

Abstract
IQP-GC-101 is a patented blend of the standardized extracts of Garcinia cambogia, Camellia sinensis, unroasted Coffea arabica, and Lagerstroemia speciosa. These individual ingredients of IQP-GC-101 have each shown promise in promoting weight loss; however, the efficacy of the blend has not been established. This randomized, placebo-controlled, double-blind, parallel group study conducted over 14 weeks (including a 2-week run-in phase) aimed to investigate the efficacy and safety of IQP-GC-101 in reducing body weight and body fat mass in overweight Caucasian adults. Subjects took three IQP-GC-101 or placebo tablets, twice a day, 30 min before main meals. All subjects also adhered to a 500 kcal/day energy deficit diet with 30% of energy from fat. Ninety-one overweight and mildly obese subjects (46 in the IQP-GC-101 group, 45 in the placebo group) completed the study. After 12-week intervention, IQP-GC-101 resulted in a mean (±SD) weight loss of 2.26 ± 2.37 kg compared with 0.56 ± 2.34 kg for placebo (pU = 0.002). There was also significantly more reduction in body fat mass, waist circumference, and hip circumference in the IQP-GC-101 group. No serious adverse events were reported. The use of IQP-GC-101 has been shown to result in body weight and body fat reduction in the current study, with good tolerability. © 2014 InQpharm Group Sdn Bhd. Phytotherapy Research published by John Wiley & Sons, Ltd.
Keywords: herbal extracts, weight management, overweight, body fat, obesity
INTRODUCTION
Being obese or overweight can lead to a multitude of health problems. Research shows that the risk of coronary artery disease increases by 3.6 times with each unit of body mass index (BMI, measured in kg/m2), 85% of hypertension is associated with BMIs of more than 25 kg/m2, and 90% of patients suffering from type 2 diabetes have a BMI of more than 23 kg/m2 (Kopelman, 2007). It has been estimated that a weight loss of 5 kg over time could account for a 55% reduction in the risk of diabetes among obese, prediabetes individuals (over a mean of 3.2 years follow-up) (Hamman et al., 2006). Weight reduction has also been associated with a markedly reduced risk of cardiovascular diseases (Fayh et al., 2013).
Managing obesity requires a two-pronged reducing energy intake as well as increasing energy expenditure. Current available drug treatments for obesity, for example, appetite suppressant (e.g., phentermine and toperamide) or lipase inhibitor (orlistat), focus primarily on reducing caloric intake, while IQP-GC-101, investigated in this study, offers the possibility of increasing thermogenesis and metabolism in supporting weight loss.
IQP-GC-101, a patented herbal blend that contains the standardized extracts of Garcinia cambogia (Malabar tamarind), Camellia sinensis (green tea), unroasted Coffea arabica (green coffee), and Lagerstroemia speciosa (banaba) in a specific ratio, is hypothesized to reduce body weight by inhibition of de novo fatty acid synthesis (Heymsfield et al., 1998) and stimulation of metabolic rate and thermogenesis (Dulloo et al., 1999; Acheson et al., 1980; Satomi et al., 2006). All four active ingredients of IQP-GC-101 are common herbs that have been used for generations as food in different parts of the world and have shown potential individually as weight loss supplements.
Garcinia cambogia is cultivated in Southeast Asia, India, and west and central Africa and is used extensively for culinary purposes in Asian countries (Jayaprakasha and Sakariah, 1998). G. cambogia is also included in the US Department of Agriculture inventory of perennial edible fruits of the tropics (Martin et al., 1987). The extract of G. cambogia has been widely marketed as a weight loss supplement worldwide. Its weight loss effect has mainly been attributed to its high (−)-hydroxycitric acid (HCA) content. Several mechanisms of action have been linked to the weight loss effect of HCA through prior animal studies, including (1) inhibition of lipogenesis through adenosine triphosphate citrate lyase inhibition, which prevents the conversion of carbohydrate to fat (Sullivan et al., 1977); (2) suppression of appetite through increasing glycogen storage thus stimulating the glucoreceptors in the liver and inducing satiety via vagus nerve (Sullivan et al., 1974); (3) reduction of the hunger feeling by increasing the level of serotonin (Ohia et al., 2002); and (4) improved glucose metabolism through regulation of leptin and insulin plasma level (Hayamizu et al., 2003). A recent review of animal and human studies established the safety profile of HCA (Chuah et al., 2012). However, the weight loss efficacy of HCA in human study has shown equivocal findings with studies reporting both negative (Heymsfield et al., 1998) and positive results (Mattes and Bormann, 2000). According to a meta-analysis by Onakpoya et al. (2011a), although supplementation of HCA results in a small statistically significant weight loss effect over placebo, the clinical relevance is still uncertain. Trials with adequate sample size and duration are still needed to confirm HCA’s weight loss efficacy.
Camellia sinensis is the source of different types of tea, one of the most widely consumed drinks in the world (Hursel et al., 2009). Extract of green tea made from the fresh leaves of C. sinensis, containing a mixture of catechin polyphenol and caffeine (epigallocatechin gallate [EGCG]-caffeine), has been suggested to possess anti-obesity effect, mainly through the promotion of fat oxidation and thermogenesis (Dulloo et al., 1999). A meta-analysis by Hursel et al. (2009) concludes that there is a positive but small effect of EGCG-caffeine mixture on weight loss and weight maintenance. Whether green tea extract may have potential synergistic effect with the other active ingredients in IQP-GC-101 on body weight regulation remains an interesting question to be addressed.
