lower fatigue slope which indicates better running speed maintenance during the RSA test (p = 0.024). YYIR performance increased over time (p = 0.045) without differences between groups (p > 0.05). This study showed that training intensity of the shuttle-run sprint training was not restricted in a hypoxic chamber of limited size which indicates that such training is feasible. Furthermore, hypoxia compared to normoxia training reduced the fatigue slope during the RSA test in youth soccer players.
Key Points.
Shuttle-run sprint training is feasible in hypoxic chambers of limited size (i.e., 4.75x2.25m).
Hypoxia sprint training (RSH), in comparison to normoxia training, might lead to better running speed maintenance during the repeated sprint ability test.
Key words: Altitude training, football, high intensity training, repeated sprint ability, Yo-Yo test
Introduction
Important performance characteristics of soccer players are excellent repeated sprint ability (RSA) and performance in the Yo-Yo intermittent recovery test (YYIR) (Krustrup et al., 2006; Rampinini et al., 2009). Both are associated with in-match physical performance (Krustrup et al., 2006; Rampinini et al., 2007) and influenced by a fast VO2 kinetic and a high buffer capacity (Dupont et al., 2010; Girard et al., 2011). Furthermore, RSA was shown to depend on maximal aerobic power (VO2max), muscle glycogen content, concentration of aerobic enzymes, mitochondrial size and number and capillary density (Dupont et al., 2010; Girard et al., 2011; Rampinini et al., 2009). Based on the observations that high intensity training under hypoxia likely improves buffer capacity (Faiss et al., 2013a; 2013b; Girard et al., 2013a), lactate exchange and removal, tissue O2 extraction (Faiss et al., 2013a; 2013b; Girard et al., 2013a), glycolytic enzyme activity (Hamlin et al., 2010; Puype et al., 2013), economy (Hamlin et al., 2010), citrate synthase activity and myoglobin content (Terrados et al., 1990), it could be speculated that this type of training might improve RSA and YYIR and thus influence physical soccer performance. Accordingly, Faiss et al. (2013a) found greater improvements in RSA (i.e., increased number of sprints until exhaustion) and Galvin et al. (2013) greater improvement in the YYIR test performance after repeated sprint training in hypoxia (RSH) compared to normoxic training (RSN). However, the training intervention was performed on cycle ergometers (Faiss et al., 2013a) which represents an unusual activity for soccer players or on a non-motorised treadmill (Galvin et al., 2013). For obvious reasons soccer coaches generally might be reluctant in adopting these procedures. Therefore new training regimes and/or new technologies are requested that overcome this restriction. The mobile inflatable hypoxic marquees as described in detail by Girard et al. (2013b) can be considered such a new and promising technology. However many research and training Centres are equipped with much smaller hypoxic chambers not allowing performing long distance sprints. Therefore, the present study aimed at investigating if performing shuttle-run sprint training - presumably reflecting a more common soccer training practice as cycling or running on a non-motorised treadmill - is feasible in a normobaric hypoxia chamber of limited size (4.75 x 2.25 m) and if such training improves RSA and YYIR test outcomes. We hypothesized that the proposed shuttle-run sprint training can be performed in small hypoxic chambers without restricting training intensity and that RSH improves RSA and YYIR test outcomes to a greater extent than RSN.
Methods
Participants
Sixteen healthy male youth soccer players (outfield players, age 15.3 ± 0.5 years, body height 1.73 ± 0.07 m and body mass 62.6 ± 6.6 kg) of an elite Tyrolean soccer training Centre were informed about the training protocol and gave written informed consent to participate in the study. Players were randomly assigned to a normoxia or a hypoxia training group according to their RSA and YYIR performance. Three players of the control group and 3 players of the hypoxia group dropped out because of longer lasting illnesses and injuries during the training period. Additionally one player skipped the second YYIR test due to the feeling of discomfort. Players were not familiar with the training modalities described in detail below. The study was carried out in conformity with the ethical standards laid down in the 1975 declaration of Helsinki and has been approved by the Institutional Review Board of the Department of Sport Science, University of Innsbruck.
