

Abstract
Clinical genetic testing for specific isolated congenital heart defects (CHD) is becoming standard of care in pediatric cardiology practice. Both genetic knowledge and attitudes toward genetic testing are associated with an increased utilization of genetic testing, but these factors have not been evaluated in parents of children with CHD. We mailed a survey to measure the demographics, genetic knowledge, and attitudes towards genetic testing of parents of children with CHD who previously consented to participate in a separate research study of the genetic etiology of left ventricular outflow tract malformations (LVOT). Of the 378 eligible families, 190 (50%) returned surveys with both parents completing surveys in 97 (51%) families, resulting in 287 participants. Genetic knowledge was assessed on an adapted measure on which the mean percent correct was 73.8%. Educational attainment and household income were directly and significantly associated with genetic knowledge (p<0.001). Attitudes about the health effects of genetic testing were favorable with at least 57% agreeing that genetic testing would be used for managing health care and finding cures for disease. Conversely, a minority of participants found it likely that genetic testing would be used for insurance (up to 39.9%), employment (15.8%), or racial/social discrimination (up to 11.2%). Parents of younger children were less likely to endorse employment or racial/social discrimination. Genetic knowledge was not correlated with specific attitudes. Among parents of children with CHD, genetic knowledge was directly associated with household income and education, but additional research is necessary to determine what factors influence attitudes towards genetic testing.
Keywords: Health Knowledge, Attitudes, and Practice, Heart Defects, Congenital, Multifactorial Inheritance, Genetic Testing
INTRODUCTION
Genetic testing for isolated congenital heart defects (CHD), a multifactorial genetic disease, is gradually being introduced in the inpatient and outpatient settings. Although array comparative genomic hybridization (CGH) has been shown to be useful in patients with severe CHD and CHD in addition to dysmorphic features, developmental delay, and/or other birth defects[Bachman et al., 2013; Connor et al., 2014], few causative genes have been identified for isolated CHDs. Even fewer have been translated into a clinical test; therefore, it is a minor portion of the isolated CHD population for whom a genetic test is clinically indicated. This is expected to change in the future due to knowledge from exome sequencing. If a specific genetic etiology was identified via genetic testing for a particular patient, this could result in elucidation of the recurrence risk, clarification of the type and risk of complications (e.g., aortic dilation or arrhythmia), and possibly identification of a specific treatment. Thus it is important to examine the genetic knowledge and attitudes of parents of children with CHD before genetic testing is commonplace in this population.
Although there is little literature on the genetic knowledge of parents of children with CHD, the genetic knowledge of community samples has generally been associated with education and age [Calsbeek et al., 2007; Haga et al., 2013; Molster et al., 2009; Rose et al., 2005a]. There are few studies of parental knowledge about genetics, and those that exist are focused mainly on disease specific knowledge for childhood diseases with a definitive genetic component such as cystic fibrosis and sickle cell disease [Lang et al., 2009; Sawyer et al., 1998]. As a first step, parental knowledge of the name of their child’s CHD has been studied with variable understanding reported, 27% to 90% [Van Deyk et al., 2004].
While attitudes toward genetic testing among parents of children with CHD remain unknown, surveys of general public’s attitudes about genetic testing conducted in the U.S. and abroad [Molster et al., 2009; Rose et al., 2005a; Rose et al., 2005b; Wang et al., 2001] have, in general, found favorable attitudes with some concern about insurance discrimination. Additionally, parents generally have a positive attitude towards and interest in genetic testing for childhood [Brunger et al., 2000; Patenaude et al., 1996] and adult onset conditions [Campbell et al., 2005; Tercyak et al., 2011].
Previous research focused on breast cancer has shown that higher genetic knowledge and more positive or less negative attitudes are linked to increased genetic test utilization [Lerman et al., 1996; Peters et al., 2005] and also anticipated utilization [Quinlivan et al., 2014]. Several studies have demonstrated an association between higher genetic knowledge and favorable attitudes toward genetic testing [Buseh et al., 2014; Ishiyama et al., 2008; Morren et al., 2007; Rose et al., 2005a], while conversely, there is also literature suggesting greater knowledge of genetics may decrease interest in genetic testing due to negative attitudes about the use of test results (i.e., insurance discrimination) [Armstrong et al., 2000; Armstrong et al., 2002; Peterson et al., 2002]. Additionally, a few studies have noted that those with lower genetic knowledge [Jallinoja et al., 2000; Morren et al., 2007] or lower educational attainment [Willis et al., 2013] are more likely to report neutral attitudes as they may experience difficulty taking a positive or negative stance.
