

Abstract
The construct and concurrent validity of the Thera-Band Perceived Exertion Scale for Resistance Exercise with elastic bands (EB) was examined. Twenty subjects performed two separate sets of 15 repetitions of both frontal and lateral raise exercise over two sessions. The criterion variables were myoelectric activity and heart rate. One set was performed with an elastic band grip width that permitted 15 maximum repetitions in the selected exercise, and another set was performed with a grip width 50% more than the 15RM grip. Following the final repetition of each set, active muscle (AM) and overall body (O) ratings of perceived exertion (RPE) were collected from the Thera-Band® resistance exercise scale and the OMNI-Resistance Exercise Scale of perceived exertion with Thera-Band® resistance bands (OMNI-RES EB). Construct validity was established by correlating the RPE from the OMNI-RES EB with the Thera-Band RPE scale using regression analysis. The results showed significant differences (p ≤ 0.05) in myoelectric activity, heart rate, and RPE scores between the low- and high-intensity sets. The intraclass correlation coefficient for active muscles and overall RPE scale scores was 0.67 and 0.58, respectively. There was a positive linear relationship between the RPE from the OMNI-RES EB and the Thera-Band scale. Validity coefficients for the RPE AM were r2 = 0.87 and ranged from r2 = 0.76 to 0.85 for the RPE O. Therefore, the Thera-Band Perceived Exertion Scale for Resistance Exercise can be used for monitoring elastic band exercise intensity. This would allow the training dosage to be better controlled within and between sessions. Moreover, the construct and concurrent validity indicates that the OMNI-RES EB measures similar properties of exertion as the Thera-Band RPE scale during elastic resistance exercise.
Key points.
This new resistance intensity scale is an appropriate and valid tool for assessing perceived exertion during strength training with elastic bands.
This scale can be used without reducing the accuracy of the dosage prescribed during training/rehabilitation sessions and while carrying out medium and/or long-term periodization programs or therapeutic interventions.
Populations with specific physical or physiological needs could have access to an easy-to-use resource that allows them to carry out their training/rehabilitation programs with greater efficacy and without any risk to health.
Key words: RPE, myoelectric activity, heart rate, resistance exercise
Introduction
The control of exercise intensity is a key factor in ensuring the safety and efficacy of physical activity in any context, including athletic, recreational, and therapeutic settings (Robertson, 2004). Simple tools as well as scales of perceived exertion have been created to ensure control of the intensity for a wide-range of exercises performed by a variety of populations (Robertson et al., 2003; 2004; 2005a; 2005b). These scales are fundamental in that there is a functional link between the three kinds of responses that can occur during physical exercise (physiological, perceptual, and performance). Therefore, these responses can be utilized in a combined fashion using perceived exertion scales to monitor exercise intensity (Lagally et al., 2002).
To make it easier to monitor intensity during the prescription and performance of physical exercise, scales have been created for use during aerobic and strength training in a wide range of situations (Robertson et al., 2003, 2004; 2005b). These scales positively relate the rating of perceived exertion (RPE) with certain physiological variables such as blood lactic acid concentration, muscular activity, and heart rate (Lagally et al., 2002; Lepley and Hatzel, 2010; Miller et al., 2009; Rozenek et al. 1993). Such tools have been implemented and validated to control intensity while performing exercises, independently of age (Robertson et al., 2005b). This means that these RPE scales would be useful for health-fitness and clinical practitioners (Robertson, 2004).
Very few studies have used the OMNI perceived exertion scale for resistance exercise (OMNI-RES) (Robertson et al., 2003; 2005b) while carrying out physical conditioning programs with different kinds of materials for strength training (i.e., weight machines; elastic bands and tubing; aquatic devices that increase drag force) (Colado et al., 2009; 2010; 2012a; Colado and Triplett, 2008). However, there is doubt as to whether this kind of scale should be used with materials other than those for which they were validated (i.e., Olympic curl bars and plate-loaded machines) (Robertson et al., 2003).
There has only been one study to date that has carried out concurrent validation of the OMNI-RES for other kinds of materials that are not based on weight for strength training, as is the case with elastic bands (Colado et al., 2012b). Myoelectric activity and heart rate were used as criterion variables, showing that the OMNI-RES can be used for monitoring the intensity of exercise when elastic bands are used. In similar fashion to the OMNI-RES scale validated for weight devices by Robertson et al. (2003), the OMNI-RES exercise scale of perceived exertion with elastic bands (OMINI-RES EB) (see figure 1a) has both verbal and mode-specific pictorial descriptors distributed over a comparatively wide response range. However, some researchers believe that it is necessary to assess the perception of effort in different conditions and in different populations to further its usability (Tiggemann et al., 2010). Furthermore, Colado (2004) advised that certain populations can find this kind of scale difficult to use as there are many levels of verbal information and mode-specific pictorial descriptors which are based on linear physiological responses, meaning that it may be necessary to create even simpler, more specific scales that are easier to use during training regimes (Colado et al., 2008; Pincivero et al., 2003). Therefore, the validity would be required to be constructed on a healthy population first before it can be used by those populations that find using the current scales to be difficult.
Figure 1.

