

Abstract
Writing about a personal stressful event has been found to have psychological and physical health benefits, especially when physiological response increases during writing. Response training was developed to amplify appropriate physiological reactivity in imagery exposure. The present study examined whether response training enhances the benefits of written emotional disclosure. Participants were assigned to either a written emotional disclosure condition (n = 113) or a neutral writing condition (n = 133). Participants in each condition wrote for 20 minutes on three occasions and received response training (n = 79), stimulus training (n = 84) or no training (n = 83). Heart rate and skin conductance were recorded throughout a 10-minute baseline, 20-minute writing, and a 10-minute recovery period. Self-reported emotion was assessed in each session. One month after completing the sessions, participants completed follow-up assessments of psychological and physical health outcomes. Emotional disclosure elicited greater physiological reactivity and self-reported emotion than neutral writing. Response training amplified physiological reactivity to emotional disclosure. Greater heart rate during emotional disclosure was associated with the greatest reductions in event-related distress, depression, and physical illness symptoms at follow-up, especially among response trained participants. Results support an exposure explanation of emotional disclosure effects and are the first to demonstrate that response training facilitates emotional processing and may be a beneficial adjunct to written emotional disclosure.
Keywords: written emotional disclosure, expressive writing, emotional processing, heart rate, skin conductance, response training
Enhancing the Benefits of Written Emotional Disclosure through Response Training More than two decades of research indicates that disclosure of stressful experiences through writing has far-reaching physical and mental health benefits (Pennebaker & Beall, 1986; Frattaroli, 2006; Boals, 2012). Writing's efficacy, efficiency (writing typically takes place in three to seven 15-20 minute sessions), and cost-effectiveness suggest that writing as a medium for disclosing stressful events may be a useful therapeutic technique. Early studies showing the benefits of written emotional disclosure have led it to be used as a component in some treatments for PTSD including Cognitive Processing Therapy (Resick et al., 2008), and to be evaluated as a standalone treatment for posttraumatic stress (van Emmerik, Reijntjes, & Kamphuis, 2013). Other recent writing research found significant improvements in psychological and physical health at follow-up compared to baseline for emotional disclosure and neutral writers with no significant group differences observed (Kearns, Edwards, Calhoun, & Gidycz, 2010; Daniels, 2009; Smyth, Hockemeyer, & Tulloch, 2008). Thus, while preliminary research suggests that written emotional disclosure is a form of exposure (Epstein, Sloan, & Marx, 2005; Sloan & Marx, 2004b; Sloan, Marx, Epstein & Lexington, 2007) more empirical research is required to investigate this assumption to broaden writing's clinical utility and clarify when and for whom writing may be beneficial.
The bio-informational theory of emotion (Lang, 1979) may help to elucidate the mechanism by which emotional writing is effective, and thus how its clinical utility may be improved. From the perspective of bio-informational theory, emotional imagery and written emotional disclosure are both media through which emotional memory networks can be accessed. An emotional memory network is comprised of mutually-connected information units, including descriptive, meaning, and response units, with activation of response units resulting in measurable efferent activity (Lang, 1979). While descriptive and meaning units are typically easily accessed, individuals often have difficulty accessing response units, as evidenced by low physiological reactivity during emotional imagery (Lang, Levin, Miller, & Kozak, 1983). For complete emotional processing to occur, all three types of units (descriptive, meaning, and response) must be fully activated (Foa & Kozak, 1986; Lang, et al., 1983). As the theory predicts, people with lower physiological reactivity during exposure therapy have poorer treatment outcomes than people with relatively high physiological reactivity, which reflects response unit activation (Beckham, Vrana, May, Gustafson, & Smith, 1990; Foa & Kozak, 1986; Lang, Melamed, & Hart, 1970; Watson & Marks, 1971). Craske et al. (2008) point out that this effect has been primarily restricted to heart rate reactivity during initial exposure, and has not been found with either skin conductance or self-reported fear. Craske et al. further posit other mechanisms involved in fear reduction, including toleration of fear and facilitating inhibitory learning, processes that also involve initial activation of the fear memory.
The positive association between greater physiological responding during exposure and better therapeutic outcomes has also been found in written emotional disclosure (Sloan et al., 2004b; Epstein et al., 2005; Sloan, Marks, & Epstein, 2005), suggesting that both techniques serve as media through which memory networks are activated and processed. Epstein et al. (2005) found, among college students not pre-screened for prior trauma experience or posttraumatic symptoms, greater initial heart rate reactivity to writing about an emotional topic than to writing about a neutral topic. Among those in the emotional disclosure condition, greater heart rate reactivity in the first writing session was associated with reduced depression and self-reported symptoms of physical illness one month after writing. In another study (Sloan et al., 2007), college students with at least moderate levels of post-traumatic stress symptoms were randomly assigned to write about either a neutral topic or a personal trauma in one of two conditions: with as much emotional expression as possible, or with a focus on what the event meant to them. Participants in the emotional expression condition evidenced greater HR reactivity to the first session, and greater reductions in post-traumatic stress symptoms, depressive symptoms and physical health symptoms one month post-writing, than in the neutral topic or event meaning writing condition. Other studies (Sloan & Marx, 2004b; Sloan et al., 2005) employing female college students with at least moderate post-traumatic stress symptoms found greater initial cortisol reactivity in response to emotional disclosure in the first writing session was associated with reduced PTSD symptom severity and depressive symptoms (Sloan et al., 2004b) at one and two months post writing. Case studies have confirmed these findings in patients with moderate levels of PTSD symptoms (Sloan & Marx, 2006). Thus, if a method could be found to increase physiological responding to written emotional disclosure, it may be possible to produce better therapeutic outcomes.
Given the importance of physiological output in emotional processing, Lang and his colleagues (1980) developed a brief response training program to increase efferent output during emotional imagery by amplifying pre-existing response dispositions. Compared to stimulus training (which focuses imagery on sensory experiences), response training amplifies situation-appropriate heart rate to fear and action imagery (Lang et al., 1980) and increases heart rate to imagery of one's own fear situations, but not to another group's fear (Lang et al., 1983). Similarly, when participants imagine personally-relevant scenes (as opposed to scenes created by the experimenters), response training amplifies efferent output, especially for people with poor imagery ability (Miller et al., 1987). These findings, taken together, indicate that response training does not impose physiological responses on individuals or create a demand effect, but rather facilitates access of already-present perceptual-motor memory networks (Lang, 1984).
According to Lang (1984), the key to activating an emotional memory network is for the eliciting stimulus to match the propositional units in the network, and thus response training would be predicted to have the same enhancing effect on physiological responding regardless of the input medium. Since writing about a personally-traumatic event, like imagery processing, serves to access memory networks as evidenced by physiological responding (Sloan et al., 2004b; Epstein et al., 2005; Sloan et al., 2005), it is reasonable to expect that response training will amplify physiological response found when writing these scenes. Further, if efferent output is amplified, the beneficial effects of writing would be expected to increase.
Current thinking is that emotion and behavior is conceived on a dimension from normal to abnormal (NIMH, 2011). About 60% of a population-based representative sample of Americans report experiencing at least one significant adverse childhood event (verbal, physical, or sexual abuse; mentally-ill or substance-abusing household member, etc.) (CDC, 2010), and by college up to 84% report experiencing at least one traumatic event (Vrana & Lauterbach, 1994). Negative physical and mental health consequences are associated with experiencing just one event and increase with additional negative experiences (Felitti et al., 1998). Writing about an emotional topic in an expressive way has produced positive physical and mental health outcomes for people with PTSD (Sloane & Marx, 2006) and for college students without notable traumatic histories (Sloane & Marx, 2004a). Thus, emotionally writing about personal events, from truly traumatic to merely distressing, may have broadly applicable benefits.