Green coffee extract has also been associated with weight loss. In an animal study, two major constituents of green coffee extract, that is, caffeine and chlorogenic acid have been shown to play a role in suppressing fat absorption and enhancing fat metabolism in the liver, respectively (Shimoda et al., 2006). Despite the positive results in animals, validity of human studies conducted to access the efficacy of green coffee extract on weight loss is still questionable. In a recent systematic review, clinical trials that reported the weight loss effect of green coffee extract have been found to be associated with high risk of bias due to the small sample size and short study duration among other study short falls (Onakpoya et al., 2011b).
Lagerstroemia speciosa is a tropical plant found in Southeast Asia. Its leaves are used in the Philippines as a traditional treatment for diabetes and kidney disease (Klein et al., 2007). It has been studied in animals for hypoglycemic and adipocyte-differentiation inhibition activities (Liu et al., 2001; Deocaris et al., 2005).
Notably, a previous clinical study has evaluated the effectiveness and safety of a tablet product containing these four herbal extracts. The blood glucose level was reduced significantly after consumption of the tablet containing the herbal composition in comparison to the placebo. The study, however, did not report any weight loss effect of this combination (Stobs et al., 2012). A pilot study (unpublished) was conducted previously on the effects of the present combination on body weight loss. In this study, conducted on Asian subjects, the herbal combination has shown promising results in weight loss compared with HCA alone, or a placebo. As there are differences in metabolic characteristics between different ethnic groups (Razak et al., 2005), the outcomes of this pilot study may not be applicable to the European population. The objective of this study was to investigate the effects of IQP-GC-101 on body weight and body fat reduction in overweight Caucasians.
METHODS
Subject recruitment
The study took place in two centers in Berlin, Germany, from July 2011 to December 2011, and was approved by the ethics committee of the Charité Universitatsmedizin prior to initiation. Newspaper advertisement was used for subject recruitment. All subjects provided written informed consent before screening procedures were performed.
Subjects were between 18 and 60 years, and had to fulfill the following inclusion criteria: (1) body mass index (BMI) between 25 and 32 kg/m2; (2) stable body weight for the past 3 months before study enrollment; (3) be accustomed to 3 meals a day; (4) be committed to adhere to the diet plan; (5) agree to not use other weight loss products during the study period; and (6) agree to use appropriate contraceptive plans (for females of childbearing potential).
The exclusion criteria for the study included: (1) known hypersensitivity to any of the ingredients of the investigational product; (2) afflicted with or had a history of systemic or gastrointestinal diseases that may confound the outcomes of the study; (3) pregnant or nursing; (4) history of eating disorder; (5) history of bariatric surgery; (6) use of other weight loss products within 6 weeks before enrollment; (7) change in dosage of estrogen, oral contraceptives, and thyroid hormone within the last 3 months prior to enrollment; (8) concurrent use of medication that might affect body weight for example systemic corticosteroids and antidepressants; (9) smoking cessation within 6 months prior to the start of the study; (10) participated in other clinical trials within 4 weeks prior to enrollment; and (11) inability to comply to study procedures.
Study design
A randomized, placebo-controlled, double-blind, parallel group study was conducted over 14 weeks, including a 2-week run-in phase. After fulfilling all inclusion/exclusion criteria, subjects entered the run-in phase, during which their adherence to the diet plan assigned and investigational product intake (placebo) were assessed.
Compliant subjects were then randomized to either IQP-GC-101 or a matching placebo. Follow-up visits were conducted at weeks 4, 8, and 12 following randomization.
This clinical investigation was performed according to the principles of the World Medical Association (Declaration of Helsinki), the European Union recommendations for Good Clinical Practice (CPMP/ICH/135/95), ICH E6 (R1), and ICH E3, as well as the German GCP-V (2004, revised 2006). The study was registered on clinicaltrials.gov (ID: NCT01423617).
Interventions
All subjects received diet counseling and a diet plan that provided them with a 500 kcal deficit diet (calculated on the basis of each individual’s body weight, height, age, gender, and activity level). The diet plans were compiled by a dietician and ensured a balanced diet providing 30% of the ingested energy as fat. In total, plans for five levels of energy were available: 1500, 1800, 2000, 2200, and 2500 kcal per day. A food diary was maintained by all subjects in order for diet compliance to be monitored.
Each tablet of IQP-GC-101 (supplied by InQpharm Europe Ltd.) contained 850 mg of standardized extracts in a specific ratio: G. cambogia extract (650 mg) – standardized to at least 60% HCA, C. sinensis extract (100 mg) – at least 15% epigallocatechin-3-gallate and 11% caffeine, unroasted C. arabica extract (75 mg) – at least 25% chlorogenic acid and 5% caffeine, and L. speciosa extract (25 mg) – at least 5% corosolic acid. The placebo was identical in appearance to the intervention, and the active ingredients were substituted with microcrystalline cellulose and dicalcium phosphate. Subjects were instructed to take three tablets of IQP-GC-101 or placebo, twice a day, 30 min before breakfast and lunch. Subjects in the IQC-GC-101 group consumed a total of 5.10 g of standardized extracts daily.
Randomization
Randomization was generated using permuted blocks of four, and the randomization codes were kept by an independent biostatistics department. The investigator received sealed envelopes containing allocation information to either the intervention or placebo for each randomized subject. As this study was performed in a double-blind method, neither the investigator nor the subject was aware of the treatment allocation. In cases of emergency (i.e., serious adverse event), the investigator was allowed to open the envelope, which contained subjects’ allocation information.