In this study, we examined the genetic knowledge and attitudes toward genetic testing of parents of children with heart defects affecting the left ventricular outflow tract (LVOT). These defects encompass a wide range of severities, including bicuspid aortic valve (BAV) at the mild end of the spectrum, the moderate severity defects aortic stenosis (AS) and coarctation of the aorta (CoA), and the most severe form as hypoplastic left heart syndrome (HLHS). The aims of this study were threefold: (1) Examine the current level of genetic knowledge among parents of children with LVOT malformations and determine factors associated with higher knowledge; (2) Describe current attitudes toward genetic testing and factors related to the acceptance of certain beliefs; and (3) Determine whether genetic knowledge is associated with certain attitudes toward genetic testing.
MATERIALS AND METHODS
Study Sample
We conducted a survey of parents who previously consented for their child (proband) to participate in the “Genetics of Left Ventricular Outflow Tract (LVOT) Malformations” study, hereafter referred to as the LVOT Genetics Study (additional information on the consent process can be found in [Klima et al., 2014]). Both studies were approved by the Institutional Review Board. All parents, including adoptive parents, step parents, and legal guardians, were eligible for this study if they participated in the consent process for the LVOT Genetics Study between April 2005 and April 2010, were English-speaking, had a valid address, and their child was 0–20 years old at the time of consent for the LVOT Genetics Study. Parents were excluded if they no longer had custody of the proband or if the proband was deceased.
Study Procedure
An introductory letter was sent to all eligible families that included an opt-out phone number to decline study participation. Study packets were mailed two weeks later to all families who did not decline. This mailing occurred in September of 2010 and included a $3 incentive. If a response was not received within 2 weeks, another study packet was sent. Families who had not responded after the second packet was sent were called to remind them to complete the study packets.
Survey Instruments
Demographics
Demographic characteristics, including parent age, gender, race/ethnicity, education, marital status, household income, and current employment, were measured using items from the Behavioral Risk Factor Surveillance System (BRFSS) 2009 questionnaire (Center for Disease Control and Prevention, Atlanta, GA). Parental occupation was obtained using two open-ended questions from The United States Census 2000 Long-Form Questionnaire (U.S. Census Bureau, Washington, MD) and then coded using the 2010 Standard Occupation Classification (SOC) System Manual (U.S. Bureau of Labor Statistics, Washington D.C.). The SOC was used to collapse 840 occupations into 6 high-level aggregation groups and also to create a binary variable of health/science occupation versus other occupation. Proband characteristics and information on the time since LVOT Genetics Study consent were obtained from that study database. Parents were also asked to indicate their relationship to the proband. Two questions about use of the internet to search for health information were taken from the Internet & American Life Project (Pew Research Center, Washington D.C.).
Genetic Knowledge
Knowledge about genetics was assessed with an 18-item true/false instrument [Jallinoja et al., 1999] and modified for use in this study (see Table 3 for the modified items). Specifically, this instrument measures knowledge of the structure and function of genes, as well as the relationship between genetics, heredity, and the onset of disease. Correct answers were given a score of 1, while incorrect or “Don’t Know” answers were given a score of 0. A summary score was created by summing the score for all 18 items for each participant who completed all 18 knowledge questions. This score was then used to calculate a percent correct.
Table III.