OMNI-Resistance Exercise Scale of perceived exertion with Thera-Band® resistance bands (a) compared to Thera-Band resistance exercise scale of perceived exertion with Thera-Band® resistance bands (b).
It is well known that in order to measure the construct validity of a new scale for perceived exertion, it is necessary to correlate the RPE from a criterion scale with the RPE from a conditional scale (Robertson et al., 2004). As the OMNI-Resistance Exercise Scale of perceived exertion with Thera-Band® resistance bands used by Colado et al. (2012b) is the only specific scale to have been accepted as a valid perceptual measurement tool due to the statistically significant correlation between physiological and perceptual variables, it seems that this can be used as the criterion metric in order to establish construct validity of a new scale. To establish concurrent validity of a new scale, criterion or stimulus variables must be correlated with a concurrent or response variable (Lagally and Robertson, 2006). In addition, any validation of a new scale should provide information on its effectiveness for controlling the intensity between different training sessions. In addition it must be sensitive enough to differentially measure RPE from active muscle groups as well as the overall body where the criterion variables increased over separate sets of resistance exercise.
Therefore, the purposes of this investigation were (i) To assess the construct validity of a new perceived exertion scale for resistance exercises performed with elastic bands; (ii) To examine the effect of two different resistance exercise intensities with elastic bands on RPE, myoelectric activity, and heart rate responses; (iii) To examine the concurrent validity of the Thera-Band resistance exercise scale for use with elastic bands during isotonic resistance exercises; and (iv) To determine the reliability of the session RPE method, using the Thera-Band resistance exercise scale, for quantifying resistance training with elastic bands. It was hypothesized that (i) the two scales (OMNI-RES EB and Thera-Band® resistance exercise scale) could be used interchangeably during resistance exercises with elastic bands; and (ii) that the ratings of perceived exertion for the active muscles and overall body would show a positive link with muscular activation and heart rate during resistance exercises with elastic bands.
Methods
Experimental design
Borg’s original RPE scales have been modified during the past several decades in an attempt to apply the scales to different settings, populations, and exercises (Mays, 2009). Mays et al. (2010) stated that there are few studies that show evidence of cross-modal application of OMNI ratings of perceived exertion scales, thus providing the justification and necessity for the development of OMNI scales that differ in the pictorial, numerical and/or verbal descriptors for specific exercise modes or type of population. Considering this rationale, the Thera-Band perception of exertion scale for resistance training with elastic bands has five perception levels that range from “Easy” to “Maximal” (Figure 1b). The use of only five intensity levels could be more useful for subjects with only limited resistance training experience (Colado, 2004). Another new feature of the scale is that the values are exclusively expressed as words, which could make it more intuitive to use (Colado and Chulvi, 2008).
According to Mays et al. (2010), for a newly developed RPE scale to be considered a valid metric for use in clinical and health-fitness settings, response validity has to be established which is usually provided by concurrent and construct validity. Therefore, the present study was developed based on these guidelines. Two sets of each exercise (i.e., lateral and frontal raise) were performed at different intensities (low- and high-intensity sets), and subjects used both scales to give their ratings of perceived exertion of active muscles (RPE-AM) and overall body (RPE-O). To demonstrate the construct validity of the new Thera-Band scale, its values were compared with those obtained with the OMNI-RES EB scale while performing the two different exercises. To demonstrate the concurrent validity of the new Thera-Band scale, all dependent variables (EMG, RPE-AM, RPE-O, and heart rate) were compared for the different intensities.
Subjects
Twenty subjects [12 male and 8 female; 22.00 (±0.76) years; 1.77 (±0.03) m; 69.80 (±2.67) kg; 489.24 (±71.16) min physical activity per week; data expressed as mean (SEM)] participated in this study. The inclusion criteria were: (i) 6 months minimum experience of physical activity and (ii) attendance at weight-training class or participating in weight training exercises at least twice a week for at least 3 weeks before testing. Participants suffering musculoskeletal pain or any neuromuscular and cardiovascular disorder were excluded from the study. All subjects signed an informed consent form before starting the protocol. The review board of the institution approved the study. All procedures applied in this study comply with the requirements listed in the 1975 Declaration of Helsinki and its amendment in 2008.
Procedure
Each subject took part in a familiarization session and one measurement session at least 48 hours apart. The subjects were also advised not to carry out any exhausting activities during the 48 hours prior to each session. The study was performed in September and all the sessions were conducted at the same hour of the day. The subjects were also told not to change their diets and not to consume stimulants (e.g., caffeine) 4 hours before the sessions. The subjects were permitted to drink water ad libitum during the study sessions.
The measurement protocols were always strictly controlled by the same evaluators, using a digital metronome to ensure that the different exercises and series were always performed at the same speed. The subjects underwent a standard warm-up in every session. The order in which the exercises were performed was counterbalanced. The order in which the different sets were performed according to their intensity was randomised for the measurement sessions.
Familiarization session
In the first session, the subjects became familiar with the exercises and the use of the scales. They were instructed to use the correct technique in both exercises, avoiding any nonstandard movements and focusing movement exclusively on the shoulder. In addition, the subjects were helped to maintain the correct position (and enhance the reproducibility of the experimental situation) through appropriate configuration of the measurement area. The range of movement was set from a position at which the hand was touching the hip to 900 for both movements. The exercises were performed using the dominant upper extremity.