Outcome measurements
Differences between IQP-GC-101 and placebo in mean loss of body weight (kg) and body fat mass (kg) after 12 weeks of intervention were the primary outcomes of this study. Secondary outcomes included change in fat free mass (kg), waist circumference (cm), and hip circumference (cm). These parameters were measured at baseline, weeks 4, 8, and 12.
Body weight was measured in kilogram using calibrated Tanita BC-420 SMA scales. The same scales were used to measure body fat mass and fat free mass (in kg) using bioelectrical impedance analysis. Height (cm) was measured using a wall-mounted stadiometer (KaWe Person-check).
Waist circumference (cm) was measured at the level midway between the lateral lower rib margin and the iliac crest. Hip circumference (cm) was measured as the maximal circumference over the buttocks.
The Control of Eating Questionnaire (COEQ) (Greenway et al., 2010) was completed at baseline, weeks 4, 8, and 12. The COEQ contains 21 items (20 of which are presented as visual analog scales) and measures hunger, fullness, the desire to eat different types of food, food cravings, and mood and alertness. The visual analog scale responses were measured in millimeters (mm) on a 100-mm scale.
Fasting venous blood samples were obtained at the screening and the final visits. Parameters assessed were full blood count, electrolyte levels, liver function, renal function, lipid metabolism, and carbohydrate metabolism. Analysis was conducted in a central laboratory.
Sample size and statistical analysis
Assuming a dropout rate of 10%, a sample size of 46 subjects per arm was calculated to provide a 4.75% (two-sided) significance level, with 80% power. Statistical analysis was performed with IBM© spss© Statistics, Version 19 (IBM Corp, Armonk, NY, USA). There were two primary endpoints in this study: 1. change in body weight and 2. change in body fat between baseline and week 12 of treatment. The testing of the primary endpoints data was performed with the non-parametric Mann–Whitney U test by analyzing the rank sums (pU) and covariance analysis (pANOVA). All primary and secondary endpoints went through an explorative examination and were descriptively assessed. Frequency distribution was analyzed using the Chi-squared test (pChi).
The first primary endpoint (body weight) was tested first with a significance level (type I error) of 4.75% (two-tailed test) or of 2.38% for the one-tailed test. As this null hypothesis was refuted the second primary outcome parameter (body fat mass) was tested with a 4.75% (two-tailed) or a 2.38% (one-tailed) significance level. Other tests were performed with a significance level (type I error) of 5.0% (two-tailed test) or of 2.5% for the one-tailed test.
For the primary endpoints, p-values of less than 0.0475 (two-tailed test) indicate a significant difference, for other tests, p-values of less than 0.05 indicate a significant difference. Data analysis was performed on the intent to treat (ITT) population.
RESULTS
Of the 102 subjects who entered the run-in phase, 92 were randomized. One subject (placebo arm) was lost to follow-up after randomization; 91 subjects were included in the ITT population for final analysis (Fig. 1). A total of 84 subjects fully complied with the study protocol (per protocol population). Out of the 91 subjects from ITT population, 46 were randomized to the IQP-GC-101 and 45 to the placebo arm.
Figure 1.
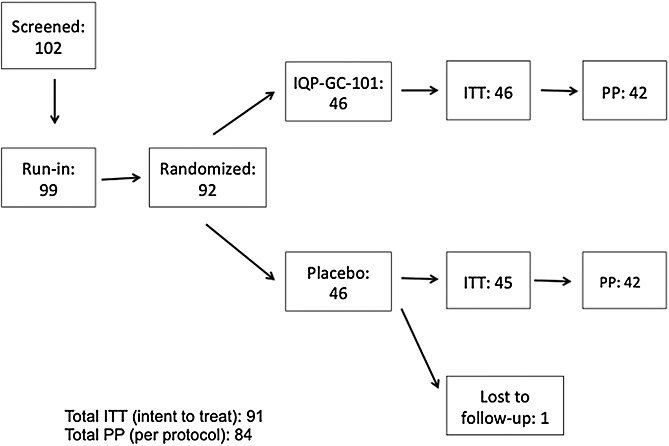
Subject flow. Of the 102 subjects who entered the run-in phase, 92 were randomized. 91 subjects were included in the intent to treat population for final analysis.
Demographics
All subjects recorded their ethnicity as ‘Caucasian’. The mean age of the subjects at screening was 42.8 ± 11.2 years. 29 out of 91 subjects (31.9%) were male. The gender distribution between the IQP-GC-101 group and the placebo group was not significantly different (pChi = 0.231). The mean height of the subjects was 169.6 ± 10.8 cm in the IQP-GC-101 group and 170.6 ± 9.1 cm in the placebo group. There was no significant difference between the two groups in the distribution of subjects in terms of mean age, height and body weight (Table 1).
Table 1.
Subjects’ demographics at baseline
| Parameters | IQP-GC-101 | Placebo | pChi-value |
|---|---|---|---|
| Number (%) | Number (%) | ||
| Gender (male) | 12 (26.1) | 17 (37.8) | 0.231 |
| Mean ± SD | Mean ± SD | pU-value | |
| Age (years) | 43.1 ± 10.8 | 42.5 ± 11.6 | 0.809 |
| Height (cm) | 169.6 ± 10.8 | 170.6 ± 9.1 | 0.289 |
| Body weight (kg) | 82.3 ± 12.3 | 83.3 ± 9.6 | 0.487 |
Compliance
Compliance to the investigational product was defined as an intake of between 75% and 125% of the number of tablets to be consumed according to instructions. All subjects complied with the dosing regimen. There was no significant difference in the compliance rate between the two arms during the study period (pU = 0.857).