Univariate estimates of genetic knowledge by participant and proband characteristics.
| Low (%) | High (%) | Model χ2 | p-value | |
|---|---|---|---|---|
| Parent Age Group | ||||
| ≤ 40 years | 54.9 | 45.1 | 2.18 | 0.14 |
| >40 years | 62.9 | 37.1 | ||
| Gender | ||||
| Male | 55.3 | 44.7 | 0.68 | 0.41 |
| Female | 60.4 | 39.6 | ||
| Race | ||||
| Other | 50.0 | 50.0 | 0.85 | 0.36 |
| White | 59.1 | 40.9 | ||
| Education | ||||
| ≤ HS diploma | 83.8 | 16.2 | 22.8 | <0.001 |
| Some college or more | 49.0 | 50.7 | ||
| Marital Status | ||||
| Married | 56.4 | 43.6 | 0.88 | 0.35 |
| Not married | 67.4 | 32.6 | ||
| Household Income | ||||
| ≥ $75,000 | 45.1 | 54.9 | 14.1 | <0.001 |
| $35,000–$74,999 | 62.5 | 37.5 | ||
| <$35,000 | 76.2 | 23.8 | ||
| Employment | ||||
| Employed/Self-employed | 54.7 | 45.3 | 3.31 | 0.19 |
| Homemaker | 70.7 | 29.3 | ||
| Unemployed | 69.0 | 31.0 | ||
| SOC1 Occupational Classification | ||||
| Management, business, science, and arts | 57.9 | 42.1 | 0.00 | 0.96 |
| Other | 65.0 | 35.0 | ||
| Health/Science Occupation | ||||
| Health & Science | 54.8 | 45.3 | 0.87 | 0.35 |
| Other | 60.6 | 39.4 | ||
| Proband Age | ||||
| ≥ 9 years | 65.3 | 34.8 | 3.75 | 0.05 |
| < 9 years | 53.9 | 46.1 | ||
| Congenital Heart Defect | ||||
| AS | 63.8 | 36.2 | 3.63 | 0.46 |
| BAV | 60.4 | 39.6 | ||
| CoA | 54.2 | 45.8 | ||
| HLHS | 68.3 | 31.7 | ||
| Other | 45.0 | 55.0 | ||
| Searched on-line for medical information (Yes) | 56.9 | 43.1 | 2.6 | 0.10 |
| Searched on-line for heart defect (Yes) | 58.4 | 41.6 | 0.11 | 0.74 |
Standard Occupational Classification
Genetic Testing Attitudes
Attitudes towards genetic testing were measured with a 12-item scale [Rose et al., 2005a] which measured individuals’ attitudes about how results from genetic tests may be used in three domains: health effects, insurance/employment discrimination, and racial/social discrimination. Although developed with a 4-point likelihood scale (very likely, somewhat likely, not too likely, not at all likely), we added a “neutral” option to each statement as previous studies have found that some individuals may have neutral attitudes [Jallinoja et al., 2000; Morren et al., 2007]. Therefore, the attitude measure was scored on a 5-point scale (1=very likely, 2=somewhat likely, 3=neutral, 4=not too likely, 5=not at all likely).
Statistical Analysis
The internal consistency of the genetic knowledge and the attitudes measures were assessed by calculating Cronbach’s alpha in SPSS version 21. All remaining statistical analyses were performed using SAS 9.2[92]. Statistical significance was set at p<.01 to account for the multiple analyses.
Genetic knowledge was examined initially as a continuous variable and then as a dichotomous variable by utilizing a median split. The cut-point for the median split was 80% correct on the genetic knowledge measure such that all scores in the 80th percentile and above were in the “high” category and those scores below the 80th percentile were in the “low” category. As the results were equivalent when examining genetic knowledge as a continuous and dichotomous variable, the dichotomous variable was utilized for ease of interpretation. Independent variables were examined as predictors of high knowledge utilizing a general estimating equation (GEE) models with a binomial link function specified by PROC GENMOD. The REPEATED statement was employed to account for non-independence due to within family correlation when two parents of the same proband participated. The results of the univariate models are presented as model χ2 Score statistics and p-values. The final multivariate model is presented as adjusted odds ratios, 95% confidence intervals, and p-values.
Attitudes toward predictive testing were initially evaluated with univariate descriptive statistics and multivariate models as described above. Each of the 12 items was examined separately by modeling the probability that participants responded “likely” (very likely or somewhat likely) to a given statement about how genetic testing results could be used. Odds ratios and 95% confidence intervals are reported for those items that were significantly associated with independent variables. Finally, genetic knowledge scores were related to each attitude item using PROC GENMOD as previously described.