During this session, the grip width with which they reached their 15 repetition maximum (RM) was determined, taking into account the suggestions of previous studies (Colado et al., 2012b; Newsam et al., 2005). To do this, the subjects performed sets of each exercise, adjusting the grip width until they were able to perform 15RM. During this procedure, the recovery time between series was 3 minutes.
In order to familiarize themselves with the scales, the subjects carried out two different protocols, one of high and one of low intensity, to establish the range of values for perceived exertion and how they corresponded to the ratings on the OMNI-RES EB and Thera-Band scales. The high-intensity protocol was performed first, during which the subjects also performed an additional set of 15 repetitions with the grip width at 100% of their 15RM. At the end of the same protocol, it was explained that the perceived exertion at that time corresponded to a rating of “10” on the OMNI-RES EB scale and “Maximal” on the Thera-Band scale. During the low-intensity protocol, they performed a single repetition with a grip width that only allowed the elastic band to tighten very slightly at the end of the range of movement. At the end of this set, it was explained that the perceived exertion at that time corresponded to a rating of “0” on the OMNI-RES EB scale and “Easy” on the Thera-Band scale.
Experimental sessions
Two identical measurement sessions were carried out to obtain electromyographic (EMG) recordings, heart rate data, and RPE while the subjects performed one set of 15 low-intensity repetitions and another of high-intensity repetitions of each of the exercises. During the low-intensity set, the subjects carried out the exercises with a grip width of +50% over the width with which they achieved their 15RM and with the grip identified for the 15RM during the high intensity set. The recovery time between these sets was 2 minutes. At the end of the concentric phase of the last repetition, the subjects reported their perceived exertion of the active muscles with both scales and, immediately after finishing the set, their overall perception using both scales (i.e., a number from the OMNI-RES EB scale and a letter from the Thera-Band scale). The reliability of the scale was also tested from these two identical measurement sessions.
Electromyography recording
Surface electromyographic (SEMG) signals were measured using the Telemyo 900 system (Noraxon USA Inc., Scottsdale, AZ, USA). The skin was shaved, abraded and cleansed with alcohol before placing a disposable bipolar surface electrode (Noraxon dual electrode, Noraxon USA Inc., Scottsdale, AZ, USA) over the muscle. Surface electrodes were placed on the following muscle groups: (i) Pectoralis Major (one third of the distance between the anterior aspect of the acromion and the xiphoid process); (ii) Anterior Deltoid (between the lateral border of the clavicle and the deltoid tuberosity on the humerus); (iii) Middle Deltoid (3cm below the acromion over the muscle mass on the lateral upper arm); and (iv) Supraspinatus (aligned with the midpoint of the scapular spine, 2cm superiorly).
All signals were acquired at a sampling frequency of 1 kHz, amplified and converted from analogue to digital. All EMG records (µV) were stored on a hard drive for later analysis.
To normalize the EMG data, the subjects made an attempt with the dominant extremity to obtain their maximum isometric voluntary contraction (MIVC) for each of the exercises. These isometric attempts were performed with a 450 angle of the glenohumeral joint, following the same technical principles as in the dynamic exercises.
Heart rate measurement
Heart rate monitors (Polar FT1, Polar Electro, Tampere, Finland) were attached around the chests of the subjects with an elastic band. The reading given by the pulsometer when the subject performed the 15th repetition of each series was recorded and stored for later analysis.
Data reduction
All SEMG signal analyses were performed with Matlab 7.0 (Mathworks Inc., Natick, MA, USA). The SEMG signals related to the isometric exercises were analyzed using the middle 2s period. On the other hand, the SEMG signals of the dynamic exercises were analyzed using the entire fifteenth repetition. All signals were bandpass-filtered at a 20–400 Hz cut-off frequency with a 4th-order Butterworth filter. SEMG amplitude in the time domain was quantified using the root mean square (RMS) and processed every 100 milliseconds. The maximum and mean RMS amplitudes were selected for every trial. The data obtained were normalized to the MIVC, and therefore expressed as percentage of the MIVC.
Statistical analyses
Statistical analysis was carried out using SPSS version 17 (SPSS inc., Chicago, IL, USA). All variables were checked for normality (K-S normality test). Standard statistical methods were used to obtain the mean as a measurement of the central trend and the standard error (SE) as a measurement of dispersion.
The construct validity was determined for overall and active muscle RPE, using categorical linear regression analysis, with the RPE of the OMNI-RES EB as predictor for the RPE Thera-Band scale. In addition, a mixed model [Site (2) x Exercise (2) x Intensity (3)] MANOVA was performed to examine the RPE for the OMNI scale. Post-hoc analysis with the Bonferroni correction was performed in the case of significant main or interaction effects. The Chi Square test (χ2) was applied to examine the RPE for the Thera-Band scale. The level of significance was set at p ≤ 0.05 prior to Bonferroni correction.