Body weight
At baseline, the mean body weight of subjects was 82.3 ± 12.3 kg in the IQP-GC-101 group and 83.3 ± 9.6 kg in the placebo group (pU = 0.487). By week 12, subjects on IQP-GC-101 experienced significantly more weight loss (2.26 ± 2.37 kg) compared with subjects on placebo (0.56 ± 2.34 kg) (pU = 0.002) (Fig. 2). This is confirmed by covariance analysis (p(ANOVA) = 0.001).
Figure 2.
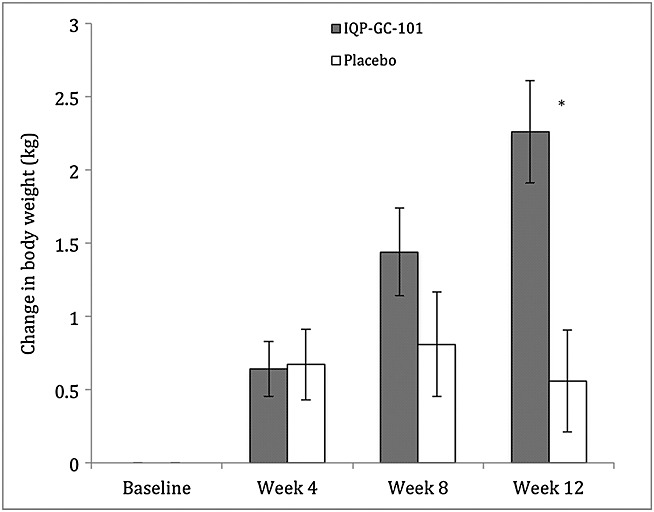
Body weight change in the intent to treat population. Error bars represent one standard error of mean. Positive values indicate reduction in body weight, in relation to baseline. * indicates a statistically significant difference in weight loss between the subjects on IQP-GC-101 and the subjects on placebo (pU = 0.002).
Body fat
The body fat of the subjects in both groups was not significantly different at baseline. Subjects randomized to IQP-GC-101 had a reduction in body fat from baseline to week 12. On the other hand, their placebo counterparts lost body fat at week 4, but regained it at weeks 8 and 12. By the end of the study, subjects on IQP-GC-101 lost a mean of 1.12 ± 1.84 kg of body fat, compared with subjects on placebo, who gained a mean of 0.37 ± 2.14 kg of body fat (pU = 0.001) (Fig. 3). This is confirmed by covariance analysis (p(ANOVA) = 0.001).
Figure 3.
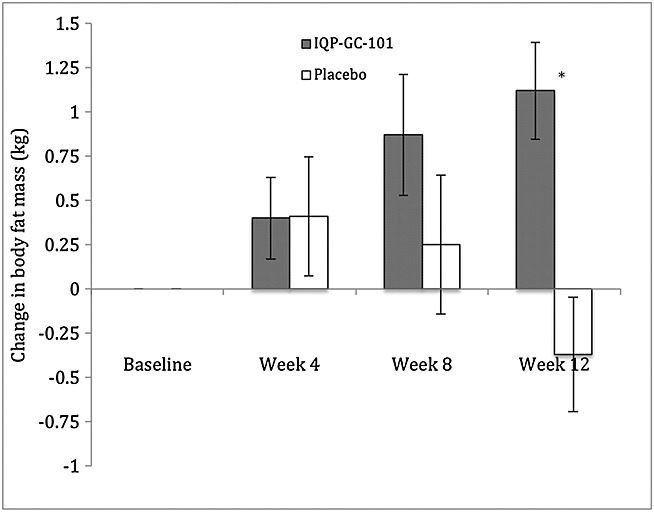
Body fat mass change in the intent to treat population. Error bars represent one standard error of mean. Positive values indicate decrease in body fat mass, while negative values indicate increase in body fat mass, in relation to baseline. * indicates a statistically significant difference in change in body fat mass between the subjects on IQP-GC-101 and the subjects on placebo (pU = 0.001).
Secondary outcomes (Table 2)
Table 2.
Secondary outcomes measurement
| Parameters | Unit | IQP-GC-101 | Placebo | pU-value | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Week 12 | Difference | Baseline | Week 12 | Difference | |||
| BMI | kg/m2 | 28.5 ± 2.1 | 27.7 ± 2.3 | 0.78 ± 0.81 | 28.6 ± 1.8 | 28.3 ± 1.9 | 0.22 ± 0.80 | 0.002 |
| Fat free mass | kg | 53.7 ± 10.9 | 52.6 ± 11.0 | 1.10 ± 1.60 | 55.2 ± 10.0 | 54.2 ± 10.0 | 1.00 ± 1.58 | 0.899 |
| Waist circumference | cm | 98.5 ± 8.5 | 96.5 ± 8.6 | 2.00 ± 2.44 | 101.0 ± 8.6 | 100.3 ± 8.8 | 0.69 ± 2.24 | 0.006 |
| Hip circumference | cm | 108.3 ± 6.4 | 106.7 ± 6.7 | 1.54 ± 1.76 | 108.7 ± 6.4 | 108.1 ± 6.7 | 0.64 ± 1.91 | 0.019 |
BMI, body mass index.
BMI: Accordingly, in line with body weight data, subjects on IQP-GC-101 also experienced a greater reduction in BMI compared with their placebo counterparts, from baseline to week 12.
