

Abstract
Background:
It has been established that hyperlipidemia increases the incidence and mortality associated with coronary heart disease. In this study, the effects of Dill (Anethum graveolens) were evaluated on lipid profile of hypercholesterolemic patients.
Materials and Methods:
In this clinical study, 91 hyperlipidemic patients were randomly designated into two groups. One group received gemfibrozil (900 mg daily) and the other group received Dill tablet (six tablets daily) for 2 months. The blood lipids including total cholesterol, triglyceride and high density lipoprotein (HDL)-cholesterol from each group were assessed at the beginning and end of the trial.
Results:
Use of gemfibrozil brought about increased HDL-cholesterol by 3.91% (P < 0.05) and reduced triglyceride and total cholesterol by 32.7% (P < 0.05) and 9.41% (P < 0.05), respectively. Applying Dill tablet for 2 months resulted in reduction of total cholesterol up to 18% (P < 0.05) and triglyceride by 7.38% (P < 0.05). However, circulating HDL-cholesterol was not affected by this treatment. In this study, gemfibrozil decreased triglyceride and increased HDL-cholesterol more than anethum (P < 0.05). Anethum decreased total cholesterol more than gemfibrozil (P < 0.05). Patients treated with anethum did not report any side effects.
Conclusion:
The results of this trial indicate that Dill might be beneficial for hypercholesterolemic and hypertriglycemic patients.
Keywords: Anethum graveolens, gemfibrozil, high density lipoprotein-cholesterol, total cholesterol, triglyceride
INTRODUCTION
Cardiovascular diseases are the leading causes of morbidity and mortality all over the world. Hypercholesterolemia, especially elevated low-density lipoprotein (LDL), is a major coronary heart disease risk factor. While the American Heart Association <200 mg/dl recommended for cholesterol,[1] 16% of adults were found to have more than 240 mg/dl, a level considered to carry twice the cardiovascular risk of those individuals at the desired level.[1] Elevated LDL cholesterol and triglycerides are considered detrimental of cardiovascular outcomes. It has been suggested that very LDL and chylomicron remnants might also play an active role in peripheral vascular and coronary artery disease development.[2] Therefore, considerable attention has been directed toward examining the impact of cholesterol lowering medications and interventions for cardiovascular outcomes.[2]
Cholesterol has been shown to interrupt and alter vascular function and structure as it builds within the lining of the vascular wall, and is able to interfere with endothelial function leading to plaques, lesions, occlusion, and emboli; along with a reduction in recovery, healing, and appropriate management of ischemia/reperfusion injury.[3] With specific relevance to the microcirculation, it has been clearly demonstrated that evolution of hypercholesterolemia is associated with endothelial cell dysfunction.[3] In addition, it has been shown that there is a near abrogation in vascular nitric oxide bioavailability, elevated oxidant stress, and the creation of a strongly proinflammatory condition; symptoms which can culminate in profound impairments to vascular reactivity.[4] Researches in vascular consequences of chronic hypercholesterolemia, the mechanisms through which these consequences occur, and the potentially beneficial effects of ameliorative therapies have received considerable attention in recent years.[5,6,7]
In this regard, tending to use herbal medicine not only in the treatment and preventing various diseases,[8,9,10] but also in preventing the toxic effects of other drugs[11,12,13] has dramatically increased, especially in Iran. Fortunately, recent researches in the field of medicinal plants have had promising results,[2,14,15,16,17,18,19] although they may have significant side effects, too.[20,21,22,23,24] Dill (Anethum graveolens) is one of these plants which is also known as shevid and is sometimes used with rice and called shevid-polo.[25,26] It is the sole species of the genus Anethum. Dill usually grows to 40-60 cm, with slender stems, finely divided, softly delicate leaves. The flowers are white to yellow, in small umbels 2-9 cm diameter.[26] Dill has a very long history of herbal use going back more than 2000 years. The seeds are a common and very effective household remedy for a wide range of digestive problems. The dill is useful as aromatic, carminative, mildly diuretic, galactogogue, stimulant and stomachic. It is also used to increase the flow of milk in nursing mothers, to help prevent colic, for bad breath, cough, cold and flu, period pains.[27,28,29]
Many people in Iran believe it can alleviate hyperlipidemia. According to an animal study, it has been shown to reduce postprandial heperglycemia and hypercholesterolemia in rabbit.[30] However, its impact on these parameters in human has not been studied, yet. This study was, therefore, designed to evaluate the Dill effects in comparison to gemfibrozil on lipid profile of hypercholesterolemic patients.