Experimental design
The shuttle-run sprint training started in the third week of the winter preparation phase and was arranged in agreement with the coaches. Besides the normal training regime, which was the same for both groups, 8 sessions (participants performing only 7 sessions were also included into analyses; reasons: colds, School engagement, minor injury) of a shuttle-run sprint training program was performed during a 5 week period. The training was performed each week on Tuesday and Thursday. Because of the 5 week training period participants were allowed to be absent not more than 3 times, with the request that at least one training session had to be completed during the last week. The training was performed in an air-conditioned (21°C) normobaric hypoxic chamber (size 4.75 x 2.25m, LowOxygen, Germany). For the hypoxia group the FiO2 was set at 14.8%, equivalent to approximately 3300m, shown not to reduce peak power output in repeated sprint efforts (Goods et al., 2014). The normoxia group trained in a separate training room under the same conditions in terms of floor conditions and cone distance at a FiO2 of 20.95%. Group assignment was blinded to the players (single blinded study design) as players were not informed about the hypoxia intervention and were not conscious of this technique. We considered this to be ethically acceptable as no complications were expected to occur with this training modality. One week before and one week after the shuttle-run sprint training period the RSA and the YYIR test were performed.
Testing protocol
The RSA test consisted of 6 x 40m sprints (20m back and forth) with 20s of passive recovery between sprints. Players started 0.5m ahead of a photocell system (Brower-Timing-System, Utah) sprinted 20m, touched a cone with one hand and sprinted back through the timing system as fast as possible. Best time in a single trial, mean time and performance loss which can be calculated in various ways (Glaister et al. 2008) was established. In present investigation the performance loss was determined once according to Rampinini et al. (2007) (i.e., %decrement = ([RSAmean]/[RSAbest]×100)–100) and once by calculating the slope of the speed loss over the course of the sprints by linear regression analysis (termed fatigue slope). The reliability of the RSA test outcomes have been reported to be 1.3, 0.8, and 25.0% (typical error expressed as a coefficient of variation) for the best sprint time, the mean time and %decrement respectively (Rampinini et al. 2007). Additionally in present investigation an ICC of r = 0.894 for the mean time was observed. The YYIR test level 2 consisted of repeated 2 x 20m runs back and forth between the starting, turning, and finishing line at a progressively increased speed until exhaustion. The speed was controlled by audio bleeps. Between each shuttle, the players had a 5s active rest period, consisting of 2 x 2.5m jogging. The end of the test was considered when players failed twice to reach the front line in time (objective evaluation) or players felt unable to complete another shuttle (subjective evaluation) (Wahl et al., 2014, Krustrup et al., 2006). The completed shuttle and the resulting distance covered were registered. Approximately 3-5 min after the test capillary blood was taken from the earlobe to determine lactate concentration (Biosen C-Line, Germany).
Training program
Each training session was performed according to the protocol previously used by Faiss et al. (2013a) and took place after completing 1 hour of field team training. The training comprised 3 series of 5 x 10s back and forth sprints performed at a maximal intensity. Recovery time between repetitions was 20s and between series 5min (Faiss et al., 2013a). Sprinting distance was 4.5m and was signed by cones. Players had to touch the cone (30.5 cm in height) with their hands before turning and sprinting to the other cone. The training was arranged in the way that 2 players run simultaneously. During the 20s recovery period other 2 players performed the shuttle run. Between series (5 minutes rest) the remaining players performed the shuttles in the same way (at most 6 players performed the training simultaneously, after this training the FiCO2 raised to 0.36%). After the first and last training session (approximately 2-5 minutes after the last shuttle sprint) capillary blood was drawn from the earlobe to determine lactate concentration.
Statistical analysis
Unpaired t-test were used to examine differences between groups at training begin. ANOVA with repeated measurement design was used to determine changes due to the training intervention (main effect: training) and to determine different changes between the hypoxia and normoxia training group (interaction: training x group). Effect size (ES, partial η2) was calculated for all performance parameters. Within-group effects were analyzed by paired t-test. Results are presented as means±SD. Significance was set at p ≤ 0.05.
Results
Players of the RSH group performed 7.2 ± 1.1 and those of the RSN group 7.8±0.4 training sessions (p = 0.306). Training intensity, indicated by the number of shuttles completed, did not differ between groups (7.8 ± 0.1 vs. 7.7 ± 0.2, p = 0.228 mean shuttles performed during the training sessions). Lactate concentrations measured after the first training session did not differ between groups (8.7 ± 0.8 vs. 9.4 ± 2.2 mmol·L-1, for the RSH and the RSN group, respectively; p = 0.562) and did not change after the training period (7.7 ± 1.9 vs. 9.6 ± 2.6 mmol·L-1, for the RSH and RSN group, respectively; main effect: training p = 0.685, interaction: training x group p = 0.475). Outcomes of the performance testing are shown in Table 1. Performance of the YYIR test improved after the training (p = 0.045) and lactate concentration decreased after the YYIR test (p = 0.002), without between group differences. After RSH the fatigue slope was lower when compared to RSN (p = 0.024; Figure 1).