Waist and hip circumference: The circumference for both the waist and the hip in both groups were similar at baseline. Subjects on IQP-GC-101 demonstrated a significantly higher reduction of waist circumference and hip circumference after 12 weeks.
Control of Eating Questionnaire
The change in subject response for each of the 20 visual analog scale items was assessed separately. For all of the questions, there was no significant difference in the change of the responses from baseline to week 12 between the two groups.
Laboratory parameters
All were within the normal reference ranges used by the central laboratory. The investigators did not report any clinically relevant changes in blood chemistry in any of the study subjects. Results of laboratory parameters are detailed in Table 3.
Table 3.
Results of measurement of laboratory parameters
| Parameters | Unit | IQP-GC-101 | Placebo | pU-value | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Week 12 | Difference | Baseline | Week 12 | Difference | |||
| Hemoglobin | mmol/l | 8.65 ± 0.80 | 8.68 ± 0.81 | −0.03 ± 0.52 | 8.62 ± 0.70 | 8.65 ± 0.67 | −0.03 ± 0.82 | 0.964 |
| Haematocrit | l/l | 0.42 ± 0.03 | 0.43 ± 0.03 | −0.001 ± 0.028 | 0.43 ± 0.03 | 0.42 ± 0.03 | 0.002 ± 0.034 | 0.554 |
| Erythrocytes | Tpt/l | 4.63 ± 0.34 | 4.67 ± 0.32 | −0.04 ± 0.27 | 4.67 ± 0.39 | 4.66 ± 0.37 | 0.01 ± 0.34 | 0.942 |
| Platelets | Gpt/l | 264.2 ± 52.1 | 268.0 ± 50.7 | −3.8 ± 56.5 | 255.1 ± 61.6 | 251.8 ± 51.2 | 3.3 ± 63.7 | 0.834 |
| Leukocytes | Gpt/l | 6.84 ± 1.51 | 7.00 ± 1.83 | −0.16 ± 1.88 | 6.57 ± 2.10 | 6.55 ± 2.18 | 0.02 ± 1.65 | 0.774 |
| Alanine transaminase | µkat/l | 0.44 ± 0.23 | 0.47 ± 0.21 | −0.03 ± 0.15 | 0.52 ± 0.32 | 0.49 ± 0.25 | 0.03 ± 0.34 | 0.074 |
| Aspartate amino transferase | µkat/l | 0.40 ± 0.12 | 0.42 ± 0.10 | −0.02 ± 0.10 | 0.42 ± 0.15 | 0.43 ± 0.16 | −0.01 ± 0.18 | 0.246 |
| Alkaline phosphatase | µkat/l | 1.23 ± 0.33 | 1.26 ± 0.29 | −0.03 ± 0.23 | 1.23 ± 0.41 | 1.21 ± 0.39 | 0.02 ± 0.33 | 0.771 |
| Gamma-glutamyl transferase | µkat/l | 0.48 ± 0.30 | 0.46 ± 0.24 | 0.02 ± 0.16 | 0.51 ± 0.31 | 0.51 ± 0.44 | 0.00 ± 0.37 | 0.741 |
| Bilirubin | µmol/l | 10.8 ± 5.0 | 10.7 ± 4.7 | 0.08 ± 4.63 | 11.8 ± 5.7 | 13.1 ± 9.7 | −1.29 ± 8.59 | 0.608 |
| Creatinine | µmol/l | 70.3 ± 13.4 | 72.4 ± 13.5 | −2.15 ± 12.50 | 68.7 ± 11.2 | 71.1 ± 11.6 | −2.33 ± 11.14 | 0.508 |
| Urea | mmol/l | 4.81 ± 1.16 | 4.58 ± 1.30 | 0.23 ± 1.46 | 4.82 ± 1.17 | 4.82 ± 1.65 | 0.00 ± 1.67 | 0.317 |
| Sodium | mmol/l | 138.7 ± 1.8 | 139.3 ± 2.2 | −0.59 ± 2.31 | 138.9 ± 2.2 | 139.1 ± 3.5 | −0.27 ± 3.27 | 0.330 |
| Potassium | mmol/l | 4.31 ± 0.41 | 4.33 ± 0.38 | −0.02 ± 0.44 | 4.31 ± 0.43 | 4.30 ± 0.34 | 0.01 ± 0.40 | 0.628 |
| Glucose | mmol/l | 4.90 ± 0.51 | 4.94 ± 0.65 | −0.04 ± 0.74 | 4.78 ± 0.63 | 4.67 ± 0.84 | 0.10 ± 0.81 | 0.534 |
| Cholesterol | mmol/l | 5.84 ± 1.03 | 5.78 ± 0.91 | 0.07 ± 0.88 | 6.09 ± 1.03 | 5.92 ± 1.06 | 0.17 ± 0.86 | 0.790 |
| Low-density lipoprotein | mmol/l | 3.79 ± 0.78 | 3.81 ± 0.71 | −0.02 ± 0.65 | 3.92 ± 0.86 | 3.89 ± 0.78 | 0.02 ± 0.76 | 0.941 |
| High-density lipoprotein | mmol/l | 1.48 ± 0.40 | 1.48 ± 0.43 | 0.00 ± 0.36 | 1.52 ± 0.39 | 1.51 ± 0.38 | 0.01 ± 0.33 | 0.997 |
| Triglycerides | mmol/l | 1.72 ± 1.22 | 1.71 ± 1.04 | 0.01 ± 0.78 | 1.65 ± 1.27 | 1.68 ± 1.54 | −0.03 ± 1.07 | 0.841 |
Adverse events
No serious adverse events (AEs) were reported. Nine AEs were reported by subjects from the IQP-GC-101 group, and four AEs were from the placebo group; there was no significant difference in the frequency of AEs reported between the two groups (pchi = 0.117). All of the AEs were rated as ‘mild’ or ‘moderate’ in severity by the investigators and were considered unrelated to the consumption of the study products (Table 4).