MATERIALS AND METHODS
This randomized single blind clinical study was performed on referring individuals to internal clinic, in Shahrekord University of Medical Sciences. The blood test was taken from patients after taking written consent and completing questionnaire by the colleague physician. Subjects in both groups using gemfibrozil and Dill were asked about age, gender, job (housekeeper, unemployed, and practitioner), the degree (illiterate, elementary education, diploma, bachelor or higher), body mass index (BMI), and related risk factors such as risk of hypertension and diabetes, smoking, having heart disease, heart disease history or hyperlipidemia in family (to take blood test, participants were asked to keep themselves fasting between 10 h and 14 h (6 pm-8 am). During this time, they were free to drink water or tea. Then they referred to reference laboratory to take test in the morning. Total cholesterol and high density lipoprotein (HDL) were measured with cholesterol oxidase-phosphatidic acid phosphatase (PAP) enzyme approach and triglycerides with glycerol phosphate oxidase-PAP enzyme approach, and spectrophotometric in 520 nm wavelength, according to kit instructions. Because in cases that triglyceride is more than 400 mg/dl, Friedewald formula cannot be used to measure LDL[27] and with regarding to this problem that in this study, great numbers of patients had triglyceride more than 400 mg/dl, it was skipped to measure and investigate LDL. After doing primary test, patients who had serum triglyceride between 250 and 400 mg/dl, and serum total cholesterol between 220 and 27 mg/dl and had not used drugs during the past month were invited to participate.
The hyperlipidemic patients with normal fasting glucose levels, normal kidney, liver and thyroid functions included the trial. Patients with coronary artery disease, diabetes, hypertension, or obesity were excluded from the study. No patient was allowed to use lipid-modifying drugs, diuretics, beta-blockers, corticosteroids, and sex steroids.
Ninety ones who met the above requirements, willing to cooperate were placed equally in groups A and B based on the entrance time, so that, the first patient was assigned to group one and the second one to group two, and so on. Group A was given gemfibrozil (Darupakhsh, Iran), 900 mg orally/day,[31] and group B was given Dill tablets (six pills a day, Iran Daruk, Iran) for 2 months. The Dill dose was chosen based on traditional use of this plant by Iranian people. Patients were asked to record and report any side effects. Blood lipid testing was repeated again at the end of the treatment period. After completing questionnaires and laboratory results, data were compared by paired t-test using, IBM SPSS Statistics version 21, USA.
Data were analyzed by paired t-test for comparison of each factor before and after treatment and Student's t-test for comparison of the each factor between groups, using SPSS software version.
RESULTS
A total of 13 patients were excluded from the study due to incompliance, so that 42 patients in gemfibrozil group and 35 ones in Dill group completed the study. These patients were taken a test at the end of the study [Figure 1]. People in both treatment groups of gemfibrozil and Dill were compared according to age, gender, BMI, smoking, having diabetes, hypertension and heart disease that there was no significant difference between them. Furthermore, there was no significant difference between two groups for cholesterol, triglyceride or HDL before treatment [Table 1]. In Dill group 21% and in gemfibrozil group 34% of patients observed low-fat diet. As Table 2 shows, the mean level of cholesterol and triglyceride has been reduced in comparison to before treatment after treating with gemfibrozil (P < 0.001). Also, in Dill group, the mean level of cholesterol and triglyceride has been reduced in comparison to before treatment (P < 0.001) but there was not a significant difference between the mean level of HDL in Dill group, before and after treatment [Table 3].
Figure 1.
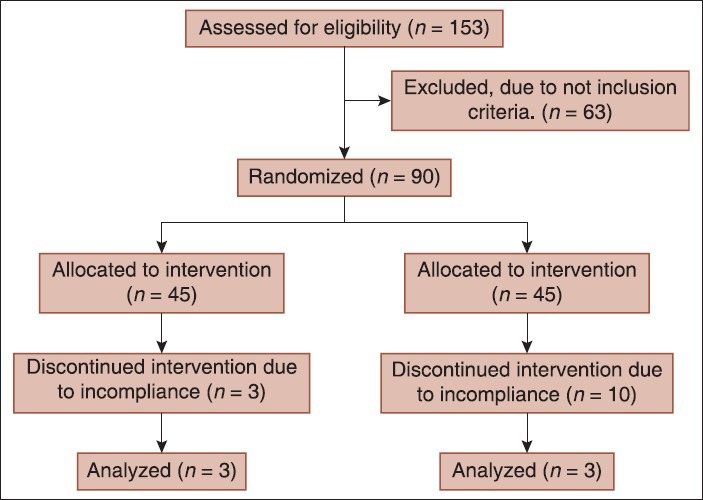
Flow diagram of the progress through the phases of parallel randomized trial of two groups
Table 1.
