

Abstract
Background:
Extracranial–intracranial arterial bypass surgery is rarely performed for recurrent or progressing stroke due to vertebrobasilar artery steno-occlusive disease. Non-enhanced 7.0-T magnetic resonance (MR) imaging reveals cerebral arteries more clearly than 3.0-T or less MR imaging.
Case Description:
A 45-year-old man developed recurrent transient ischemic attacks due to hemodynamic ischemia caused by occlusion of bilateral vertebral arteries despite antiplatelet therapy. MR angiography with a 7.0-T imager demonstrated that each marginal tentorial artery ran along the tentorial edge and anastomosed with each posterior cerebral artery (PCA) as collateral circulation. Superficial temporal artery (STA)–superior cerebellar artery (SCA) or PCA bypass surgery was planned through a subtemporal approach. During surgery, the SCA was not visible when the tentorial edge was elevated. The tentorium was not cut, and the STA was anastomosed with the P2 segment of the PCA. Ischemic symptoms completely resolved after surgery.
Conclusions:
Preoperative 7.0-T MR imaging visualized the marginal tentorial artery as an unusual collateral pathway in a patient with symptomatic bilateral vertebral artery occlusion undergoing arterial bypass surgery.
Keywords: 7.0-T MR imaging, arterial bypass surgery, collateral circulation, vertebral artery occlusion
INTRODUCTION
Symptomatic vertebrobasilar artery steno-occlusive disease is commonly treated with antiplatelet drugs. However, the early risk of stroke recurrence in patients with such pathogenesis is high,[2,4,15] and these patients require active preventive treatment.[14] Extracranial–intracranial arterial bypass surgery such as superficial temporal artery (STA) to superior cerebellar artery (SCA) anastomosis is rarely performed for recurrent or progressing stroke due to vertebrobasilar steno-occlusive disease.[1,12,13] With STA–SCA anastomosis, the SCA as a recipient artery is located under the tentorium. The tentorium is thus usually cut to expose the SCA and obtain a wide and shallow operative field.[6,13] Non-enhanced 7.0-T magnetic resonance (MR) imaging clearly reveals cerebral arteries that are not visible on MR imaging at 3.0 T or less.[3,5,7,9,10]
In this report, we describe a case involving a patient with frequent ischemic attacks and hemodynamic brain ischemia caused by occlusion of bilateral vertebral arteries (VAs). Preoperative 7.0-T MR imaging demonstrated collateral circulation running along the tentorial edge that had not been identified on cerebral angiography with arterial catheterization. Based on this MR finding, we performed STA–posterior cerebral artery (PCA) anastomosis instead of STA–SCA anastomosis, which would have involved cutting the tentorium.
CASE REPORT
History and examination
A 45-year-old man presented with minor stroke appearing as symptoms of dizziness and defects of the visual field, and 0.5-T MR imaging showed an infarct in the right occipital lobe. Administration of an antiplatelet drug was initiated. Six months later, the patient experienced transient ischemic attacks manifesting as dizziness and disturbance of consciousness. MR imaging using a 1.5-T imager showed spotty new ischemic lesions in the right cerebellum, pons, and left thalamus. MR angiography with the same imager revealed occlusion of bilateral VAs.
Cerebral angiography with arterial catheterization showed occlusion at the V3 segments of bilateral VAs. On common carotid angiography, bilateral posterior communicating arteries, bilateral marginal tentorial arteries, and the upper part of the basilar artery were faintly visible [Figure 1]. However, whether the former two arteries perfused the latter was unclear.
Figure 1.
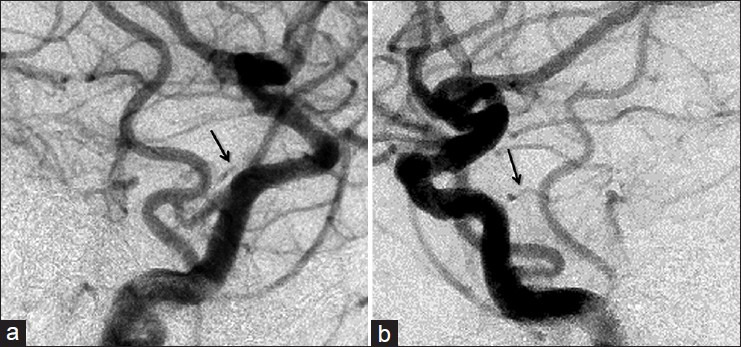
Preoperative common carotid angiography (a, right; b, left) shows bilateral marginal tentorial arteries (arrows) and the upper part of the basilar artery. The whole courses of the former arteries are unclear
Three-dimensional time-of-flight MR angiography with a 7.0-T imager (Signa 950; GE Medical Systems, Milwaukee, WI, USA) demonstrated that each marginal tentorial artery originating from each internal carotid artery ran along the tentorial edge and anastomosed with each PCA [Figure 2a]. The right SCA was located below each marginal tentorial artery [Figure 2b].