Table 4.
Adverse events
| Subject No. | Group | Description of adverse effect | Severity |
|---|---|---|---|
| 36 | IQP-GC-101 | Cystitis | Moderate |
| 47 | Placebo | Infection of upper respiratory tract | Mild |
| 49 | IQP-GC-101 | Toothache | Moderate |
| 63 | IQP-GC-101 | Diarrhea | Mild |
| Infection of upper respiratory tract | Mild | ||
| 64 | IQP-GC-101 | Bilateral heel spurs | Moderate |
| 67 | Placebo | Gastrointestinal infection | Moderate |
| Bronchitis | Moderate | ||
| 68 | IQP-GC-101 | Second degree burn, back of right hand | Mild |
| 70 | IQP-GC-101 | Infection of upper respiratory tract | Mild |
| 74 | Placebo | Laryngopharyngitis, chronic bronchitis with leukocytosis | Mild |
| 76 | IQP-GC-101 | Bronchitis | Mild |
| 83 | IQP-GC-101 | Infection of upper respiratory tract | Mild |
DISCUSSION
IQP-GC-101 is a unique and proprietary blend of four herbal extracts. While all the individual extracts have been evaluated in individual studies, to our knowledge, this is the first time that such a combination has been tested in a clinical investigation on Caucasian subjects, under controlled conditions. Besides adhering to the standards of ICH-GCP, the study design took into account the guidance of the European Food Safety Authority that recommended that evidence of weight loss effects should be provided with the consumption of a food supplement over a minimum period of 12 weeks (European Food Safety Authority Panel on Dietetic products, Nutrition and Allergies, 2012).
In the current study, all subjects adhered to a slightly hypocaloric diet, and they were therefore expected to experience a degree of weight loss regardless of the treatment group allocated. Subjects on IQP-GC-101 lost significantly more body weight (2.26 ± 2.37 kg vs. 0.56 ± 2.34 kg) and body fat mass (1.12 ± 1.84 kg vs. gain of 0.37 ± 2.14 kg) compared with subjects on placebo by the end of the study. The difference in mean weight loss between the treatment and placebo arms in the current study is comparable with those reported by Bloch et al. (2003) (weight loss of 3.7 kg vs. 2 kg; active vs. placebo) in a 12-week study with high dose orlistat (360 mg/day), and by Anderson et al. (2006) (weight loss of 3.05 kg vs. 1.90 kg) in a 16-week study with low dose orlistat (180 mg/day). Additionally, the difference in mean weight loss observed in the current study is higher than the net mean effect of 0.88 kg reported in a meta-analysis of randomized controlled trials of G. cambogia extracts with daily dose of HCA ranging from 1.0 to 2.8 g (Onakpoya et al., 2011a). Thus, the current study indicated that the use of herbal extracts combination in IQP-GC-101 results in better weight loss effect in comparison to products containing only G. cambogia extract used in the other studies.
However, it is observed that the weight loss effect was less than the magnitude expected from the energy deficit diet. A possible explanation may be that the adherence to the given diet plan could have been questionable. This probably mimics real-life situation where adherence to energy restriction is often found to be difficult. On the other hand, the low rate of weight loss and the increase in the mean body fat mass in the placebo group after 12 weeks may be explained by a model where the energy homeostasis system is postulated to be more resistant to body weight loss than it is to weight gain; in case of negative energy balance, anabolic pathways (stimulation of food intake and reduction of metabolism) are activated, and catabolic pathways (inhibition of food intake and increase of metabolism) are suppressed (Schwartz et al., 2003). In the context of this study, both groups lost weight initially due to the lower daily calories consumed. After 4 weeks, as the homeostasis systems of the subjects in the placebo arm were responding to the reduction in body weight, dietary fat was stored. The same effect was however not observed in the IQP-GC-101 group; this is a possible indicator that IQP-GC-101 works by reducing lipogenesis, promoting fat oxidation and thermogenesis, the mechanism of actions reported in previous studies of the individual herbal extracts such as garcinia (Sullivan et al., 1977), green tea (Dulloo et al., 1999), and green coffee (Shimoda et al., 2006).
The study also assessed responder rates, looking into the percentage of subjects who lost at least 5% of their baseline weight, and, due to the relatively short duration of the trial, subjects who lost at least 3% of their baseline weight. There was no significant difference in the proportion of subjects who lost at least 5% of baseline weight (11 out of 46 subjects [23.9%] for IQP-GC-101 vs. five out of 45 subjects [11.1%] for the placebo group, pchi = 0.184), but there was a significant difference in the proportion of subjects who lost at least 3% of their baseline weight (24 out of 46 subjects [52.2%] for IQP-GC-101 vs. eight out of 45 subjects [17.8%] for placebo, pchi = 0.001). A longer study may be able to ascertain if the weight reduction rate can be sustained to reach clinically significant levels.
The lack of significance in the changes of responses to the COEQ scales was not unexpected, as the weight loss mechanism of IQP-GC-101 was not predicted to be through the enhancement of satiety or the reduction of cravings and appetite. Moreover, the effect on appetite and satiety could not be adequately quantified and compared due to study limitation.