Regarding the concurrent validation, a mixed model [muscle group (2) x condition (2)] MANOVA was performed to determine the effect of the intensity on the SEMG-related variables for both exercises. Post-hoc analysis with Bonferroni correction was performed in the case of significant main or interaction effects. Also, Student t-tests for related samples (two-tailed) were applied to determine the existence of differences between intensities in heart rate data. Bonferroni correction was applied to avoid increasing familywise error as several dependent variables were included in Student t-tests. Wilcoxon test was applied to determine differences between intensities in RPE scores. Finally, the reliability of the RPE scores was checked by means of intraclass correlation coefficient (ICC) and standard error of measurement (SEM). The level of significance was set at p ≤ 0.05 prior to Bonferroni correction.
Results
Regarding the construct validity, categorical line regression analysis showed that the RPE of the OMNI-RES EB scale was an excellent predictor for the RPE of the Thera-Band scale for active muscles with frontal (r2 = 0.87, SEE = 0.035) and lateral raise (r2 = 0.87, SEE = 0.018) and overall body with the frontal (r2 = 0.85, SEE = 0.022) and lateral raise (r2 = 0.76, SEE = 0.045).
The MANOVA revealed a significant main effect of the intensity on the RPE of the OMNI-RES EB scale (F4,35 = 37.62, p < 0.001, η2p = 0.81). Univariate contrast showed a main effect of the intensity on overall body RPE (F1.56,59.31 = 55.69, p < 0.001, η2p = 0.59) and active muscles RPE (F1.36,51.76 = 90.73, p < 0.001, η2p = 0.7) of the OMNI-RES EB scale (Figure 2).
Figure 2.
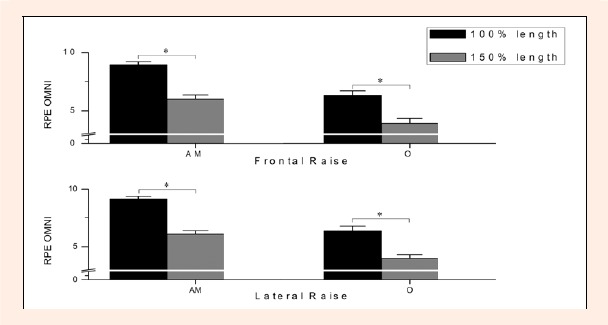
Comparisons between intensities on the OMNI-RES with elastic band scores. The columns represent the mean and the error bars represent the standard error of the mean. AM = active muscles; O = overall body. * Indicates significant differences (p<0.05) between intensities.
Finally, there was a significant association between the intensity and the RPE-AM in the frontal raise (χ28 = 29.05, p < 0.001) and the lateral raise (χ28 = 25.09, p=0.002). There was also a significant association between the intensity and the RPE-O in the frontal raise (χ28 = 16.99, p = 0.03) and the lateral raise (χ28 = 18.54, p = 0.018).
Regarding the concurrent validity, multivariate contrast revealed that there was a main effect of the intensity in the EMG-related variables in the frontal (F2,34 = 13.69, p < 0.001, η2p = 0.45) and lateral raise (F2,35 = 11.01, p < 0.001, η2p = 0.39) exercises. Univariate analysis shown a significant main effect of the intensity in the mean RMS (F1,35 = 28.07, p < 0.001, η2p = 0.44) and maximum RMS (F1,35 = 12.58, p = 0.001, η2p = 0.26) in the frontal raise exercise. This effect also appeared in the mean RMS (F1,36 = 17.64, p < 0.001, η2p = 0.33) and maximum RMS (F1,36 = 19.44, p < 0.001, η2p = 0.35) in the lateral raise exercise. The results provided by the planned contrasts are shown in Figure 3.
Figure 3.
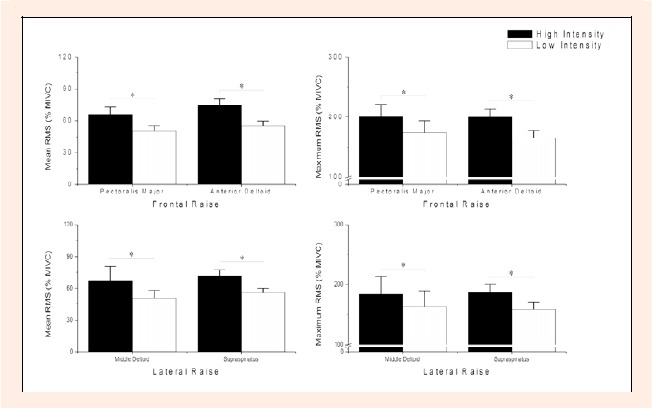
Comparisons between intensities for muscle activation. The columns represent the mean and the error bars represent the standard error of the mean. * Indicates significant differences (p<0.05) between intensities.
The RPE scores for active muscles were higher in the high intensity set than in the low intensity set (z = -3.904, p < 0.001) for the frontal raise. The same results were found for the lateral raise (z = -3.716, p < 0.001). In regards to the RPE overall scores, the results show lesser values in the low intensity test for frontal (z = -3.535, p < 0.001) and lateral (z = -3.779, p < 0.001) raises (Figure 4). Finally, the heart rate in the low intensity test (frontal raise: 112.6 ± 4.74, lateral raise: 113.05 ± 4.97) was lower than in the high intensity protocol (frontal raise: 122.45 ± 4.74, lateral raise: 124.0 ± 4.72) for both exercises, frontal (t19 = 4.43, p<0.001) and lateral (t19 = 6.16, p < 0.001) raises.