Figure 2.
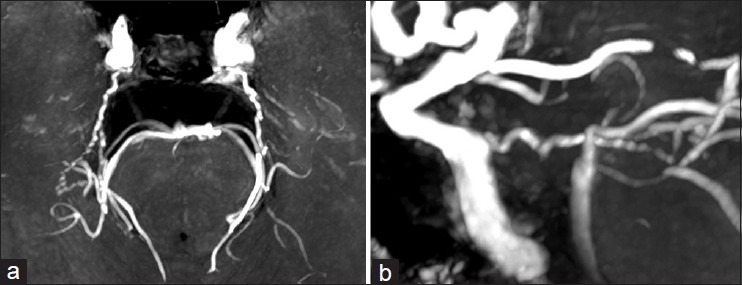
Maximum intensity projection of preoperative three-dimensional time-of flight magnetic resonance angiography using a 7.0-T imager and a 32-channel phased array coil for the brain to optimize signal detection with the image sequence from a spoiled gradient echo (repetition time, 12 ms; echo time, 2.9 ms; flip angle, 12°; matrix size, 512 × 512; field of view, 22 × 22 cm; slice thickness, 1.0 mm) revealing that each marginal tentorial artery originating from each internal carotid artery runs along the tentorial edge and anastomoses with each posterior cerebral artery (a). The right superior cerebellar artery is located below the right marginal tentorial artery (b)
Quantitative brain perfusion single-photon emission computed tomography (SPECT)[11] showed decreased cerebrovascular reactivity to acetazolamide in the cerebellum and bilateral occipital lobes; in the latter, blood flow was also reduced [Figure 3].
Figure 3.
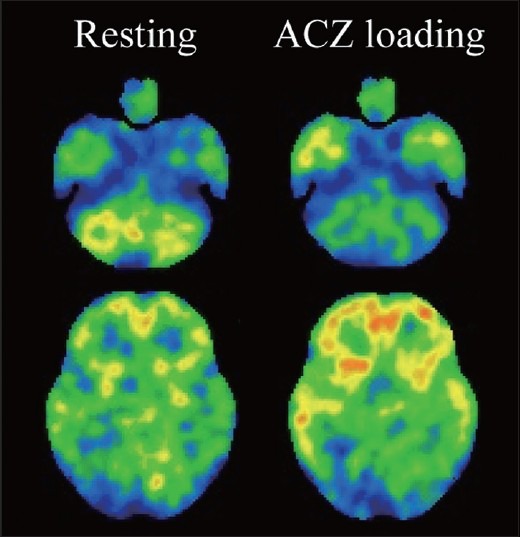
Preoperative quantitative brain perfusion single-photon emission computed tomography displaying decreased cerebral blood flow in bilateral occipital lobes (left column) and decreased cerebrovascular reactivity to acetazolamide in the cerebellum and bilateral occipital lobes (right column)
Operation and postoperative course
The patient suffered frequent orthostatic dizziness and we planned STA–SCA or PCA bypass surgery using a subtemporal approach through a right temporal craniotomy. During surgery, the SCA was not visible when the tentorial edge was elevated, as expected from preoperative 7.0-T MR angiography [Figure 2b]. The tentorium was not cut because it included the marginal tentorial artery as collateral circulation [Figure 2a], and the STA was anastomosed with the P2 segment of the PCA.
Orthostatic dizziness completely resolved after surgery and postoperative angiography demonstrated that the entire posterior circulation was perfused via an anastomosed STA [Figure 4].
Figure 4.