One shortcoming worth noting in the current study is that subjects with regular caffeine intake were not excluded. While the present study was conducted to examine the effect of IQP-GC-101 on Caucasian subjects, it is suggested that the interaction of two factors, habitual caffeine intake and ethnicity, may impact the effect of green tea catechins-caffeine on body weight regulation. A systematic review of green tea in weight loss showed that Caucasians having a higher coffee intake tended to tolerate the effect of caffeine and thus showed a lower weight loss in response to treatment with EGCG and coffee, compared with Asians with low coffee intake (Hursel et al., 2009). Likewise, while all subjects were committed to adhere to a slightly hypocaloric diet with 30% of energy coming from fat, strict control of daily dietary calories intake was not implemented, and impact of deviations from daily recommended dietary calories intake was not quantified. Nonetheless, the weight loss effect is encouraging and hence, it is reasonable to infer the efficacy of IQP-GC-101 in a non-controlled, real-life setting.
It should also be noted that the results of this study refer specifically to the blend of all four extracts, in the specified concentrations, and thus the weight loss efficacy cannot be generalized to the individual ingredients.
With regards to safety, there have been some concerns on the effect of HCA on liver functions due to the warning imposed by FDA, and the recall of Hydroxycut products (US FDA, accessed 2013). Alanine transaminase, aspartate aminotransferase, alkaline phosphatase, gamma-glutamyl transpeptidase, and bilirubin levels were measured in this study and no clinically relevant or statistically significant changes to any of the parameters was detected from screening until the end of the study.
In conclusion, IQP-GC-101, in combination with a slightly hypocaloric diet, significantly reduced body weight and body fat mass, with a favorable safety profile. Further investigations to determine the longer-term weight management benefits of IQP-GC-101 may add to the knowledge of its use in the treatment overweight and obesity.
Acknowledgments
The authors would like to thank Professor Andrew Hill of the University of Leeds; Regina Busch, MD; and Dr Norman Bitterlich for their invaluable assistance and advice. InQpharm Europe Ltd is the sponsor of this study.
Conflict of Interest
Pee-Win Chong and Zhi-Ming Beah are employees of InQpharm Europe Ltd, the sponsor of this study, and were involved in the study design, oversight, and the drafting of the manuscript. Barbara Grube, MD was the principal investigator of the study. Linda Riede is an employee of analyze and realize GmbH and was the project manager for this trial.
REFERENCES
- Acheson KJ, Zahorska-Markiewicz B, Pittet P, Anantharaman K, Jequier E. Caffeine and coffee: their influence on metabolic rate and substrate utilization in normal weight and obese individuals. Am J Clin Nutr. 1980;33(5):989–997. doi: 10.1093/ajcn/33.5.989. [DOI] [PubMed] [Google Scholar]
- Anderson JW, Schwartz SM, Hauptman J, et al. Low-dose Orlistat effects on body weight of mildly to moderately overweight individuals: a 16 week, double-bind, placebo-controlled trial. Ann Pharmacother. 2006;40:1717–1723. doi: 10.1345/aph.1H234. [DOI] [PubMed] [Google Scholar]
- Bloch KV, Salles GF, Muxfeldt ES, Nogueira AR. Orlistat in hypertensive overweight/ obese patients: results of a randomized clinical trial. J Hypertens. 2003;21:2159–2165. doi: 10.1097/00004872-200311000-00026. [DOI] [PubMed] [Google Scholar]
- Chuah LO, Yeap SK, Ho WY, Beh BK, Alitheen NB. In vitro and in vivo toxicity of garcinia or hydroxycitric acid: a review. Evid Base Compl Alternative Med. 2012 doi: 10.1155/2012/197920. DOI: 10.1155/2012/197920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deocaris CC, Aguinaldo RR, dela Ysla JL, Asencion AS, Mojica ERE. Hypoglycemic activity of irradiated Banaba (Lagerstroemia speciosa Linn.) leaves. J Appl Sci Res. 2005;1(1):95–98. [Google Scholar]
- Dulloo AG, Duret C, Rohrer D, et al. Efficacy of a green tea extract rich in catechin polyphenols and caffeine in increasing 24-h energy expenditure and fat oxidation in humans. Am J Clin Nutr. 1999;70(6):1040–1045. doi: 10.1093/ajcn/70.6.1040. [DOI] [PubMed] [Google Scholar]
- EFSA Panel on Dietetic products, Nutrition and Allergies (NDA) Guidance on the scientific requirements for health claims related to appetite ratings, weight management, and blood glucose concentrations. EFSA J. 2012;10:2604. (11 pp) [Google Scholar]
- Fayh APT, Lopes AL, Vargas da Silva AM, Reischak-Oliviera A, Friedman R. Effects of 5% weight loss through diet or diet plus exercise on cardiovascular parameters of obese: a randomized controlled trial. Eur J Nutr. 2013;52:1443–1450. doi: 10.1007/s00394-012-0450-1. [DOI] [PubMed] [Google Scholar]