The goal of the current project is to examine whether response training enhances physiological response in college students not screened for trauma exposure when writing about their most distressing experience, and whether this improves outcomes of writing. Hypotheses are: 1) Written emotional disclosure will increase heart rate (HR), skin conductance (SC), self-reported unpleasantness and arousal compared to neutral writing; 2) Response training will increase HR and SC more than other training conditions during written emotional disclosure but not neutral writing; 3) Written emotional disclosure will reduce event-related distress, depression, and physical illness symptoms more than neutral writing; 4) Greater HR and SC in response to writing about an emotional topic in the first session will be associated with greater improvement in event-related distress, depression, and physical illness symptoms; and 5) Response training will enhance emotional processing, thus the relationship between physiological reactivity and health outcomes in written emotional disclosure proposed in hypothesis 4 will be even stronger in response trained participants.
Method
Design
Participants were randomly assigned to one of six groups, with three training conditions (response training, stimulus training, no training) crossed with two writing conditions (emotional disclosure, neutral writing). All participants wrote for three 20-minute sessions each separated by at least a day and spread over no more than two weeks, and then were mailed a follow-up questionnaire packet one month after their third writing session.
Participants
Participants were 246 college students 18 years of age or older from a large, urban university Department of Psychology research pool who were not screened to confirm trauma exposure. As can be seen in Table 1, participants were mostly women in their early twenties, college freshmen or sophomores, generally identified English as their first language, and were ethnically diverse. Approval for the study was obtained from the university's Institutional Review Board. Participants were compensated with course credit, as is typical in written emotional disclosure studies (Kloss & Lisman 2002; Smyth, True & Souto, 2001.
Table 1. Demographic information.
| Variable | Response Trained Emotional Disclosure N (%) or M (SD) | Stimulus Trained Emotional Disclosure N (%) or M (SD) | No Training Emotional Disclosure N (%) or M (SD) | Response Trained Neutral N (%) or M (SD) | Stimulus Trained Neutral N (%) or M (SD) | No Training Neutral N (%) or M (SD) | Total Sample N (%) or M (SD) |
|---|---|---|---|---|---|---|---|
| Age | 20.9 (4.2) | 20.9 (2.8) | 23.9 (9.8) | 20.8 (4.3) | 21.1 (4.7) | 21.4 (4.0) | 21.5 (5.5) |
| (Range 18-37) | (Range 18-28) | (Range 18-53) | (Range 18-26) | (Range 18-43) | (Range 18-35) | (Range: 18-53) | |
| Gender | |||||||
| Male | 9 (22.5%) | 9 (25.7%) | 10 (26.3%) | 10 (25.6%) | 10 (20.4%) | 21 (46.7%) | 69 (28%) |
| Female | 31 (77.5%) | 26 (74.3%) | 28 (73.7%) | 29 (74.4%) | 39 (79.6%) | 24 (53.3%) | 177 (72%) |
| Race | |||||||
| White | 23 (57.5%) | 16 (45.7%) | 19 (50.0%) | 23 (59.0%) | 19 (38.8%) | 18 (40.0%) | 118 (48%) |
| Black/African American | 8 (20.0%) | 11 (31.4%) | 8 (21.1%) | 7 (17.9%) | 19 (38.8%) | 16 (35.6%) | 69 (28%) |
| Asian | 4 (10.0%) | 4 (11.4%) | 2 (5.3%) | 6 (15.4%) | 5 (10.2%) | 6 (13.3%) | 27 (11%) |
| Hispanic | 1 (2.5%) | 1 (2.9%) | 1 (2.6%) | 1 (2.6%) | 0 (0.0%) | 1 (2.2%) | 5 (2%) |
| Native Hawaiian or Other Pacific Islander | 1 (2.5%) | 0 (0.0%) | 1 (2.6%) | 0 (0.0%) | 0 (0.0%) | 1 (2.2%) | 3 (1.2%) |
| Other | 3 (7.5%) | 3 (8.6%) | 7 (18.4%) | 2 (5.1%) | 6 (12.2%) | 3 (6.7%) | 24 (9.8%) |
| Year in School | |||||||
| Freshman | 14 (35.0%) | 9 (25.7%) | 12 (31.6%) | 15 (38.5%) | 19 (38.8%) | 23 (51.1%) | 92 (37.4%) |
| Sophomore | 13 (32.5%) | 7 (20.0%) | 8 (21.1%) | 9 (23.1%) | 6 (12.2%) | 7 (15.6%) | 50 (20.3%) |
| Junior | 8 (20.0%) | 7 (20.0%) | 5 (13.2%) | 5 (12.8%) | 9 (18.4%) | 7 (15.6%) | 41 (16.7%) |
| Senior | 5 (12.5%) | 12 (34.3%) | 13 (34.2%) | 10 (25.6%) | 15 (30.6%) | 8 (17.8%) | 63 (25.6%) |
| Native Language | |||||||
| English | 35 (87.5%) | 32 (91.4%) | 27 (71.1%) | 35 (89.7%) | 45 (91.8%) | 37 (82.2%) | 211 (85.8%) |
| Other | 5 (12.5%) | 3 (8.6%) | 11 (28, 9%) | 4 (10.3%) | 4 (8.2%) | 8 (17.8%) | 35 (14.2%) |
Apparatus and Materials
Physiological assessment
Physiological responses were assessed at writing sessions one and three. HR was selected because cardiovascular changes have been found to be common and detectable measures of changes in psychological and arousal states in similar studies (Sloan et al., 2007; Epstein et al., 2005). Only one study has compared the effect of trauma and neutral writing on SC (Petrie et al., 1995) and found that written emotional disclosure increased initial SC more than neutral writing. Thus, SC was included in the current study to further assess the effects of writing on SC. The electrocardiograph (EKG) signal was obtained using sensors attached immediately below the participants' right clavicle and lowest left rib. A ground electrode was attached on the participant's forearm. The EKG signal was amplified and filtered by a Coulbourn S75-01 Hi Gain Bioamplifier. The R-wave triggered a digital input on the computer, which recorded the interbeat interval with millisecond resolution. Interbeat intervals were converted off-line to heart rate in beats/minute. Skin Conductance (SC) was recorded using a Coulbourn S71 - 22 Skin Conductance Coupler that applied a constant .5 V across two standard Ag-AgCl electrodes. Electrodes filled with K-Y jelly were attached after participants washed their hands with tap water. Pilot work was conducted to determine an appropriate electrode location that would not be influenced by the physical movement of writing. On the non-dominant hand, one electrode was attached between the base of the index and middle finger and the other was placed on the outer base of the palm. SC was sampled at 10 Hz with a 12-bit analog-digital converter and converted off-line to μmhos. Heart rate and skin conductance were recorded continuously for a 10-minute baseline period prior to writing, during the 20-minute writing session, and for a 10-minute post-writing recovery period.
Self-report measures
Participants completed measures of distress related to their most distressing lifetime event, depression, and physical illness symptoms at baseline and one month after the third writing session. To evaluate post-event distress, participants completed the Davidson Trauma Scale (DTS; (Davidson et al., 1997), in which the individual was asked to identify a distressing/ traumatic experience that was most disturbing to him/her and to complete the 17-item scale assessing DSM-IV PTSD symptoms experienced in the last week related to the identified event. On the DTS, symptom severity is rated from 0 (not at all distressing) to 4 (extremely distressing). The internal reliability and the two-week test-retest reliability of the DTS are 0.99 and 0.86, respectively. The Center for Epidemiological Studies-Depression Scale (CES-D), is a 20-item self-report of depression symptoms over the past week (Radloff, 1977). Scores below 15, 16-20, and 21-30 indicate no, mild, and moderate depression, respectively. The CESD scale has satisfactory levels of sensitivity and specificity for a college-student cohort using standard cutpoints (Shean & Baldwin, 2008). The CES-D has high internal consistency (.85) and moderate test-retest reliability. The Pennebaker Inventory of Limbic Languidness (PILL; Pennebaker, 1982) is a 54-item scale that assesses common physical symptoms and sensations on a 5-point scale from have never or almost never experienced to experience the symptom more than once every week. Normative data show a mean of 59 and standard deviation of 25. The Cronbach alpha of the PILL ranges from 0.88 to 0.91, and the two-month test-retest reliability ranges from 0.79 to 0.83. Significant correlations are found between PILL scores and the frequency of visits to the health center and physicians, health-related work absences, and aspirin use (Pennebaker, 1982).