Comparison of cholesterol, triglyceride and HDL average in two groups
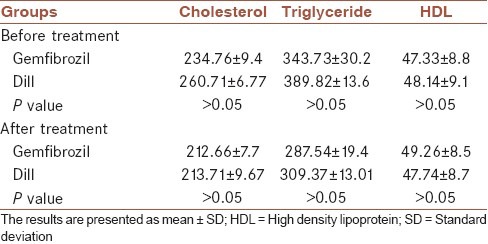
Table 2.
Comparison of cholesterol, triglyceride and HDL average before and after treatment with gemfibrozil
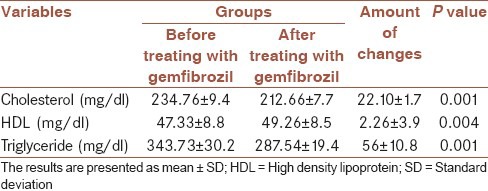
Table 3.
Comparison of cholesterol, triglyceride and HDL average before and after treatment with Dill
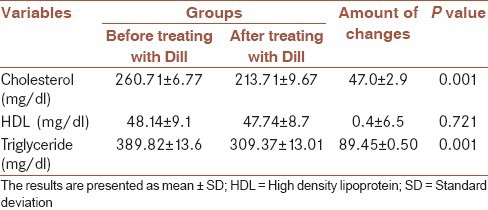
By using Dill, the mean level of cholesterol was reduced by 18%, and by using gemfibrozil, it was reduced by 9.41% (P < 0.05). Gemfibrozil and Dill has reduced triglyceride by 32.7% and 7.38%, respectively (P < 0.05). Gemfibrozil has increased HDL by 3.91%, but Dill reduced it by 0.8% (P < 0.05) [Table 2].
By using Dill, patients did not express any signs of adverse effects. However, 21.4% of patients who used gemfibrozil reported gastrointestinal complications.
DISCUSSION
In this study, results showed that Dill had less impact on triglyceride and HDL in comparison to gemfibrozil but reduced cholesterol more. Dill impact on reducing patients’ cholesterol was statistically significant in comparison to gemfibrozil. However, it should be considered that gemfibrozil has been known as an effective drug on triglyceride, and in previous studies gemfibrozil had little impact on cholesterol. On the other hand, cholesterol average in patients pre-treated with Dill is nearly equal to normal maximum (240 mg/dg).
In a study that has been done on hyperlipidemic patients, Dill effect has been compared with cholestyramine, nicotinic acid, and placebo that Dill has not statistically had a significant difference with placebo in reducing cholesterol and triglyceride and it had not been effective in comparison to other known drugs.[27] The only other independent research that has shown appropriate effect of Dill on hyperlipidemia is the study that Institute of biochemistry and biophysics, Tehran University, has studied the essence of Dill leave on blood lipids in rat.[32]
It is not clear that with what mechanism Dill plant is effective on hyperlipidemia, but in other studies done on the impact of several volatile compounds it has been shown that antioxidants are the main reason for hypolipidemic and antitoxic activities of these plants.[33,34,35,36]
According to the above study and inconsistent results for an exact comment about the Dill drug, it seems that doing more comprehensive studies on Dill effect on blood lipids and their mechanism are required. As mentioned in the result section, no side effect was reported. In examining gemfibrozil effects, patients just mentioned gastrointestinal complications and because of time limitation, it was not possible to investigate other effects of gemfibrozil like increased risk of gallstones, myopathy, and so on.
Totally, according to the limited effects of Dill and good impact of this drug on cholesterol and blood triglyceride, it seems that Dill is an appropriate drug for treating hyperlipidemia and triglyceride.
AUTHORS’ CONTRIBUTIONS
MM contributed in the conception and design of the work and agreed for all aspects of the work. AB contributed in revising the draft, approval of the final version of the manuscript. MRK contributed in the conception of the work, preparing and revising the draft and agreed for all aspects of the work.
ACKNOWLEDGEMENT
The research work was financially supported by Research Deputy of Shahrekord University of Medical Sciences, Shahrekord, Iran (research project number 886).