Table 1.
YYIR and RSA performance parameters before and after the training period.
| Hypoxia group | Normoxia group | all | ANOVA (main effect) | ANOVA (interaction) | ||||
|---|---|---|---|---|---|---|---|---|
| pre | post | pre | post | pre | post | training | training x group | |
| YYIR test | ||||||||
| Running distance (m) | 1430±458 | 1710±183 | 1832±310 | 2216±395 | 1653±414 | 1991±402 | .045 | .715 |
| (n = 4) | (n = 4) | (n = 5) | (n = 5) | (ES .46) | (ES .02) | |||
| Lactatemax (mmol·L-1) | 9.2±3.2 | 6.6±1.5 | 11.5±1.7 | 7.6±1.0 | 10.4±2.7 | 7.1±1.3 | .002 | .113 |
| (n = 4) | (n = 4) | (n = 5) | (n = 5) | (ES .75) | (ES .14) | |||
| RSA test | ||||||||
| Fastest sprint (s) | 7.1±.3 | 7.1±.3 | 7.2±.3 | 7.2±.1 | 7.1±.3 | 7.1±.2 | .852 | .876 |
| (n = 5) | (n = 5) | (n = 5) | (n = 5) | (ES 0.01) | (ES .01) | |||
| Sum of sprints (s) | 44.6±1.6 | 44.0±1.3 | 45.4±1.6 | 45.4±1.0 | 45.0±1.6 | 44.7±1.3 | .279 | .347 |
| (n = 5) | (n = 5) | (n = 5) | (n = 5) | (ES 0.14) | (ES .11) | |||
| Mean time (s) | 7.4±.3 | 7.3±.2 | 7.6±.3 | 7.6±.2 | 7.5±0.3 | 7.4±.2 | .279 | .347 |
| (n = 5) | (n = 5) | (n = 5) | (n = 5) | (ES 0.14) | (ES .11) | |||
| Performance decrement1 (%) | 5.2±1.4 | 3.7±2.0 | 5.1±1.5 | 4.6±1.5 | 5.1±1.4 | 4.2±1.7 | .212 | .498 |
| (n = 5) | (n = 5) | (n = 5) | (n = 5) | (ES .19) | (ES .06) | |||
| Fatigue slope2 (slope) | .13±.02 | .08±.04 | .11±.02 | .12±.03 | .12±.02 | .10±.04 | .077 | .024 |
| (n = 5) | (n = 5) | (n = 5) | (n = 5) | (ES .34) | (ES .49) | |||
YYIR, Yo-Yo intermittent recovery; RSA, repeated-sprint ability, Effect size, ES (partial η2)
1 calculated according to Rampinini et al. (2007): %decrement = ([RSAmean]/[RSAbest] × 100) – 100
2 slope of the linear regression equation calculated over the 6 repetitions
Figure 1.
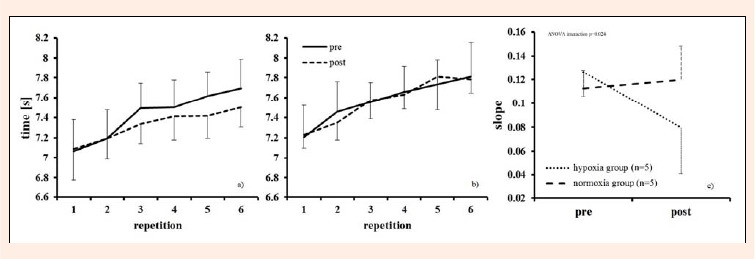
Sprinting time of each repetition during the repeated sprint ability test for the RSH (a) and the RSN (b) group and fatigue slope (c) (i.e. slope of the linear regression equation calculated over the 6 repetitions) before and after the training period.RSH, repeated sprint training in hypoxia; RSN, repeated sprint training in normoxia (Millet et al., 2013)
Discussion
To our best knowledge, this is the first study performing soccer specific shuttle-run sprint training under hypoxia conditions. Outcomes show that absolute training intensity (number of shuttles completed) does not differ between the two conditions which indicates that such type of training is feasible and can be well performed in relatively small hypoxic chambers (4.75 x 2.25m). Results also indicate that shuttle-run sprint training in hypoxia may improve RSA, with respect to the fatigue slope, when compared to training in normoxia.