The Self-Assessment Manikin (SAM; Bradley & Lang, 1994) assesses self-reported valence and arousal, and was used by participants before and after each writing session to rate their emotional state at that moment. A pictorial (converted to a 1-9 rating) scale was used to assess valence (unpleasantness to pleasantness) and arousal (relaxed to aroused), with nine indicating maximum pleasantness and arousal. These dimensions have been found to reliably covary with physiological reactions, suggesting that the SAM is a valid measure of emotional responding (Bradley, Greenwald, Petry & Lang, 1992).
Training Conditions
Just before the beginning of the first writing session participants in the response and stimulus training conditions took part in an individual session lasting approximately 45 minutes, following procedures outlined in previous studies (Lang et al., 1980, 1983; Miller et al., 1987). Prior to training, participants were taught diaphragmatic breathing to help them relax and stabilize baseline responding, with the instructions to “place one hand on your chest and the other on your abdomen… inhale slowly through your nose and try to make the hand on your abdomen rise… After you've taken a full breath, pause for a second, and then exhale slowly and fully through your nose or mouth and count to one to yourself as you exhale.” Four scripts (approximately 100 words each), lacking reference to emotion but containing descriptive detail and reference to behavioral and physiological responding (for response training) or containing stimulus detail (for stimulus training), were read by the trainer. After each script was read, participants were asked to imagine the script and to describe their imagery. Response training participants were systematically praised for providing imagery descriptions of active physiological and behavioral involvement, including verbal responses (“I scream”), overt motor acts (“I run away”), and responses of the physiological organs (“My heart is racing”), and instructed to “do in the image what you would do in the real situation”. Stimulus training participants were systematically praised for providing imagery descriptions focusing on sensory detail (“The sky is blue” or “The sun is shining”), and were told that “the idea of a vivid image is that you get a realistic picture of the scene in your mind”. If participants did not provide appropriate descriptions of their imagery, they were encouraged to do so for the remaining trials. The no training participants were taught diaphragmatic breathing and given ample time to adapt to the laboratory environment before psychophysiological baseline data were collected. The full response and stimulus training protocols are available from the authors upon request.
Writing Conditions
Writing instructions were adapted from instructions developed by Pennebaker (1997), with the addition that participants in the stimulus and response training conditions were instructed to “use the techniques you were taught earlier [or “in the first session”] in order to more fully involve yourself in your writing”. Emotional disclosure participants were asked to write about “the most traumatic, upsetting experience of your entire life that you identified when you filled out [the DTS] earlier” with as much emotion and feeling as possible. Though standard instructions (Pennebaker, 1997) allow individuals to write about different topics each session, greater physiological reactivity and psychological and physical health changes have been found among participants who wrote about the same experience during each writing session (Sloan et al., 2005). As such, participants were asked to write about the same experience in each writing session. Neutral writing participants were asked to write about the details of how they use their time without describing any emotion or opinions. On the first day of writing neutral writing participants wrote about “what you did yesterday from the time you got up until the time you went to bed”. On the second day, they were asked to “describe what you have done today since you woke up”. On the third day, they were asked to “describe what you will be doing over the next week”.
Procedures
Upon arrival to the first session, participants read and signed the consent form. They next completed a demographic questionnaire, the CES-D, DTS, PILL, and valence and arousal ratings. Participants then received response, stimulus, or no training. Next, electrodes were attached and participants were instructed to sit quietly and relax using the breathing technique they were taught, if they found it to be relaxing. If they did not find the technique to be relaxing, they were asked to breathe normally, focusing on their breathing and clearing their mind of all thoughts. Baseline physiological data were recorded for ten minutes, after which they were instructed to write for 20 minutes about either a personal traumatic event or a neutral topic. After writing, participants sat quietly for 10 minutes while recovery data were collected. The electrodes were then removed and valence and arousal ratings were completed. Participants were then asked to return to the lab for their next scheduled writing session. At the beginning of session two, participants again wrote for 20 minutes, though physiological data were not recorded. Session three was the same as session two, except that physiological data were once again collected. One month after writing, participants were mailed a follow-up packet including the CES-D, DTS, and the PILL.
Data Preparation and Analysis
After deleting the first two minutes of HR and SC data to reduce variability in physiology due to variable writing start times, the remaining 18 minutes of data from the 20-minute writing period were divided into three 6-minute periods (minutes 3-8, 9-14, and 15-20). SC data were log-transformed to reduce skew (Boucsein, 1992). The mean of the last five minutes of pre- writing was used as a baseline to create change scores for each of these three writing periods. In addition, change scores (one-month follow-up minus baseline) were created for post-traumatic symptom severity (DTS), depression (CES-D) and physical illness symptoms (PILL).
Because the association between treatment outcome and initial fear response is better supported than the association between outcome and within-session or between-session habituation (Craske et al., 2008), hypotheses for this study are focused on data from the first session and the 1-month follow-up data. Valence and arousal ratings were analyzed with 2 Writing Condition (emotional disclosure, neutral) × 3 Training Condition (response, stimulus, no training) × 2 Prepost (pre-writing, post writing) repeated measures ANOVAs. HR and SC change scores from session one were analyzed using 2 Writing Condition × 3 Training Condition × 3 Period (minutes 3-8, 9-14, 15-20) repeated measures ANOVAs. Hypothesis 1 predicts a main effect of writing condition in this ANOVA, with HR and SC increase greater in the emotional disclosure condition. Hypothesis 2 predicts greater HR and SC change for response training than the other training conditions, but only for the emotional disclosure writers. Because this effect may also vary across the 20-minute writing period, this hypothesis predicts a Writing Condition × Training Condition × Period (minutes 3-8, 9-14, and 15-20) interaction, with response training producing greater physiological reactivity than the other training groups at one or more periods within the writing session for emotional, but not neutral, writing. For repeated measures effects we employed a multivariate F-test not requiring an assumption of sphericity.
Change in physical illness (PILL) and trauma (DTS) symptoms were analyzed with a 2 Writing Condition × 3 Training Condition × 2 Interval (baseline, one-month follow-up) repeated measures ANOVA. Hypothesis 3 predicts a Writing Condition × interval interaction for each variable. Since depression (CES-D) scores were significantly different between writing groups at baseline, depression was analyzed with a 2 Writing Condition × 3 Training Condition univariate analysis of covariance was conducted with baseline CES-D as the covariate and CES-D scores at follow-up as the dependent variable, with a main effect of writing condition predicted.
This study also examined whether physiological responding during emotional disclosure is associated with greater improvement in mental and physical health outcomes (Hypothesis 4). Further, if response training increases the likelihood of emotional processing, then the association between physiological reactivity and health outcomes should be strongest among response-trained emotion writers (Hypothesis 5). To test these hypotheses, for emotional disclosure participants, a stepwise regression analysis was conducted regressing the follow-up minus pre-writing difference scores for each outcome measure (DTS, CES-D, and PILL) onto the following session one variables: HR and SC difference scores (mean of minutes 3-8 of writing minus mean of last five minutes of baseline), HR and SC baseline scores (mean of last five minutes of baseline), training group (response and stimulus training, each dummy-coded as 0 or 1), and the interaction of training group with each of the four physiological independent variables (HR and SC difference score; HR and SC baseline). All independent variables were mean centered. If an interaction term entered in the stepwise regression analysis (at p < .05), a simultaneous regression was conducted to include all significant interactions and main effects plus all the main effects constituting the interactions in the final model. Beta values from the simultaneous regression model are reported. The change in symptoms from baseline to one-month follow-up is predicted to be associated with HR and/or SC difference scores (Hypothesis 4) and the interaction between these difference scores and training group (Hypothesis 5).