Figure 4.
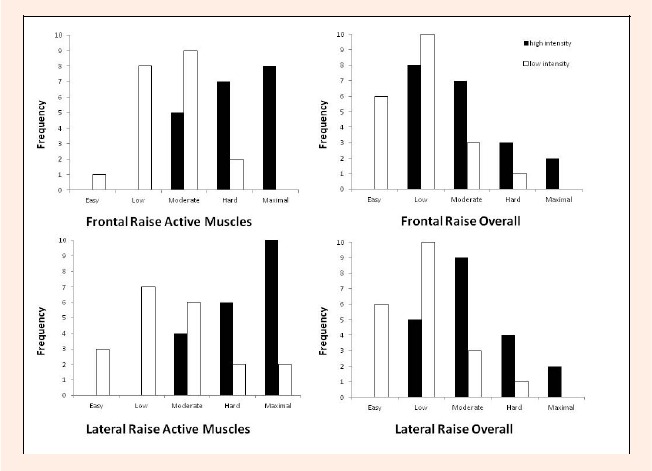
Ratings of Perceived Exertion Scores. The columns represent the frequency.
The inter-session reliability analysis shows moderate-good intraclass correlation coefficient (ICC) for active muscles (0.67; SEM = 0.62) and overall (0.58; SEM = 0.65) RPE scale scores.
Discussion
The most important finding of this study was that the Thera-Band resistance scale can be used to monitor intensity when elastic bands are used. This is of great relevance because there is still a need to find valid methods of monitoring global training intensity during resistance training (Day et al., 2004), even more so when materials such as elastic bands are used (Colado and Triplett, 2008). Thus, this study has validated a new and simplified scale that favours precise control of exercise intensity during resistance training with elastic bands.
The findings of this study are in agreement with certain previous studies that used the OMNI Scale to assess exertional perceptions during resistance exercises (Robertson et al., 2003; 2005b). Therefore, a scale with a new pictorial format has been validated using a concurrent paradigm (Robertson et al., 2005b). The results indicate that there are differences in the physiological (EMG and heart rate) and perceptual variables in response to changes in resistance exercise intensity through elastic band grip width. This reduction in grip width is normally used with elastic bands as the equivalent to increasing resistance when training with weight-based devices (Colado and Triplett, 2008). Therefore, these findings are also consistent with previous studies using Borg scales (i.e., 6–20, CR-10) that showed RPE increased as a function of increasing the total weight lifted (Pinciveiro et al., 2001; Suminski et al., 1997).
In accordance with the hypothesis, the Thera-Band resistance exercise scale and the OMNI-RES EB scale obtained validity coefficients for the RPE AM of r2 = 0.87 and ranged from r2 = 0.76 to 0.85 for the RPE O. Thus, if perceived exertion is high or low on the OMNI-RES EB scale, it must also be high or low, respectively, on the Thera-Band resistance exercise scale. As with the present study, several studies have been carried out to obtain the construct validity of different scales for different kinds of exercises, with all of them obtaining validity coefficients in similar relevance to those obtained in the present study (Lagally and Robertson, 2006; Nakamura et al., 2009; Utter et al., 2006). With these studies, the Borg 6-20 Scale was used as the criterion metric, as was the case with the construct validity of the OMNI Resistance Exercise Scale (Lagally and Robertson, 2006), OMNI-Kayak RPE Scale (Nakamura et al., 2009), and Omni Perceived Exertion Scale for Elliptical Ergometry (Mays et al., 2010). Specifically, the present study examined the construct validity of the Thera-Band resistance exercise scale using the OMNI-RES EB scale as the criterion metric.
Gearhart et al. (2002) showed that performing few maximal repetitions using a heavier weight is perceived to be more difficult than lifting a comparatively lighter weight with more repetitions. This finding was also corroborated in the current study, since a set with greater resistance (shorter grip width) with the associated maximum number of repetitions led the subjects to report a higher perception of exertion than that obtained when performing a set with less resistance (longer grip width) and with the same number of repetitions not associated with a maximum effort.
We have, therefore, objectively confirmed the validity of the method for prescribing intensity while performing strength exercises with materials where the resistance may not be constant, as is the case with elastic bands. This methodology follows the suggestions of previous studies (Kraemer et al., 2001; Suminski et al., 1997) where the number of repetitions was adapted to the training aims and where perceived exertion was used as a criteria to create a progressive or more exact prescription of the exercise intensity, having been applied successfully with different populations in previous studies for the development of programs with elastic bands and tubes (Colado et al., 2009; 2010; Colado and Triplett, 2008).
The construct and concurrent validation of our study has been performed only with the evaluation of two exercises following the same methodological guidelines regarding the number of exercises employed and characteristics of previous studies (Colado et al., 2012b; Lagally et al., 2002; Pincivero et al., 2003; Robertson et al., 2003; 2005b). An advantage of the present study was the use of two exercises of the upper extremities versus one because previous studies that examined ratings of perceived exertion during resistance exercise usually have employed one exercise for upper or lower body (Lagally et al., 2002; Pincivero et al., 2003; Robertson et al., 2003; 2005b). In our study, both exercises produced similar scores.