Recently RSH has evolved as a promising training method. Whereas Galvin et al. (2013) did not find improvements in RSA, Faiss et al. (2013a) showed larger improvements in RSA (i.e., increased number of sprints until exhaustion) after performing repeated sprint cycling training in hypoxia compared to normoxia. Furthermore, Puype et al. (2013) showed greater improvements in the anaerobic threshold after sprint interval cycling training performed in hypoxia than normoxia. Also in the present study where, in contrast to the former studies, a presumably more common soccer training practice was applied, RSH compared to RSN resulted in a lower fatigue slope which indicates better running speed maintenance during the RSA test (Figure 1).
The mechanisms responsible for the improved RSA could be an increased muscular perfusion, a changed pH regulation and enhancement of the glycolytic activity after RSH (Faiss et al., 2013a; 2013b, Puype et al., 2013). On the contrary the muscular oxidative activity might be less influenced by such training (Faiss et al., 2013a) which could explain why no hypoxia effect on the YYIR outcome was found. However, it has to be mentioned that Galvin et al. (2013), after RSH, reported improved YYIR test outcomes when compared to RSN. The different training modalities might partly explain these different findings.
Some limitations have to be mentioned. The small sample-size certainly is the major weakness of the study. Even more surprising is the result of an improved RSA, which indicates that such training might be very promising. The missing physiological parameters explaining the hypoxia effect can be considered a further limitation. However, from a coach’s point of view performance improvements may be considered the most important outcomes even though they not always were found to have practical relevance (Mendez-Villanueva and Buchheit, 2013). It has to be clearly stated that the practicability of the proposed training regime in small hypoxic chambers should be considered the main outcome of the present study. Due to the aforementioned limitations the improved RSA outcome has to be considered with caution and should be confirmed in further studies. Moreover also the effectiveness of the proposed shuttle-run sprint training to improve match performance should be addressed in further studies as this should be the ultimately target.
Conclusion
In conclusion this study showed that soccer specific shuttle-run sprint training is feasible in hypoxic chambers of limited size. Furthermore, in youth soccer player, this type of hypoxia training might lead to larger improvements in RSA, indicated by the lower fatigue slope when compared to normoxia training. Such outcomes could not only be of importance for soccer players, but also for all athletes performing in sports with an intermittent activity profile (e.g., tennis, basketball).
Acknowledgements
The authors gratefully acknowledge the assistance of the coach (Stefan Landauer) and the head (Mag. Helmut Lorenz) of the BNZ Tyrol and of Martin Krautschneider during the testing and training sessions, as well as the participating players for their enthusiasm and cooperation. Furthermore, we want to thank Mag. Patrick Murnig from JumpAndReach for his support. The study was supported by the “Aktion D. Swarovski & Co 2012” and by the “Nachwuchsförderung 2013” of the University Innsbruck
Biographies
Hannes GATTERER
Employment
Department of Sport Science, University Innsbruck, Austria
Degree
PhD
Research interests
High altitude physiology, altitude training, intermittent hypoxia, exercise physiology, body composition
E-mail: Hannes.gatterer@uibk.ac.at
Marc PHILIPPE
Employment
Department of Sport Science, University Innsbruck, Austria
Degree
MSc
Research interests
Eccentric versus concentric exercise, high altitude physiology, exercise physiology
E-mail: Marc.Philippe@student.uibk.ac.at
Verena MENZ
Employment
Department of Sport Science, University Innsbruck, Austria
Degree
MSc
Research interests
High intensity training, high altitude physiology, exercise physiology
E-mail: verena.menz@student.uibk.ac.at
Florian MOSBACH
Employment
MSc student, Department of Sport Science, University Innsbruck, Austria
Degree
BSc
Research interests
High altitude physiology, exercise physiology
E-mail: Florian.Mosbach@student.uibk.ac.at
Martin FAULHABER
Employment
Department of Sport Science, University Innsbruck, Austria
Degree
MD
Research interests
High altitude physiology, exercise physiology, intermittent hypoxia, epidemiology of alpine sport
E-mail: Martin.Faulhaber@uibk.ac.at
Martin BURTSCHER
Employment
Prof., Department of Sport Science, University Innsbruck, Austria
Degree
PhD
Research interests