Results
Demographics
Table 1 summarizes demographic characteristics for the entire sample and separately for each group. Only one group difference was found, as participants in the no training condition were marginally older [M = 22.68, SD = 9.34] than response [M = 20.86, SD = 9.50] and stimulus [M = 20.98, SD = 9.34] trained participants, F(2, 244) = 2.87, p = .059.
Attrition
Rates of compliance across all conditions were quite high, with the large majority of the initial 246 participants (n = 234; 95.1%) completed all three writing sessions (107 emotional disclosure participants [94.7%] and 127 neutral writing participants [95.5%]). Most (n = 194; 78.9%) of the initial participants completed all three writing sessions and the one month follow-up. For analyses that included only within writing session physiological or psychological reactivity to writing, the 234 participants who completed all three writing sessions were used. For analyses that included the follow-up measures of psychological or physical health, the 194 individuals who completed all three writing sessions and the follow-up were used.
Preliminary Data Screening
Writing Condition × Training Condition analyses were run to examine whether there were significant baseline differences between participants randomized to the six groups on measures of trauma (DTS), depression (CES-D), physical illness symptoms (PILL), and baseline HR and SC. No significant baseline difference was found for frequency of common physical symptoms (PILL). Neutral writing participants had higher baseline CES-D scores than emotional disclosure participants, Writing Condition F(1, 236) = 7.97, p = .005. Response-trained participants had marginally higher baseline DTS severity scores than participants in the stimulus condition, Training Condition F (2,235) = 3.13, p = .045. Baseline and follow-up questionnaire data are presented in Table 2. No significant HR baseline differences were found. Response-trained and no training participants had higher SC baseline scores than stimulus-trained participants, Training Condition F(2, 233) = 6.02, p = .003. See Table 3 for baseline HR and SC data. Table 4 lists the number of participants who identified different types of events as their most traumatic or stressful, categorized by adapting previously-developed classification schemes (Greenberg & Stone, 1992; Lumley & Provenzano, 2003).
Table 2. Baseline and Follow up Means (and Standard Deviations) for DTS, CES-D, and PILL.
| Emotional Disclosure | Neutral | Total | ||||
|---|---|---|---|---|---|---|
|
|
|
|
||||
| Baseline | Follow up | Baseline | Follow up | Baseline | Follow up | |
| DTS-Severity | ||||||
| Response | 19.3 (18.2) | 11.2 (13.0) | 23.3 (15.7) | 10.7 (13.2) | 21.4 (16.9) | 10.9 (13.0) |
| Stimulus | 14.3 (10.7) | 8.2 (14.3) | 18.1 (13.8) | 9.4 (11.7) | 16.4 (12.6) | 8.9 (12.8) |
| No Training | 19.6 (13.4) | 12.2 (11.3) | 18.6 (14.0) | 11.3 (12.5) | 19.1 (13.6) | 11.8 (11.8) |
| Total | 17.9 (14.4) | 10.7 (12.8) | 19.8 (14.5) | 10.4 (12.3) | 18.9 (14.4) | 10.5 (12.5) |
|
| ||||||
| CES-D | ||||||
| Response | 14.4 (9.1) | 14.4 (7.5) | 17.3 (11.2) | 16.8 (12.0) | 15.8 (10.2) | 15.6 (9.8) |
| Stimulus | 11.4 (7.2) | 11.0 (9.8) | 18.0 (11.4) | 16.2 (11.1) | 14.7 (9.3) | 13.6 (10.5) |
| No Training | 12.6 (6.4) | 14.5 (6.9) | 14.3 (8.7) | 12.8 (8.6) | 13.4 (7.6) | 13.7 (7.7) |
| Total | 12.8 (7.6) | 13.3 (8.1) | 16.5 (10.4) | 15.3 (10.6) | 14.7 (9.0) | 14.3 (9.3) |
|
| ||||||
| PILL | ||||||
| Response | 57.6 (26.9) | 54.6 (27.6) | 65.8 (24.7) | 58.0 (26.0) | 61.7 (25.9) | 56.3 (26.6) |
| Stimulus | 54.2 (23.0) | 45.7 (21.4) | 55.6 (27.3) | 51.6 (24.8) | 55.0 (25.3) | 49.1 (23.4) |
| No Training | 56.0 (26.5) | 52.0 (24.9) | 50.9 (24.0) | 45.0 (21.0) | 53.5 (25.2) | 48.5 (23.1) |
| Total | 56.0 (25.3) | 51.0 (24.8) | 57.3 (25.9) | 51.6 (24.4) | 56.7 (25.6) | 51.3 (24.5) |
DTS: Davidson Trauma Scale; CES-D: Center for Epidemiological Studies-Depression; PILL: Pennebaker Inventory of Limbic Languidness
Table 3. Baseline Heart Rate and Skin Conductance Means (and Standard Deviations).
| Emotional Disclosure | Neutral | Total | |
|---|---|---|---|
| Heart Rate (bpm) | |||
| Response Training | 81.7 (11.5) | 77.4 (11.8) | 79.7 (11.8) |
| Stimulus Training | 76.0 (11.2) | 79.2 (13.9) | 77.9 (12.9) |
| No Training | 75.2 (10.0) | 78.5 (13.6) | 76.9 (12.0) |
| Total | 77.7 (11.2) | 78.4 (13.2) | 78.1 (12.3) |
|
| |||
| Skin Conductance (μmho) | |||
| Response Training | .285 (.520) | .361 (.466) | .321 (.493) |
| Stimulus Training | .038 (.441) | .144 (.524) | .103 (.493) |
| No Training | .306 (.493) | .348 (.433) | .328 (.460) |
| Total | .218 (.498) | .271 (.486) | .247 (.491) |
Table 4. Types of Stressful Events Disclosed.
| Event Category | n | % |
|---|---|---|
| Death of loved one | 61 | 24.8 |
| Divorce/separation/conflict between parents or own divorce | 3 | 1.2 |
| Serious problems of close other | 27 | 11.0 |
| Romantic issues | 18 | 7.3 |
| Physical or sexual abuse/attack | 18 | 7.3 |
| Illness | 15 | 6.1 |
| Car accident or other accident | 17 | 6.9 |
| Problems in relationship with friends, peers or family members | 12 | 4.9 |
| Difficulty with school or job | 3 | 1.2 |
| Other (multiple) | 25 | 10.2 |
| Abortion/ pregnancy/ miscarriage | 10 | 4.1 |
| Personal problem such as self-harm, legal problems, or other personal stressful situations | 30 | 12.2 |
| Harassment or bullying | 7 | 2.9 |
Response to Writing
Effects of writing
As predicted (Hypothesis 1), pleasantness decreased from before to after emotional disclosure, but did not change as a function of neutral writing, Writing Condition × Prepost, F(1,239) = 65.39, p < .001, ή2 = .215. Emotional disclosure also increased arousal levels, whereas neutral writing decreased arousal levels, Writing Condition × Prepost F(1, 239) = 17.06, p < .001, ή2 = .067 (see Table 5.). Hypothesis 1 also predicted that emotional disclosure would increase HR and SC more than neutral writing. Emotional disclosure [M = 4.4 bpm, SD = 7.3] increased HR more than neutral writing [M = 3.7 bpm, SD = 6.9]; however, this pattern was not significant, F(1, 227) = 1.15, p = 0.29, ή2 = .005. Emotional disclosure [M = .26 μmhos, SD = 0.39] also increased SC more than neutral writing [M = .20 μmhos, SD = 0.36], however, this pattern was also not significant, F(1, 233) = 2.64, p = .11, ή2 =.011.