- Greenway FL, Fujioka K, Plodkowski RA, et al. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2010;376:595–605. doi: 10.1016/S0140-6736(10)60888-4. [DOI] [PubMed] [Google Scholar]
- Hamman RF, Wing RR, Edelstein SL, et al. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care. 2006;29(9):2102–2107. doi: 10.2337/dc06-0560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayamizu K, Ishii Y, Shigematsu N, et al. Safety of Garcinia cambogia extract in healthy men: high doses administration study I. J Oleo Sci. 2003;52(9):499–504. [Google Scholar]
- Heymsfield SB, Allison DB, Vasselli JR, Pietrobelli A, Greenfield D, Nunez C. Garcinia cambogia (Hydroxycitric acid) as a potential antiobesity agent. JAMA. 1998;280(18):1596–1600. doi: 10.1001/jama.280.18.1596. [DOI] [PubMed] [Google Scholar]
- Hursel R, Viechtbauer W, Westerterp-Plantenga MS. The effects of green tea on weight loss and weight maintenance: a meta-analysis. Int J Obes (Lond) 2009;33(9):956–961. doi: 10.1038/ijo.2009.135. [DOI] [PubMed] [Google Scholar]
- Jayaprakasha GK, Sakariah KK. Determination of organic acids in Garcinia cambogia (Desr.) by high-performance liquid chromatography. J Chromatogr A. 1998;806(2):337–339. [Google Scholar]
- Klein G, Kim J, Himmeldirk K, Cao Y, Chen X. Antidiabetes and anti-obesity activity of Lagerstroemia speciosa. Evid Base Compl Alternative Med. 2007;4(4):401–407. doi: 10.1093/ecam/nem013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kopelman P. Health risks associated with overweight and obesity. Obes Rev. 2007;8(Supplement 1):13–17. doi: 10.1111/j.1467-789X.2007.00311.x. [DOI] [PubMed] [Google Scholar]
- Liu S, Kim J, Li Y, Liu X, Li J, Chen X. An extract of Lagerstroemia speciosa L. has insulin-like glucose uptake–stimulatory and adipocyte differentiation–inhibitory activities in 3T3-L1 cells. J Nutr. 2001;131(9):2242–2247. doi: 10.1093/jn/131.9.2242. [DOI] [PubMed] [Google Scholar]
- Martin FW, Campbell CW, Ruberte RM. Perennial edible fruits of the tropics: an inventory. Washington, DC: United States Department of Agriculture, Agricultural Research Service; 1987. , p. 212. [Google Scholar]
- Mattes RD, Bormann L. Effects of (−)-Hydroxycitric acid on appetitive variables. Physiol Behav. 2000;71(1–2):87–94. doi: 10.1016/s0031-9384(00)00321-8. [DOI] [PubMed] [Google Scholar]
- Ohia SE, Opere CA, LeDay AM, Bagchi M, Bagchi D, Stohs SJ. Safety and mechanism of appetite suppression by a novel hydroxycitric acid extract (HCA-SX) Mol Cell Biochem. 2002;238(1–2):89–103. doi: 10.1023/a:1019911205672. [DOI] [PubMed] [Google Scholar]
- Onakpoya I, Hung SK, Perry R, Wider B, Ernst E. The use of Garcinia extract (hydroxycitric acid) as a weight loss supplement: a systematic review and meta-analysis of randomized clinical trials. J Obes. 2011a doi: 10.1155/2011/509038. DOI: 10.1155/2011/509038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Onakpoya I, Terry R, Ernst E. The use of green coffee extract as a weight loss supplement: a systematic review and meta-analysis of randomized clinical trials. Gastroenterol Res Pract. 2011b doi: 10.1155/2011/382852. DOI: 10.1155/2011/382852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Razak F, Anand S, Vuksan V, et al. Ethnic differences in the relationships between obesity and glucose-metabolic abnormalities: a cross-sectional population based study. Int J Obes (Lond) 2005;29:656–667. doi: 10.1038/sj.ijo.0802937. [DOI] [PubMed] [Google Scholar]
- Satomi T, Seigo K, Masaki M, Haruki M. An inhibitory effect on the increase in the postprandial blood glucose by Banaba extract capsule enriched corosolic acid. J Integr Study Dietary Habits. 2006;17(3):255–259. [Google Scholar]
- Schwartz MW, Woods SC, Seeley RJ, Barsh GS, Baskin DG, Leibel RL. Is the energy homeostasis system inherently biased toward weight gain? Diabetes. 2003;52(2):232–238. doi: 10.2337/diabetes.52.2.232. [DOI] [PubMed] [Google Scholar]
- Shimoda H, Seki E, Aitani M. Inhibitory effect of green coffee bean extract on fat accumulation and body weight gain in mice. BMC Complement Altern Med. 2006;6:9. doi: 10.1186/1472-6882-6-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stobs SJ, Miller H, Kaats GR. A review of the efficacy and safety of banaba (Lagerstroemia speciosa L.) and corosolic acid. Phytother Res. 2012;26:317–324. doi: 10.1002/ptr.3664. [DOI] [PubMed] [Google Scholar]
- Sullivan AC, Triscari J, Hamilton JG, Miller ON, Wheatley VR. Effect of (−)-Hydroxycitrate upon the accumulation of lipid in the rat II: appetite. Lipids. 1974;9(2):129–134. doi: 10.1007/BF02532137. [DOI] [PubMed] [Google Scholar]
- Sullivan AC, Singh M, Srere PA, Glusker JP. Reactivity and inhibitor potential of hydroxycitrate isomers with citrate synthase, citrate lyase and ATP citrate lyase. J Biol Chem. 1977;252(21):7583–7590. [PubMed] [Google Scholar]
- U.S. Food and Drug Administration. Warning on Hydroxycut products http://www.fda.gov/forconsumers/consumerupdates/ucm152152.htm [Accessed 20 August 2013]