Intermittent hypoxia, high altitude physiology, high altitude diseases, exercise physiology, sports medicine
E-mail: Martin.Burtscher@uibk.ac.at
References
- Dupont G., McCall A., Prieur F., Millet G.P., Berthoin S. (2010) Faster oxygen uptake kinetics during recovery is related to better repeated sprinting ability. European Journal of Applied Physiology 110, 627-634. [DOI] [PubMed] [Google Scholar]
- Faiss R., Léger B., Vesin J.M., Fournier P.E., Eggel Y., Dériaz O., Millet G.P. (2013a) Significant molecular and systemic adaptations after repeated sprint training in hypoxia. PLoS One 8, e56522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faiss R., Girard O., Millet G.P. (2013b) Advancing hypoxic training in team sports: from intermittent hypoxic training to repeated sprint training in hypoxia. British Journal of Sports Medicine 47(Suppl.1), i45-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galvin H.M., Cooke K., Sumners D.P., Mileva K.N., Bowtell J.L. (2013) Repeated sprint training in normobaric hypoxia. British Journal of Sports Medicine 47(Suppl1), i74-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Girard O., Amann M., Aughey R., Billaut F., Bishop D.J., Bourdon P., Buchheit M., Chapman R., D'Hooghe M., Garvican-Lewis L.A., Gore C.J., Millet G.P., Roach G.D., Sargent C., Saunders P.U., Schmidt W., Schumacher Y.O. (2013a). Position statement—altitude training for improving team-sport players' performance: current knowledge and unresolved issues. British Journal of Sports Medicine 47(Suppl1), i8-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Girard O., Brocherie F., Millet G.P. (2013b) On the use of mobile inflatable hypoxic marquees for sport-specific altitude training in team sports. British Journal of Sports Medicine 47(Suppl1), i121-123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Girard O., Mendez-Villanueva A., Bishop D. (2011) Repeated-sprint ability - part I: factors contributing to fatigue. Sports Medicine 41, 673-694. [DOI] [PubMed] [Google Scholar]
- Glaister M., Howatson G., Pattison J.R., McInnes G. (2008) The reliability and validity of fatigue measures during multiple-sprint work: an issue revisited. Journal of Strength and Conditioning Research 22, 1597-1601. [DOI] [PubMed] [Google Scholar]
- Goods P.S.R., Dawson B.T., Landers G.J., Gore C.J., Peeling P. (2014) Effect of Different Simulated Altitudes on Repeat Sprint Performance in Team Sport Athletes. International Journal of Sports Physiology and Performance, [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- Hamlin M.J., Marshall H.C., Hellemans J., Ainslie P.N., Anglem N. (2010) Effect of intermittent hypoxic training on 20 km time trial and 30 s anaerobic performance. Scandinavian Journal of Medicine and Science in Sports 20, 651-661. [DOI] [PubMed] [Google Scholar]
- Krustrup P., Mohr M., Nybo L., Jensen J.M., Nielsen J.J., Bangsbo J. (2006) The Yo-Yo IR2 test: physiological response, reliability, and application to elite soccer. Medicine and Science in Sports and Exercise 38, 1666-1673. [DOI] [PubMed] [Google Scholar]
- Mendez-Villanueva A., Buchheit M. (2013)Football-specific fitness testing: adding value or confirming the evidence? Journal of Sports Sciences 31, 1503-1508. [DOI] [PubMed] [Google Scholar]
- Millet G.P., Faiss R., Brocherie F., Girard O. (2013). Hypoxic training and team sports: a challenge to traditional methods? British Journal of Sports Medicine 47(Suppl1), i6-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puype J., VanProeyen K., Raymackers J.M., Deldicque L., Hespel P. (2013) Sprint interval training in hypoxia stimulates glycolytic enzyme activity. Medicine and Science in Sports and Exercise 45, 2166-2174. [DOI] [PubMed] [Google Scholar]
- Rampinini E., Sassi A., Morelli A., Mazzoni S., Fanchini M., Coutts A. (2009) Repeated-sprint ability in professional and amateur soccer players. Applied Physiology, Nutrition, and Metabolism 34, 1048-1054. [DOI] [PubMed] [Google Scholar]
- Rampinini E., Bishop D., Marcora S.M., Ferrari Bravo D., Sassi R., Impellizzeri F.M. (2007) Validity of simple field tests as indicators of match-related physical performance in top-level professional soccer players. International Journal of Sports Medicine 28, 228-235. [DOI] [PubMed] [Google Scholar]
- Terrados N., Jansson E., Sylven C., Kaijser L. (1990)Is hypoxia a stimulus for synthesis of oxidative enzymes and myoglobin? Journal of Applied Physiology 68, 2369-2372. [DOI] [PubMed] [Google Scholar]
- Wahl P., Güldner M., Mester J. (2014) Effects and sustainability of a 13-day high-intensity shock microcycle in soccer. Journal of Sports Science and Medicine 13, 259-265. [PMC free article] [PubMed] [Google Scholar]