Table 5. Self-Assessment Manikin Valence and Arousal Means (and Standard Deviations) for Pre and Post Writing.
| Valence Pre | Valence Post | ||||
|---|---|---|---|---|---|
|
|
|||||
| Emotional Disclosure | |||||
| Response | 7.2 (1.36) | 5.5 (2.06) | |||
| Stimulus | 7.1 (1.42) | 5.5 (2.03) | |||
| No Training | 7.4 (1.24) | 5.3 (2.24) | |||
| Total | 7.3 (1.33) | 5.4 (2.10) | |||
|
| |||||
| Neutral | |||||
| Response | 6.7 (1.35) | 6.3 (1.54) | |||
| Stimulus | 6.7 (1.67) | 6.9 (1.35) | |||
| No Training | 6.9 (1.58) | 6.9 (1.37) | |||
| Total | 6.8 (1.55) | 6.7 (1.43) | |||
|
| |||||
| Arousal Pre | Arousal Post | ||||
|
|
|||||
| Emotional Disclosure | |||||
| Response | 4.1 (1.71) | 4.5 (2.10) | |||
| Stimulus | 3.7 (1.69) | 4.5 (1.97) | |||
| No Training | 3.6 (1.76) | 4.3 (2.01) | |||
| Total | 3.8 (1.73) | 4.5 (2.02) | |||
|
| |||||
| Neutral | |||||
| Response | 4.1 (1.71) | 3.3 (1.93) | |||
| Stimulus | 3.8 (1.60) | 3.7 (1.99) | |||
| No Training | 4.1 (1.76) | 3.7 (1.67) | |||
| Total | 4.0 (1.68) | 3.6 (1.86) | |||
Hypothesis 3 was that emotional disclosure would reduce severity of trauma, depression, and physical illness symptoms more than neutral writing from baseline to the one month follow-up. Participants reported a decrease in severity of trauma symptoms from baseline to follow-up, Interval F(1, 175) = 78.33, p < .001. While both emotional disclosure and neutral writing led to a reduction in severity of trauma symptoms (DTS), emotional disclosure did not reduce severity of trauma symptoms more than neutral writing from baseline to follow-up, Writing Condition × Interval F(1, 175) = 1.58, p = .210. A similar pattern was found for physical illness symptoms (PILL), Interval F(1, 177) = 17.43, p < .001, Writing Condition × Interval interaction F(1, 177) = .08, p = .78 and depression symptoms (CES-D), Writing Condition F(1, 183) = .53, p > .050.
Effects of training
Hypothesis 2 was that response training would increase HR and SC to emotional disclosure more than stimulus or no training, whereas training condition would not affect HR and SC during neutral writing. Because this effect was likely to vary across the 20-minute writing period, this hypothesis predicts a Writing Condition × Training Condition × Period interaction, with response training producing greater physiological reactivity than the other training groups at one or more periods within the writing session for emotional, but not neutral, writing. The predicted three-way interaction was borderline significant for HR, F(2, 227) = 2.76, p = .066, ή2 = .024. Follow-ups compared the response training condition against the other two conditions at each interval within the written emotion disclosure group and within the neutral writing group. Figure 1 shows that response-trained emotion writers had marginally greater HR increase at minutes 3-8 (p = .083), and significantly greater HR reactivity at minutes 15-20 (p = .037) than no training participants. Response trained neutral writers did not differ in HR from the other training conditions at any point in the writing interval. The hypothesized three-way interaction was not found for SC reactivity, p > .10. Training condition also did not affect self-reported levels of unpleasantness and arousal, Writing Condition × Training Condition × Prepost interaction for unpleasantness or arousal, both p > .20.
Figure 1.
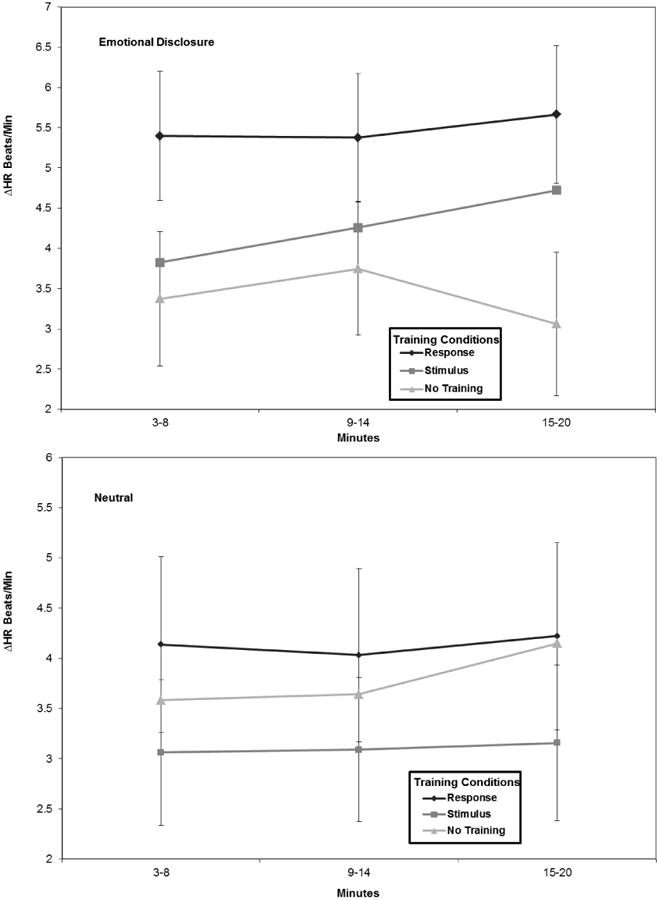
HR presented for the Writing Condition × Training Condition × Period Interaction. Vertical lines represent standard error (SE) bars. SE bars are not included for the middle group to increase clarity of the figure, but are comparable to that of the other conditions.
Predicting Health Outcome from Response to Writing
Hypothesis 4 was that HR and SC during emotional disclosure would be associated with greater improvement in trauma, depression and physical illness symptoms at follow-up. Hypothesis 5 was that, if response training increased the likelihood of emotional processing, then the association between physiological reactivity and health outcomes would be strongest among response-trained emotion writers.
Trauma symptom severity (DTS)
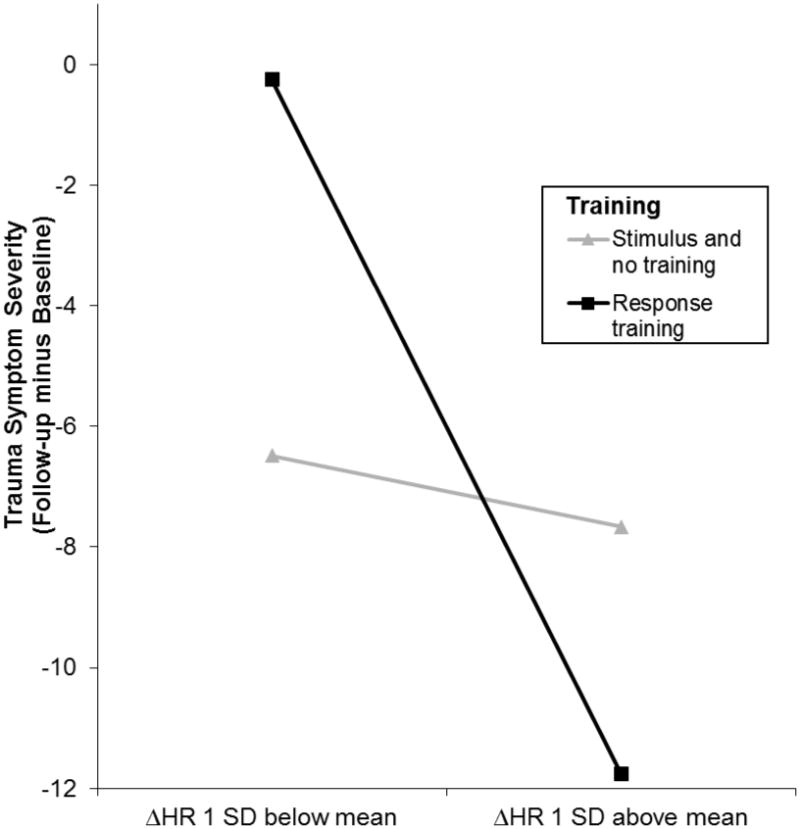
As can be seen in the correlations in Table 6, as predicted (Hypothesis 4), decreases in trauma symptom severity from pre- to post-writing were associated with increases in heart rate and skin conductance during emotional disclosure across all training groups. However, as can be seen in Figure 2, this association was especially evident in response-trained participants (Hypothesis 5). The HR change × Response Training interaction was the only significant term in the simultaneous regression model, Adjusted R2 = .068; t (81)= -2.65, p = .010, β = -.274.