Footnotes
Source of Support: This study was financially supported by Research Deputy of Shahrekord University of Medical Sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–78. doi: 10.1016/S0140-6736(05)67394-1. [DOI] [PubMed] [Google Scholar]
- 2.Nasri H, Sahinfard N, Rafieian M, Rafieian S, Shirzad M, Rafieian-Kopaei M. Effects of Allium sativum on liver enzymes and atherosclerotic risk factors. J HerbMed Pharmacol. 2013;2:23–8. [Google Scholar]
- 3.Hayakawa H, Raij L. Relationship between hypercholesterolaemia, endothelial dysfunction and hypertension. J Hypertens. 1999;17:611–9. doi: 10.1097/00004872-199917050-00004. [DOI] [PubMed] [Google Scholar]
- 4.Asgary S, Sahebkar A, Afshani MR, Keshvari M, Haghjooyjavanmard S, Rafieian-Kopaei M. Clinical evaluation of blood pressure lowering, endothelial function improving, hypolipidemic and anti-inflammatory effects of pomegranate juice in hypertensive subjects. Phytother Res. 2014;28:193–9. doi: 10.1002/ptr.4977. [DOI] [PubMed] [Google Scholar]
- 5.Kazemi S, Asgary S, Moshtaghian J, Rafieian M, Adelnia A, Shamsi F. Liver-protective effects of hydroalcoholic extract of allium hirtifolium boiss. In rats with alloxan-induced diabetes mellitus. ARYA Atheroscler. 2010;6:11–5. [PMC free article] [PubMed] [Google Scholar]
- 6.Asgary S, Rafieian-Kopaei M, Najafi S, Heidarian E, Sahebkar A. Antihyperlipidemic effects of Sesamum indicum L. in rabbits fed a high-fat diet. Scientific World Journal 2013. 2013 doi: 10.1155/2013/365892. 365892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rafieian-Kopaie M, Nasri H. Serum lipoprotein (a) and atherosclerotic changes in hemodialysis patients. J Renal Inj Prev. 2013;2:47–50. doi: 10.12861/jrip.2013.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Khosravi-Boroujeni H, Mohammadifard N, Sarrafzadegan N, Sajjadi F, Maghroun M, Khosravi A, et al. Potato consumption and cardiovascular disease risk factors among Iranian population. Int J Food Sci Nutr. 2012;63:913–20. doi: 10.3109/09637486.2012.690024. [DOI] [PubMed] [Google Scholar]
- 9.Khajehdehi P. Turmeric: Reemerging of a neglected Asian traditional remedy. J Nephropathol. 2012;1:17–22. doi: 10.5812/jnp.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Asgary S, Kelishadi R, Rafieian-Kopaei M, Najafi S, Najafi M, Sahebkar A. Investigation of the lipid-modifying and antiinflammatory effects of Cornus mas L. supplementation on dyslipidemic children and adolescents. Pediatr Cardiol. 2013;34:1729–35. doi: 10.1007/s00246-013-0693-5. [DOI] [PubMed] [Google Scholar]
- 11.Baradaran A, Mahmoud Rafieian-Kopaei M. Histopathological study of the combination of metformin and garlic juice for the attenuation of gentamicin renal toxicity in rats. J Renal Inj Prev. 2012;2:15–21. doi: 10.12861/jrip.2013.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nasri H, Nematbakhsh M, Ghobadi S, Ansari R, Shahinfard N, Rafieian-Kopaei M. Preventive and curative effects of ginger extract against histopathologic changes of gentamicin-induced tubular toxicity in rats. Int J Prev Med. 2013;4:316–21. [PMC free article] [PubMed] [Google Scholar]
- 13.Rafieian-Kopaie M. Medicinal plants for renal injury prevention. J Renal Inj Prev. 2013;2:63–5. doi: 10.12861/jrip.2013.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ardalan MR, Rafieian-Kopaei M. Is the safety of herbal medicines for kidneys under question? J Nephropharmacol. 2013;2:11–2. [PMC free article] [PubMed] [Google Scholar]
- 15.Tavafi M. Complexity of diabetic nephropathy pathogenesis and design of investigations. J Renal Inj Prev. 2013;2:59–62. doi: 10.12861/jrip.2013.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rafieian-Kopaie M. Metformin and renal injury protection. J Ren Inj Prev. 2013;2:91–2. doi: 10.12861/jrip.2013.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gheissari A, Mehrasa P, Merrikhi A, Madihi Y. Acute kidney injury: A pediatric experience over 10 years at a tertiary care center. J Nephropathol. 2012;1:101–8. doi: 10.5812/nephropathol.7534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rouhi H, Ganji F. Effects of N-acetyl cysteine on serum lipoprotein (a) and proteinuria in type 2 diabetic patients. J Nephropathol. 2013;2:61–6. doi: 10.5812/nephropathol.8940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rafieian-Kopaei M. Medicinal plants and the human needs. J HerbMed Plarmacol. 2012;1:1–2. [Google Scholar]