In accordance with other findings (Miller et al., 2009; Colado et al., 2012b), a reduction in elastic band grip width was related to an increased heart rate and local and overall perception of the exertion associated with the exercise being performed. Therefore, these results could indicate that this tool could be useful for monitoring heart rate in populations with cardiovascular disorders (ACSM, 2004; Williams et al., 2007).
In addition, one of the purposes of this investigation was to determine the reliability of the session RPE method, using the Thera-Band resistance exercise scale, for quantifying resistance training with elastic bands. The inter-session reliability analysis shows moderate-good ICC for active muscles and overall RPE scale scores. Therefore, the session RPE method of quantifying resistance training using the Thera-Band resistance exercise scale was shown to be a reliable measurement tool across two different elastic band training sessions when the same training intensity was applied, as was also shown by Buckley et al. (2000), Day et al. (2004), Buckley et al. (2009) and Marin et al. (2012) who tested the reliability of the RPE in different types of exercises and conditions.
Finally, it should be noted that this study is limited by the fact that it has been carried out on a healthy population with exercises only for the upper limbs. Therefore, we recommend that any future studies should confirm these findings with other populations and also include exercises for the lower limbs, and with even more technically complex exercises (i.e., multi-joint exercises).
Conclusion
The results obtained could be very valuable for researchers, clinicians, and coaches when designing and monitoring resistance-training programs with elastic bands, as these results suggest that the two scales can be used interchangeably during resistance exercise. Thus, they are appropriate and valid tools for assessing perceived exertion during this type of exercise. However, it is suggested that a single scale be selected and used consistently throughout the training program or individual workout (Lagally and Robertson, 2006). The good construct validity coefficients obtained in the present study show that the Thera-Band resistance exercise scale can be used without reducing the accuracy of the dosage prescribed during training/rehabilitation sessions and while carrying out medium and/or long-term periodization programs or therapeutic interventions. The new scale has a simpler construct (visual and verbal) than previous ones, meaning that it could be easier to apply in very different populations and allow us to overcome the limitations that arise in certain cases when perception of effort is used to monitor intensity during resistance training (Glass and Stanton, 2004). However, as has been indicated previously, future studies are needed to apply this new scale on new populations that are different from the subjects employed in our study.
The findings of this study may have important implications for exercise prescription, as this new scale showing the use of the Thera-Band resistance exercise scale with elastic bands can be a useful tool that allows the stimulus regime to be applied more effectively when performing strength training with inexpensive and accessible devices such as elastic bands. In this respect, those populations with specific physical or physiological needs, where elastic bands are accessible devices that match their special characteristics, could have access to an easy-to-use resource that allows them to carry out their training/rehabilitation programs with greater efficacy and without any risk to health (Andersen et al., 2010; Colado et al., 2009; Ellenbecker and Cools, 2010).
Acknowledgements
X.G.M. was a Vali+D researcher in formation, and thanks the Generalitat Valenciana.
Biographies
Juan C. COLADO
Employment
Tenured Professor, Department of Physical Education and Sport, University of Valencia, Spain.
Degree
PhD
Research interests
Strength and conditioning, measurement and evaluation.
E-mail: juan.colado@uv.es
Xavier GARCIA-MASSO
Employment
Assistance teacher, Faculty of Teaching Education, University of Valencia, Spain.
Degree
PhD
Research interests
Strength and conditioning, measurement and evaluation.
E-mail: Xavier.Garcia@uv.es

N. Travis TRIPLETT
Employment
Professor and Interim Department Chair, Department of Health, Leisure, and Exercise Science, Appalachian State University, USA.
Degree
PhD
Research interests
Strength and balance training.
E-mail: triplttnt@appstate.edu

Joaquin CALATAYUD
Employment
Research Fellow, Department of Physical Education and Sport, University of Valencia, Spain.
Degree
PhD student
Research interests
Strength and conditioning, measurement and evaluation.
E-mail: ximo86@hotmail.com

Jorge FLANDEZ
Employment
Tenured Professor, Faculty of Pedagogy in Physical Education, Sports and Recreation, Austral University of Valdivia, Chile.
Degree
PhD
Research interests
Strength and conditioning, measurement and evaluation.
E-mail: jflandezv@gmail.com
David G. BEHM
Employment
Associate Dean; School of Human Kinetics and Recreation, Memorial University of Newfoundland, St. John’s Newfoundland, Canada
Degree
PhD
Research interests
Neuromuscular responses to exercise
E-mail: dbehm@mun.ca

Michael E. ROGERS
Employment
Professor and Chair, Department of Human Performance Studies, Wichita State University, Wichita, Kansas, USA.
Degree
PhD
Research interests
Strength and balance training.