Table 6. Zero-order correlations between Physiological Reactivity and Baseline in Session One and One-Month Follow-up Outcomes.
| DTS-SEV | CES-D | PILL | |
|---|---|---|---|
| Heart rate change | -.208† | -.194† | -.188† |
| Skin conductance change | -.034 | - .099 | -.120 |
| Skin Conductance baseline | -.077 | -.025 | .068 |
| Heart rate baseline | .008 | .132 | .013 |
Note. DTS-SEV refers to trauma symptom severity. Heart rate and skin conductance change are the mean of the last five minutes of baseline subtracted from the mean of minutes 3-8 of writing. DTS-SEV, CES-D, and PILL change were calculated as one-month follow-up subtracted from baseline.
p < .05.
Figure 2. Severity of Trauma Symptoms (DTS) at One Month Follow-up Predicted by HR Change during Emotional Disclosure by Training Condition.
Depression (CES-D)
Table 6 shows that as predicted (Hypothesis 4), decreases in depression symptoms from pre- to post-writing were associated with increases in HR during emotional disclosure for the whole sample. However, as predicted (Hypothesis 5), it was response-trained participants with greater HR who showed a decrease in depression symptoms at follow-up, whereas stimulus-trained and no training participants had similar levels of depression symptoms at follow-up regardless of HR response to emotion writing (see Figure 3). The only significant predictor of depression change in the model was the HR change × Response Training interaction, Adjusted R2= .059; t (87) = -2.55, p = .013, β = -.254.
Figure 3. Depression Symptoms (CES-D) at One Month Follow-up Predicted by HR Change during Emotional Disclosure by Training Condition.

Physical illness symptoms (PILL)
As can be seen in Table 6, as predicted increases in HR during emotional disclosure were associated with decreases in physical illness symptoms from pre- to post-writing (Hypothesis 4). However, as predicted, it was the HR change × Response Training interaction that entered the model first, Adjusted R2= .046; t(80) = 2.22, p = .029, β = -.282, indicating a relationship between physical illness symptoms and HR change very similar to what is depicted in Figures 2 and 3 for trauma and depressive symptoms (Hypothesis 5). After this variable, the SC baseline × Stimulus Training interaction entered the model, Adjusted ΔR2= .048; t(80) = 2.05, p = .043, β=.220. The positive signs on the t and β indicate that higher baseline skin conductance was associated with more physical illness symptoms at one-month follow-up compared to baseline. Although the direction of this relationship was consistent for the entire sample of emotional disclosure writers (note the r=.068 in Table 6), it was significant only for the stimulus trained participants.
Discussion
In this study writing about a stressful event produced negative affect and high arousal compared to neutral writing. Emotional disclosure also resulted in greater heart rate response than neutral writing, although this effect was not statistically significant unless participants were trained to focus on their behavioral and physiological responses to the situations about which they were writing. From baseline to follow-up trauma, depression and physical illness symptoms decreased for participants in both the emotional disclosure and neutral writing conditions, and no training effects were found. As predicted, however, physiological response to emotional disclosure was associated with reduced posttraumatic, depression, and physical symptoms at one-month follow-up, especially in participants who were trained to focus on their responses.
As in previous studies (Sloan et al., 2005; Sloan & Marx, 2004b), written emotional disclosure increased self-reported arousal, decreased pleasantness, and increased HR compared to neutral writing; however HR differences did not reach accepted levels of significance except when response trained. The only other study directly comparing the effect of emotional and neutral writing on HR among college students not screened for trauma history (Epstein et al., 2005) found greater HR for emotional disclosure, with a large effect size (r = .42). On the other hand, Sloan et al. (2007) found, in a study of college students with at least moderate levels of post-traumatic stress symptoms, that HR for emotional disclosure was greater than for neutral writing only when participants were instructed to write “with as much emotion and feeling as possible” (most analogous to response training), but not when participants were instructed to focus on writing with insight and cognitive assimilation. A recent study of college students meeting diagnostic criteria for PTSD also found greater HR for trauma writers instructed to write with as much emotion and feeling as possible (Sloan, Marx, & Greenberg, 2011). Thus, like imagery, written emotional disclosure may result in reliable increases in physiological response only when writers are particularly traumatized/fearful and/or when physiological and emotional expression are emphasized in the processing instructions (Lang et al., 1980, 1983).
Other factors may have contributed to lack of significantly greater HR in emotional disclosure compared to neutral writing in our study. Inspection of the HR means indicates that response training increased HR more than stimulus or no training for neutral writers as well. Response-trained neutral writers were asked to write about their daily activities, and then instructed to “do in your recollection what you would do in the real situation”. Response training elicits situation-appropriate physiological reactivity by facilitating access of motor programs in non-emotional action and exercise scenes (Lang et al., 1980, 1983), and so may have elicited increased HR to writing about emotionally neutral but motorically vigorous daily activities, like biking to class. Unlike imagery studies in which participants are provided carefully-crafted scenarios in which motor activity is controlled, we did not have control over the extent to which neutral writers' daily activities were action-oriented. Another possible contributor to lack of significant HR differences between emotional and neutral writing was baseline differences in depression symptoms. Compared to emotional disclosure writers, neutral writers had higher initial depressive symptoms, which are associated with increased physiological response (Davydov, Zech & Luminet, 2011). Elevated levels of depression in neutral writers may have led to increased physiological reactivity, making it more difficult to find between-group differences.
Trauma, depression, and physical illness symptoms decreased from baseline to follow-up for both emotional disclosure and neutral writing groups. This may be in part due to the higher initial levels of depression in neutral writers. Also, while some studies have found that trauma writing results in greater reductions in psychological and physical symptoms than neutral writing (Epstein et. al., 2005; Sloan et. al., 2004b; Sloan, et. al., 2005), other studies (Kearns et al., 2010; Daniels, 2009; Smyth et al., 2008) have, like the current study, found significant improvements in health for both emotion writers and neutral writers with no group differences. Larger effect sizes have been found for psychological health outcomes when writing studies employed non-college student populations, screened participants for a trauma history, had writing occur at home, and conducted follow-ups less than one month post writing (Frattaroli, 2006). For all of these factors, the current study's design features work against finding greater improvement in psychological health for written emotional disclosure compared to neutral writing.