- 20.Behradmanesh S, Derees F, Rafieian-kopaei M. Effect of Salvia officinalis on diabetic patients. J Renal Inj Prev. 2013;2:51–4. doi: 10.12861/jrip.2013.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nasri H, Shirzad H. Toxicity and safety of medicinal plants. J HerbMed Plarmacol. 2013;2:21–2. [Google Scholar]
- 22.Rafieian-Kopaei M, Nasri H. Ginger and diabetic nephropathy. J Renal Inj Prev. 2012;2:9–10. doi: 10.12861/jrip.2013.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jafarzadeh L, Rafieian-Kopaei M, Samani RA, Asgari A. The effect of hydroalcoholic extract of Stachys lavandulifolia vahl on pregnant mice. EXCLI J. 2012;11:357–62. [PMC free article] [PubMed] [Google Scholar]
- 24.Sereshti M, Azari P, Rafieian M, Kheiri S. Use of herbal medicines by pregnant women in Shahrekord. Med J Rep Infertil. 2006;7:131–25. [Google Scholar]
- 25.Baradaran A, Rabiei Z, Rafieian M, Shirzad H. A review study on medicinal plants affecting amnesia through cholinergic system. J HerbMed Plarmacol. 2012;1:3–9. [Google Scholar]
- 26.Ravindran P, Balachandran I. Vol. 17. India: Publisher V K Krishnan Nair; 2005. Under utilized medicinal spices II, Spice India; pp. 32–6. [Google Scholar]
- 27.Setorki M, Rafieian-Kopaei M, Merikhi A, Heidarian E, Shahinfard N, Ansari R, et al. Suppressive impact of Anethum graveolens consumption on biochemical risk factors of atherosclerosis in hypercholesterolemic rabbits. Int J Prev Med. 2013;4:889–95. [PMC free article] [PubMed] [Google Scholar]
- 28.Shakiba-Dastgerdi A, Rafieian-kopaei M, Jivad N, Sedehi M, Yousefi-Darani M, Shirani F. Effect of hydro alcoholic extract of Anethum graveolens leaves on time response to pain stimuli in mice. J Shahrekord Univ Med Sci. 2013;15:70–6. [Google Scholar]
- 29.Hosseinzadeh H, Karimi GR, Ameri M. Effects of Anethum graveolens L. seed extracts on experimental gastric irritation models in mice. BMC Pharmacol. 2002;2:21. doi: 10.1186/1471-2210-2-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Setorki M, Shahinfard N, Ansari R, Forouzandeh Z, Asgharzadeh S, Rafieian-Kopaei M. Comparison between the effects of hydroalcoholic extract of Dill and statins on lipid profile. J Kerman Univ Med Sci. 2013;20:158–68. [Google Scholar]
- 31.Insua A, Massari F, Rodríguez Moncalvo JJ, Rubén Zanchetta J, Insua AM. Fenofibrate of gemfibrozil for treatment of types IIa and IIb primary hyperlipoproteinemia: A randomized, double-blind, crossover study. Endocr Pract. 2002;8:96–101. doi: 10.4158/EP.8.2.96. [DOI] [PubMed] [Google Scholar]
- 32.Yazdanparast R, Alavi M. Antihyperlipidaemic and antihypercholesterolaemic effects of Anethum graveolens leaves after the removal of furocoumarins. Cytobios. 2001;105:185–91. [PubMed] [Google Scholar]
- 33.Heidarian E, Rafieian-Kopaei M, Ashrafi K. The effect of hydroalcoholic extract of Allium latifolium on the liver phosphatidate phosphatase and serum lipid profile in hyperlipidemic rats. J Babol Univ Med Sci. 2013;15:37–46. [Google Scholar]
- 34.Rafieian-Kopaei M, Baradaran A, Rafieian M. Plants antioxidants: From laboratory to clinic. J Nephropathol. 2013;2:152–3. doi: 10.12860/JNP.2013.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tamadon MR, Ardalan MR, Nasri H. World Kidney Day 2013; acute renal injury; a global health warning. J Parathyr Dis. 2013;1:27–28. [Google Scholar]
- 36.Rafieian-Kopaei M, Baradaran A. Combination of metformin with other antioxidants may increase its renoprotective efficacy. J Renal Inj Prev. 2013;2:35–6. doi: 10.12861/jrip.2013.13. [DOI] [PMC free article] [PubMed] [Google Scholar]