E-mail: michael.rogers@wichita.edu
References
- American College of Sports Medicine (ACSM). (2004) Exercise and hypertension. Medicine and Science in Sports and Exercise 36, 533-553. [DOI] [PubMed] [Google Scholar]
- Andersen L.L., Andersen C.H., Mortensen O.S., Poulsen O.M., Bjørnlund I.B., Zebis M.K. (2010) Muscle activation and perceived loading during rehabilitation exercises: comparison of dumbbells and elastic resistance. Physical Therapy 90, 538-549. [DOI] [PubMed] [Google Scholar]
- Buckley J.P., Eston R.G., Sim J. (2000) Ratings of perceived exertion in braille: validity and reliability in production mode. British Journal of Sports Medicine 34, 297-302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckley J.P., Sim J., Eston R.G. (2009) Reproducibility of ratings of perceived exertion soon after myocardial infarction: responses in the stress-testing clinic and the rehabilitation gymnasium. Ergonomics 52, 421-427. [DOI] [PubMed] [Google Scholar]
- Colado J.C. (2004) Physical conditioning in the aquatic medium. Paidotribo, Barcelona (Spain). [Google Scholar]
- Colado J.C., Chulvi I. (2008) Criteria for development of general neuromuscular conditioning programs within the health area. Muscle Conditioning in Weight Training Facilities: Scientific-Medical Bases For Healthly Physical Exercise. Rodriguez P.L.Madrid: Panamericana Publishing; 91-127. [Google Scholar]
- Colado J.C., Chulvi I., Heredia J.R. (2008) Criteria for the design of programs for muscle conditioning from a functional perspective. Muscle Conditioning in Weight Training Facilities: Scientific-Medical Bases For Healthly Physical Exercise. Rodriguez P.L.Madrid: Panamericana Publishing; 154-167. [Google Scholar]
- Colado J.C., Garcia-Masso X., Pellicer M., Alakhdar Y., Benavent J., Cabeza-Ruiz R.A. (2010) Comparison of elastic tubing and isotonic resistance exercises. International Journal of Sports Medicine 31, 810-817. [DOI] [PubMed] [Google Scholar]
- Colado J.C., Garcia-Masso X., Rogers M.E., Tella V., Benavent J., Dantas E. H.M. (2012a) Effects of aquatic and dry land resistance training devices on body composition and physical capacity in postmenopausal women. Journal of Human Kinetics 32, 185-195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colado J.C., Garcia-Masso X., Triplett N.T., Flandez J., Borreani S., Tella V. (2012b) Concurrent validation of the OMNI-Resistance exercise scale of perceived exertion with Thera-Band® resistance bands. Journal of Strength and Conditioning Research 26, 3018-3024. [DOI] [PubMed] [Google Scholar]
- Colado J.C., Triplett N.T. (2008) Effects of a short-term resistance program using elastic bands versus weight machines for sedentary middle-aged women. Journal of Strength and Conditioning Research 22, 1441-1448. [DOI] [PubMed] [Google Scholar]
- Colado J.C., Triplett N.T., Tella V., Saucedo P., Abellán J. (2009) Effects of aquatic resistance training on health and fitness in postmenopausal women. European Journal of Applied Physiology 106, 113-122. [DOI] [PubMed] [Google Scholar]
- Day M.L., McGuigan M.R., Brice G., Foster C. (2004) Monitoring exercise intensity during resistance training using the session RPE scale. Journal of Strength and Conditioning Research 18, 353-358. [DOI] [PubMed] [Google Scholar]
- Ellenbecker T.S., Cools A. (2010) Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: an evidence-based review. British Journal of Sports Medicine 44, 319-327. [DOI] [PubMed] [Google Scholar]
- Gearhart R.F., Jr., Goss F.L., Lagally K.M., Jakicic J.M., Gallagher J., Gallagher K.I., Robertson R.J. (2002) Ratings of perceived exertion in active muscle during high-intensity and low-intensity resistance exercise. Journal of Strength and Conditioning Research 16, 87-91. [PubMed] [Google Scholar]
- Glass S.C., Stanton D.R. (2004) Self-selected resistance training intensity in novice weightlifters. Journal of Strength and Conditioning Research 18, 324-327. [DOI] [PubMed] [Google Scholar]
- Kraemer W.J., Keuning M., Ratamess N.A., Volek J.S., McCormick M., Bush J.A., Nindl B.C., Gordon S.E., Mazzetti S.A., Newton R.U., Gomez A.L., Wickham R.B., Rubin M.R., Hakkinen K. (2001) Resistance training combined with bench-step aerobics enhances women’s health profile. Medicine and Science in Sports and Exercise 33, 259-269. [DOI] [PubMed] [Google Scholar]
- Lagally K.M., Robertson R.J., Gallagher K.I., Goss F.L., Jakicic J.M., Lephart S., Goodpaster B. (2002) Perceived exertion, electromyography, and blood lactate during acute bouts of resistance exercise. Medicine and Science in Sports and Exercise 34, 552-559. [DOI] [PubMed] [Google Scholar]
- Lagally K.M., Robertson R.J. (2006) Construct validity of the OMNI Resistance Exercise Scale. Journal of Strength and Conditioning Research 20, 252-256. [DOI] [PubMed] [Google Scholar]