Response training significantly amplified HR increase to emotional disclosure, but not neutral writing. This supports the hypothesis that written emotional disclosure, like imagery, is a pathway to fully accessing emotional memories (Epstein et al., 2005; Sloan et al., 2005; Sloan et al., 2007). Response training did not affect SC to written emotional disclosure. This replicates imagery studies, which find response training has greater effects on HR than on SC during affective and action imagery (Lang et. al., 1980, 1983; Miller et. al., 1987). Unlike HR, SC is primarily responsive to emotion evoked through external stimulation, such as pictures or videos (Bradley et al., 1992), rather than emotion generated internally, such as through imagery (Lang et. al., 1980). Writing, like imagery, evokes emotion internally; thus SC response may not be suited for investigating emotional response to writing. Although written emotional disclosure increased self-reported unpleasantness and arousal compared to neutral writing, response training did not enhance this difference. The effect of response training on self-reported affect during emotional imagery has been mixed (Lang et al., 1980, 1983; Miller et al., 1987), and illustrates the frequently-found discordance between verbal and physiological channels in emotional responding.
Like other forms of imaginal and in vivo exposure (Beckham et al., 1990; Lang et al., 1970; Watson & Marks, 1971), this study found that greater physiological reactivity to written emotional disclosure was associated with improved health; in this case greater reductions in depression, posttraumatic symptoms, and physical illness symptoms at a one-month follow-up. This finding replicates previous research (Sloan et al., 2004b; Epstein et al., 2005), and adds to the literature that complete activation of the emotional memory network during exposure, including measurable physiological output, is associated with better outcome. Consistent with the data reviewed by Craske and her colleagues (Craske et al., 2008), this result was found only in heart rate, and not in skin conductance. Since written emotional disclosure acts like exposure in improving outcomes when physiological response is increased, this should encourage more future study of writing assignments as a technique for treating anxiety disorders.
What is new in this study is that response-trained emotional disclosers showed the greatest association between HR increase and symptom reduction at follow-up. Response training has been shown to amplify situation-appropriate physiological response to imagery exposure (Lang et al., 1980, 1983; Miller et al., 1987), but this is the first study to show that response training enhances the association between physiological response and improved outcomes. Since response training increases physiological response to fear and trauma processing during imagery, and now written exposure, and since in this study response training was uniquely associated with the relationship between physiological response and health outcomes, response training should be evaluated as an adjunct to exposure therapy or any procedure that employs emotional processing. One caution, however, can be seen in Figures 2 and 3: response-trained participants who exhibited lower levels of HR increase may actually show less symptom improvement than other conditions. Thus, research needs to attend to who benefits, and who does not benefit, from response training. Greater baseline skin conductance output, which is indicative of greater sympathetic nervous system activity, was associated with poorer physical illness outcomes. However, this result should be considered tentative since it reached statistical significance only in interaction with stimulus training, a result that was neither predicted nor easily explicable.
It is important to note that the current results were found with college students who were not selected for traumatic experiences or posttraumatic symptoms. Thus the events related during written emotional disclosure in this study range from merely distressing to truly traumatic (see Table 4), and so the findings should not be seen as applicable to clinical treatment contexts. Thus, these findings need to be replicated with clinical populations. Additional studies are warranted with analog and clinical populations to investigate whether the effects of response training are found with imaginal and in vivo exposure as well as written emotional disclosure.
Across the spectrum of emotional distress, exposure to and tolerance of the distress are seen to have a corrective impact. However, such approaches are not always effective, whether they involve college students emotionally disclosing a negative life experience or exposure therapy for anxiety disorders (Noyes, 1991), and thus innovations to enhance efficacy are needed. Although the current study's effects are limited to students unselected for traumatic experiences, is speculated that response training may be a particularly effective adjunct for treating the most severe and chronic anxiety disorder cases. Recent research has found that, over the entire anxiety disorder spectrum, physiological blunting during exposure to fear imagery is more pronounced among the most severe patients; such as those with more traumatic experiences, greater chronicity, negative affectivity, and poorer prognosis (McTeague et al., 2010). As such, these individuals may benefit the most from response training to enhance physiological response to exposure. Future research should assess variables that have been related to physiological blunting and determine if these results can generalize to clinical samples.
Highlights.
Written emotional disclosure has physical and mental health benefits
College students wrote about their most distressing life event for 3 20-min sessions
Increased HR while writing predicted better mental and physical health at 1 month
Training to increase physiology improved relationship between HR and outcome
Acknowledgments
This research was supported in part by a grant from the National Institutes of Mental Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Beckham JC, Vrana SR, May JG, Gustafson DJ, Smith GR. Emotional processing and fear measurement synchrony as indicators of treatment outcome in fear of flying. Journal of Behavior Therapy and Experimental Psychiatry. 1990;21:153–162. doi: 10.1016/0005-7916(90)90002-3. [DOI] [PubMed] [Google Scholar]
- Boals A. The use of meaning making in expressive writing: When meaning is beneficial. Journal of Social and Clinical Psychology. 2012;31:393–409. doi: 10.1521/jscp.2012.31.4.393. [DOI] [Google Scholar]
- Boucsein W. Electrodermal Activity. Plenum; New York: 1992. [Google Scholar]
- Bradley MM, Greenwald MK, Petry MC, Lang PJ. Remembering pictures: Pleasure and arousal in memory. Journal of Experimental Psychology: Learning, Memory, and Cognition. 1992;18:379–390. doi: 10.1037/0278-7393.18.2.379. [DOI] [PubMed] [Google Scholar]
- Bradley MM, Lang PJ. Measuring emotion: The self-assessment manikin and the semantic differential. Journal of Behavior Therapy and Experimental Psychology. 1994;25:49–59. doi: 10.1016/0005-7916(94)90063-9. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control. Adverse Childhood Experiences Reported by Adults --- Five States, 2009. Morbidity and Mortality Weekly Report. 2010;59:1609–1613. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5949a1.htm. [PubMed] [Google Scholar]
- Craske MG, Kircanski K, Zelikowsky M, Mystkowski J, Chowdhury N, Baker A. Optimizing inhibitory learning during exposure therapy. Behaviour Research and Therapy. 2008;46:5–27. doi: 10.1016/j.brat.2007.10.003. [DOI] [PubMed] [Google Scholar]
- Davidson JRT, Book SW, Colket JT, Tupler LA, Roth S, David D, et al. Assessment of a new self-rating scale for post-traumatic stress disorder. Psychological Medicine. 1997;27:153–160. doi: 10.1017/S0033291796004229. [DOI] [PubMed] [Google Scholar]
- Davydov DM, Zech E, Luminet O. Affective context of sadness and physiological response patterns. Journal of Psychophysiology. 2011;25:67–80. doi: 10.1027/0269-8803/a000031. [DOI] [Google Scholar]