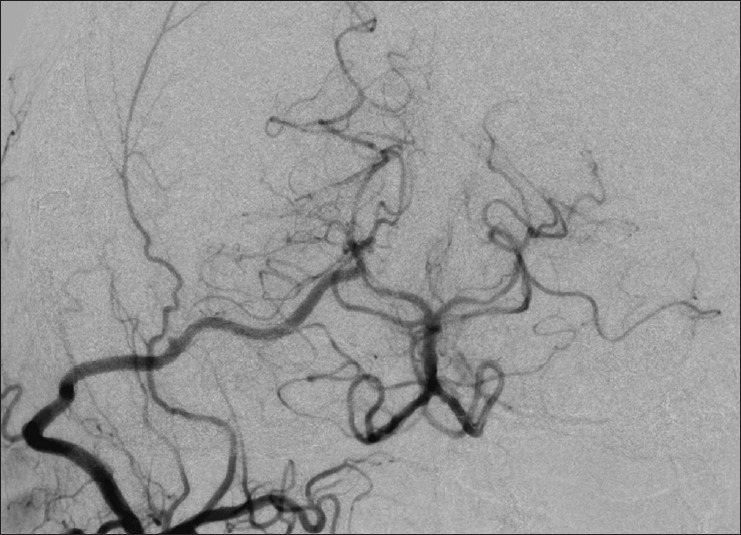
Postoperative cerebral angiography demonstrating the entire posterior circulation perfused via an anastomosed superficial temporal artery
DISCUSSION
The patient discussed in this report suffered frequent ischemic attacks due to hemodynamic brain ischemia in the posterior circulation as detected on brain perfusion SPECT, and underwent vascular reconstructive surgery. The degree of atherosclerosis is usually greater in the proximal portion of the PCA than in the SCA,[13] and the former runs in the crural cistern deeper than the latter. Thus, on extracranial–intracranial arterial bypass surgery for the posterior circulation, the SCA is used more frequently than the PCA as a recipient artery.[1,13] In the present case, preoperative 7.0-T MR imaging demonstrated the collateral circulation running along the tentorial edge, suggesting that the affected area acutely fell into more severe brain ischemia when the tentorium was cut. Furthermore, the SCA was not visible when the tentorial edge was elevated during surgery. The STA was thus anastomosed with the PCA instead of the SCA.
When the VAs are occluded bilaterally and collateral flow via the posterior communicating arteries is insufficient and, as a result, basilar arterial blood supply is tenuous, retrograde flow through the anterior spinal artery can provide collateral circulation.[8] The present case suggested the marginal tentorial artery might offer another potentially important collateral supply to the neural contents of the posterior fossa.
Several investigators have demonstrated that 7.0-T MR imaging visualized the perforating arteries as well as the large vessels of the circle of Willis or the first- and second-order branches in more detail than 1.5- or 3.0-T MR imaging.[5,7,10] In addition, 7.0-T MR imaging also showed similar angiographic findings to angiography with arterial catheterization, regarding visualization of the lenticulostriate arteries.[3] In the present case, the collateral circulation from the marginal tentorial artery to the PCA was displayed more clearly on 7.0-T MR imaging than on angiography with arterial catheterization. Thus, 7.0-T MR imaging may be advantageous for displaying unexpected collateral pathways such as the marginal tentorial artery in patients with vertebrobasilar occlusive disease, particularly when vascular reconstructive surgery is considered.
ACKNOWLEDGMENTS
This work was partly supported by Grant-in-Aid for Strategic Medical Science Research (S1491001, 2014-2018) from the Ministry of Education, Culture, Sports, Science and Technology of Japan; JSPS KAKENHI Grant Number 2612345.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2014/5/1/157/143760
Contributor Information
Yuiko Sato, Email: norimori@iwate-med.ac.jp.
Kuniaki Ogasawara, Email: kuogasa@iwate-med.ac.jp.
Kenji Yoshida, Email: kenyoshi@iwate-med.ac.jp.
Makoto Sasaki, Email: masasaki@iwate-med.ac.jp.