- Lepley A.S., Hatzel B.M. (2010) Effects of weightlifting and breathing technique on blood pressure and heart rate. Journal of Strength and Conditioning Research 24, 2179-2183. [DOI] [PubMed] [Google Scholar]
- Marín P.J., Santos-Lozano A., Santin-Medeiros F., Robertson R.J., Garatachea N. (2012) Reliability and validity of the OMNI-vibration exercise scale of perceived exertion. Journal of Sports Science and Medicine 11, 438-443. [PMC free article] [PubMed] [Google Scholar]
- Mays R.J. (2009) Validation of adult OMNI perceived exertion scales for elliptical ergometry (Dissertation). Faculty of School of Education, University of Pittsburgh (USA). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mays R.J., Goss F.L., Schafer M., Kim K.H., Nagle-Stilley E.F., Robertson R.J. (2010) Validation of adult Omni perceived exertion scales for elliptical ergometry. Perceptual & Motor Skills 111, 848-862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller P.C., Hall E.E., Chmelo E.A., Morrison J.M., DeWitt R.E., Kostura C.M. (2009) The influence of muscle action on heart rate, RPE, and affective responses after upper-body resistance exercise. Journal of Strength and Conditioning Research 23, 366-372. [DOI] [PubMed] [Google Scholar]
- Nakamura F.Y., Perandini L.A., Okuno N.M., Borges T.O., Bertuzzi R.C., Robertson R.J. (2009) Construct and concurrent validation of OMNI-Kayak rating of Perceived Exertion Scale. Perceptual & Motor Skills 108, 744-758. [DOI] [PubMed] [Google Scholar]
- Newsam C.J., Leese C., Fernandez-Silva J. (2005) Intratester reliability for determining an eight-repetition maximum for three shoulder exercises using elastic bands. Journal of Sport Rehabilitation 14, 35-47. [Google Scholar]
- Pincivero D.M., Coelho A.J., Campy R.M., Salfetnikov Y., Bright A. (2001) The effects of voluntary contraction intensity and gender on perceived exertion during isokinetic quadriceps exercise. European Journal of Applied Physiology 84, 221-226. [DOI] [PubMed] [Google Scholar]
- Pincivero D.M., Coelho A.J., Campy R.M. (2003) Perceived exertion and maximal quadriceps femoris muscle strength during dynamic knee extension exercise in young adult males and females. European Journal of Applied Physiology 89, 150-156. [DOI] [PubMed] [Google Scholar]
- Robertson R.J. (2004) Perceived Exertion for Practitioners. Human Kinetics, Champaign, IL. [Google Scholar]
- Robertson R.J., Goss F.L., Rutkowski J., Lenz B., Dixon C., Timmer J., Frazee K., Dube J., Andreacci J. (2003) Concurrent validation of the OMNI perceived exertion scale for resistance exercise. Medicine and Science in Sports and Exercise 35, 333-341. [DOI] [PubMed] [Google Scholar]
- Robertson R.J., Goss F.L., Dubé J., Rutkowski J., Dupain M., Brennan C., Andreacci J. (2004) Validation of the adult OMNI scale of perceived exertion for cycle ergometer exercise. Medicine and Science in Sports and Exercise 36, 102-108. [DOI] [PubMed] [Google Scholar]
- Robertson R.J., Goss F.L., Andreacci J., Dubé J., Rutkowski J., Snee B., Kowallis R., Crawford K., Aaron D., Metz K. (2005a) Validation of the children’s OMNI RPE scale for sStepping exercise. Medicine and Science in Sports and Exercise 37, 290-298. [DOI] [PubMed] [Google Scholar]
- Robertson R.J., Goss F.L., Andreacci J., Dubé J., Rutkowski J., Frazee K.M., Aaron D.J., Metz K. F., Kowallis R.A., Snees B.M. (2005b) Validation of the children’s OMNI resistance exercise scale of perceived exertion. Medicine and Science in Sports and Exercise 37, 819-826. [DOI] [PubMed] [Google Scholar]
- Rozenek R., Rosenau L., Rosenau P., Stone M.H. (1993) The effect of intensity on heart rate and blood lactate response to resistance exercise. Journal of Strength and Conditioning Research 7, 51-54. [Google Scholar]
- Suminski R.R., Robertson R.J., Arslanian S., Kang J., Utter A.C., DaSilva S.G., Goss F.L., Metz K.F. (1997) Perception of effort during resistance exercise. Journal of Strength and Conditioning Research 11, 261-265. [Google Scholar]
- Tiggemann C.L., Korzenowski A.L., Brentano M.A., Tartaruga M.P., Alberton C.L., Kruel L.F.M. (2010) Perceived exertion in different strength exercise loads in sedentary, active, and trained adults. Journal of Strength and Conditioning Research 24, 2032-2041. [DOI] [PubMed] [Google Scholar]
- Utter A.C., Kang J., Nieman D.C., Dumke C.L., McAnulty S.R. (2006) Validation of Omni scale of perceived exertion during prolonged cycling. Medicine and Science in Sports and Exercise 38, 780-786. [DOI] [PubMed] [Google Scholar]
- Williams M.A., Haskell W.L., Ades P.A., Amsterdam E.A., Bittner V., Franklin B.A., Gulanick M., Laing S.T., Stewart K.J.; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Nutrition, Physical Activity, and Metabolism. (2007) Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 31, 572-584. [DOI] [PubMed] [Google Scholar]