- Epstein EM, Sloan DM, Marx BP. Getting to the heart of the matter: Written disclosure, gender, and heart rate. Psychosomatic Medicine. 2005;67:413–419. doi: 10.1097/01.psy.0000160474.82170.7b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Marks JS. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventative Medicine. 1998;14:245–58. doi: 10.1016/s0749-3797(98)00017-8. [DOI] [PubMed] [Google Scholar]
- Foa EB, Kozak MJ. Emotional processing of fear: Exposure to corrective information. Psychological Bulletin. 1986;99:20–35. doi: 10.1037/0033-2909.99.1.20. [DOI] [PubMed] [Google Scholar]
- Frattaroli J. Experimental disclosure and its moderators: A meta-analysis. Psychological Bulletin. 2006;6:823–865. doi: 10.1037/0033-2909.132.6.823. [DOI] [PubMed] [Google Scholar]
- Greenberg MA, Stone AA. Emotional disclosure about traumas and its relation to health: effects of previous disclosure and trauma severity. Journal of Personality and Social Psychology. 1992;63:75–84. doi: 10.1037/0022-3514.63.1.75. [DOI] [PubMed] [Google Scholar]
- Kearns MC, Edwards KM, Calhoun KS, Gidycz CA. Disclosure of sexual victimization: Effects of Pennebaker's emotional disclosure paradigm on physical and psychological distress. Journal of Trauma and Dissociation. 2010;11:193–209. doi: 10.1080/15299730903502979. [DOI] [PubMed] [Google Scholar]
- Kloss JD, Lisman SA. An exposure-based examination of the effects of written emotional disclosure. British Journal of Health Psychology. 2002;7:31–46. doi: 10.1348/135910702169349. [DOI] [PubMed] [Google Scholar]
- Lang PJ. A bio-informational theory of emotional imagery. Psychophysiology. 1979;16:495–512. doi: 10.1111/j.1469-8986.1979.tb01511.x. [DOI] [PubMed] [Google Scholar]
- Lang PJ. Cognition in emotion: concept and action. In: Izard CE, Kagan J, Zajonc RB, editors. Emotions, cognition and behavior. Cambridge University; 1984. pp. 192–226. [Google Scholar]
- Lang PJ, Kozak MJ, Miller GA, Levin DN, McLean A., Jr Emotional imagery: Conceptual structure and pattern of somato-visceral response. Psychophysiology. 1980;17:179–92. doi: 10.1111/j.1469-8986.1980.tb00133.x. [DOI] [PubMed] [Google Scholar]
- Lang PJ, Levin DN, Miller GA, Kozak MJ. Fear behavior, fear imagery and the psychophysiology of emotion: The problem of affective response integration. Journal of Abnormal Psychology. 1983;92:276–306. doi: 10.1037/0021-843X.92.3.276. [DOI] [PubMed] [Google Scholar]
- Lang PJ, Melamed BG, Hart J. A psychophysiological analysis of fear modification using an automated desensitization procedure. Journal of Abnormal Psychology. 1970;76:220–234. doi: 10.1037/h0029875. [DOI] [PubMed] [Google Scholar]
- Lumley MA, Provenzano KM. Stress management through written emotional disclosure improves academic performance among college students with physical symptoms. Journal of Educational Psychology. 2003;95:641–649. doi: 10.1037/0022-0663.95.3.641. [DOI] [Google Scholar]
- McClernon JF, Beckham JF, Mozley SL, Feldman ME, Vrana SR, Rose JE. The effects of trauma recall and smoking topography in posttraumatic stress disorder and non- posttraumatic stress disorder trauma survivors. Addictive Behaviors. 2005;30:247–257. doi: 10.1016/j.addbeh.2004.05.013. [DOI] [PubMed] [Google Scholar]
- McTeague LM, Lang PJ, Laplante MC, Cuthbert BN, Shumen JR, Bradley MM. Aversive imagery in posttraumatic stress disorder: trauma recurrence, comorbidity, and physiological reactivity. Biological Psychiatry. 2010;67:346–356. doi: 10.1016/j.biopsych.2009.08.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller GA, Levin DN, Kozak MJ, Cook EW, III, McLean A, Jr, Lang PJ. Individual differences in imagery and the psychophysiology of emotion. Cognition and Emotion. 1987;1:367–390. doi: 10.1080/02699938708408058. [DOI] [Google Scholar]
- National Institute of Mental Health. NIMH Research Domain Criteria (RDoC) 2011 Retrieved from http://www.nimh.nih.gov/research-priorities/rdoc/nimh-research-domain-criteria-rdoc.shtml.
- Noyes R. The clinical management of anxiety disorders. In: Coryell W, Winokur G, editors. Treatments of choice for anxiety disorders. Oxford University Press; 1991. pp. 140–153. [Google Scholar]
- Pennebaker JW. The psychology of physical symptoms. New York: Springer Verlag; 1982. [Google Scholar]
- Pennebaker JW. Writing about emotional experiences as a therapeutic process. Psychological Science. 1997;8:162–166. doi: 10.1111/j.1467-9280.1997.tb00403.x. [DOI] [Google Scholar]
- Pennebaker JW, Beall SK. Confronting a traumatic event: Toward an understanding inhibition and disease. Journal of Abnormal Psychology. 1986;95:274–281. doi: 10.1037/0021-843X.95.3.274. [DOI] [PubMed] [Google Scholar]
- Petrie KJ, Booth RJ, Pennebaker JW, Davison KP, Thomas MG. Disclosure of trauma and immune response to a Hepetitis B vaccination program. Journal of Consulting and Clinical Psychology. 1995;63:787–792. doi: 10.1037/0022-006X.63.5.787. [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- Resick PA, Galovski TE, Uhlmansiek MO, Scher CD, Clum GA, Young-Xu Y. Randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence. Journal of Consulting and Clinical Psychology. 2008;76:243–258. doi: 10.1037/0022-006X.76.2.243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shean G, Baldwin G. Sensitivity and specificity of depression questionnaires in a college-age sample. The Journal of Genetic Psychology. 2008;169:281–288. doi: 10.3200/GNTP.169.3.281-292. [DOI] [PubMed] [Google Scholar]
- Sloan DM, Marx BP. Taking pen to hand: Evaluating theories underlying the written disclosure paradigm. Clinical Psychology: Science and Practice. 2004a;11:121–137. doi: 10.1093/clipsy/bph062. [DOI] [Google Scholar]
- Sloan DM, Marx BP. A closer examination of the structured written disclosure procedure. Journal of Consulting and Clinical Psychology. 2004b;72:165–175. doi: 10.1037/0022-006X.72.2.165. [DOI] [PubMed] [Google Scholar]
- Sloan DM, Marx BP. Exposure though written emotional disclosure: two case examples. Cognitive and Behavioral Practice. 2006;13:227–234. doi: 10.1016/j.cbpra.2005.08.001. [DOI] [Google Scholar]
- Sloan DM, Marx BP, Epstein EM. Further examination of the exposure model underlying the efficacy of written emotional disclosure. Journal of Consulting and Clinical Psychology. 2005;73:549–554. doi: 10.1037/0022-006X.73.3.549. [DOI] [PubMed] [Google Scholar]
- Sloan DM, Marx BP, Epstein EM, Lexington JM. Does altering the writing instructions influence outcome associated with written disclosure? Behavior Therapy. 2007;38:155–168. doi: 10.1016/j.beth.2006.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sloan DM, Marx BP, Greenberg EM. A test of written emotional disclosure as an intervention for posttraumatic stress disorder. Behaviour Research and Therapy. 2011;49:299–304. doi: 10.1016/j.brat.2011.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smyth JM, True N, Souto J. Effects of writing about traumatic experiences: The necessity for narrative structuring. Journal of Social and Clinical Psychology. 2001;20:161–172. doi: 10.1521/jscp.20.2.161.22266. [DOI] [Google Scholar]
- Smyth JM, Hockemeyer JR, Tulloch H. Expressive writing and post-traumatic stress disorder: Effects on trauma symptoms, mood states, and cortisol reactivity. British Journal of Health Psychology. 2008;13:85–93. doi: 10.1348/135910707X250866. [DOI] [PubMed] [Google Scholar]
- Van Emmerik AAP, Reijntjes A, Kamphuis JH. Writing therapy for posttraumatic stress: A meta-analysis. Psychotherapy and Psychosomatics. 2013;82:82–88. doi: 10.1159/00343131. [DOI] [PubMed] [Google Scholar]
- Vrana S, Lauterbach D. Prevalence of traumatic events and post-traumatic psychological symptoms in a non-clinical sample of college students. Journal of Traumatic Stress. 1994;7:289–302. doi: 10.1002/jts.2490070209. [DOI] [PubMed] [Google Scholar]
- Watson JP, Marks IM. Relevant and irrelevant fear in flooding-A crossover study of phobic patients. Behavior Therapy. 1971;2:275–293. doi: 10.1016/S0005-7894(71)80062-X. [DOI] [PubMed] [Google Scholar]