REFERENCES
- 1.Ausman JI, Diaz FG, Vacca DF, Sadasivan B. Superficial temporal and occipital artery bypass pedicles to superior, anterior inferior, and posterior inferior cerebellar arteries for vertebrobasilar insufficiency. J Neurosurg. 1990;72:554–8. doi: 10.3171/jns.1990.72.4.0554. [DOI] [PubMed] [Google Scholar]
- 2.Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet. 1991;337:1521–6. doi: 10.1016/0140-6736(91)93206-o. [DOI] [PubMed] [Google Scholar]
- 3.Cho ZH, Lee YB, Kang CK, Yang JW, Jung IH, Park CA, et al. Microvascular imaging of asymptomatic MCA steno-occlusive patients using ultra-high-field 7T MRI. J Neurol. 2013;260:144–50. doi: 10.1007/s00415-012-6604-5. [DOI] [PubMed] [Google Scholar]
- 4.Hankey GJ, Jamrozik K, Broadhurst RJ, Forbes S, Burvill PW, Anderson CS, et al. Long-term risk of first recurrent stroke in the Perth Community Stroke Study. Stroke. 1998;29:2491–500. doi: 10.1161/01.str.29.12.2491. [DOI] [PubMed] [Google Scholar]
- 5.Heverhagen JT, Bourekas E, Sammet S, Knopp MV, Schmalbrock P. Time-of-fright magnetic resonance angiography at 7 tesla. Invest Radiol. 2008;43:568–73. doi: 10.1097/RLI.0b013e31817e9b2c. [DOI] [PubMed] [Google Scholar]
- 6.Hopkins LN, Martin NA, Hadley MN, Spetzler RF, Budny J, Carter LP. Vertebro-basilar insufficiency. Part 2: Microsurgical treatment of intracranial vertebrobasilar disease. J Neurosurg. 1987;66:662–74. doi: 10.3171/jns.1987.66.5.0662. [DOI] [PubMed] [Google Scholar]
- 7.Kang CK, Park CA, Kim KN, Hong SM, Park CW, Kim YB, et al. Non-invasive visualization of basilar artery perforators with 7T MR angiography. J Magn Reson Imaging. 2010;32:544–50. doi: 10.1002/jmri.22250. [DOI] [PubMed] [Google Scholar]
- 8.Kang HS, Han MH, Kim SH, Kwon OK, Roh HG, Ko YC. Anterior spinal artery as a collateral channel in cases of bilateral vertebral arterial steno-occlusive diseases. AJNR Am J Neuroradiol. 2007;28:222–5. [PMC free article] [PubMed] [Google Scholar]
- 9.Maderwald S, Ladd SC, Gizewski ER, Kraff O, Theysohn JM, Wicklow K, et al. To TOF or not to TOF: Strategies for non-contrast-enhanced intracranial MRA at 7 T. MAGMA. 2008;21:159–67. doi: 10.1007/s10334-007-0096-9. [DOI] [PubMed] [Google Scholar]
- 10.von Morze C, Xu D, Purcell DD, Hess CP, Mukherjee P, Saloner D, et al. Intracranial time-of-flight MR angiography at 7T with comparison to 3T. J Magn Reson Imaging. 2007;26:900–4. doi: 10.1002/jmri.21097. [DOI] [PubMed] [Google Scholar]
- 11.Ogasawara K, Ito H, Sasoh M, Okuguchi T, Kobayashi M, Yukawa H, et al. Quantitative measurement of regional cerebrovascular reactivity to acetazolamide using 123I-N-isopropyl-p-iodoamphetamine autoradiography with SPECT: Validation study using H2 15O with PET. J Nucl Med. 2003;44:520–5. [PubMed] [Google Scholar]
- 12.Ogasawara K, Sasaki M, Tomitsuka N, Kubo Y, Inoue T, Ogawa A, et al. Early revascularization in a patient with perfusion computed tomography/diffusion-weighted magnetic resonance imaging mismatch secondary to acute vertebral artery occlusion. Neurol Med Chir. 2005;45:306–10. doi: 10.2176/nmc.45.306. [DOI] [PubMed] [Google Scholar]
- 13.Ogawa A, Kameyama M, Muraishi K, Yoshimoto T, Ito M, Sakurai Y. Cerebral blood flow and metabolism following superficial temporal artery to superior cerebellar artery bypass for vertebrobasilar occlusive disease. J Neurosurg. 1992;76:955–60. doi: 10.3171/jns.1992.76.6.0955. [DOI] [PubMed] [Google Scholar]
- 14.Ota T, Usami K, Iijima A, Saito N. Staged surgical treatment for symptomatic vertebrobasilar artery stenosis: Combined treatment with endovascular angioplasty and bypass surgery. World Neurosurg. 2012;78:90–4. doi: 10.1016/j.wneu.2011.12.006. [DOI] [PubMed] [Google Scholar]
- 15.Prognosis of patients with symptomatic vertebral or basilar artery stenosis. The Warfarin-Aspirin Symptomatic Intracranial Disease. (WASID) Study Group. Stroke. 1998;29:1389–92. doi: 10.1161/01.str.29.7.1389. [DOI] [PubMed] [Google Scholar]