RESULTS
Sample Characteristics
Of the 392 families who met inclusion criteria, 14 families were subsequently excluded for the following reasons: lack of custody of the proband (2 families), proband was deceased (1 family), and lack of a valid address (11 families). Of the remaining eligible families, 2 actively declined participation, 186 were non-responders, and 190 responded (50.3% response rate). When comparing the probands whose parents responded to the non-responders, there were no statistically significant differences in age at consent for the LVOT Genetics Study, gender, race, or type of CHD. Of the 190 responding families, both parents responded in 97 families, resulting in 287 parent participants. The demographic characteristics of these 287 participants and 190 probands are reported in Table I. Most participants were more than 40 years old (53.3%), white (94.4%), and had completed at least some college (73.9%). Most probands (86.1%) were under the age of 16 at the time of consent for the LVOT Genetics Study and the most common CHD in this cohort was CoA (41.1%).
Table I.
Characteristics of participants (n is noted if not 287) and probands (n=190).
| Parent Participants | Percentage (%) |
|---|---|
| Age Group | |
| ≤ 40 years | 53.3 |
| >40 years | 46.7 |
| Male | 36.2 |
| Race | |
| White | 94.4 |
| Other | 5.6 |
| Education (n=285) | |
| ≤ HS Diploma | 26.1 |
| Some college or more | 73.9 |
| Household income (n=274) | |
| ≥$75,000 | 42.0 |
| $35,000–$74,999 | 35.0 |
| < $35,000 | 23.0 |
| Employment (n=284) | |
| Employed/Self-employed | 74.4 |
| Homemaker | 14.4 |
| Unemployed | 10.2 |
| SOC1 occupational classification (n=281) | |
| Management, business, science, and arts | 47.0 |
| Other | 53.0 |
| Searched on-line for medical information (Yes) | 84.0 |
| Searched on-line for information on heart defect (Yes) | 73.5 |
| Probands | Percentage (%) |
| Age at consent for LVOT study | % |
| 0–1 year | 25.4 |
| 2–8 years | 32.8 |
| 9–15 years | 27.9 |
| 16–21 years | 13.9 |
| Primary Congenital Heart Defect | |
| Coarctation of the aorta (CoA) | 41.1 |
| Aortic stenosis (AS) | 20.9 |
| Bicuspid aortic valve (BAV) | 16.7 |
| Hypoplastic left-heart syndrome (HLHS) | 14.3 |
| Other (Shone2, IAA-A3, MS4) | 6.9 |
Standard Occupational Classification
Shone complex
Interrupted aortic arch type A
Mitral stenosis
Genetic Knowledge
The mean genetic knowledge summary score was 73.8% correct (SD=19.1%, range 0–100%, n=265). The percent of participants answering each item correctly ranged from 28.4% to 97.2% (Table II). The items most frequently answered correctly related to the interaction of genetic and environmental factors (e.g., “Some diseases are caused by genes, environment, and lifestyle”, true, 97.2% correct) while the items that participants had the most difficulty with were those related to basic genetic knowledge (e.g., “Humans have 20 pairs of chromosomes”, false, 28% correct). The 18 items of the genetic knowledge score had a Cronbach’s alpha of 0.814, indicating good internal consistency.
Table II.
Items of the modified genetic knowledge measure listed by percentage of participants correctly answering each item.
| % Correct | |
|---|---|
| Some diseases are caused by genes, environment, and lifestyle. (true) | 97.2 |
| Genes determine traits such as height, eye color, and facial appearance. (true) | 96.8 |
| Healthy parents can have a child with an inherited disease. (true) | 95.7 |
| A gene is a disease. (false) | 91.6 |
| You can see a gene with the naked eye. (false) | 90.8 |
| All serious diseases are inherited. (false) | 89.4 |
| A genetic test can tell you if you have a higher chance to develop a specific disease. (true) | 84.9 |
| The child of a person with an inherited disease will always have the same disease. (false) | 84.2 |
| A gene is a piece of DNA. (true) | 81.1 |
| Altered (mutated) genes can cause disease. (true) | 79.3 |
| A person with an altered (mutated) gene may be completely healthy. (true) | 77.2 |
| A person has thousands of genes. (true) | 68.8 |
| A chromosome contains many genes. (true) | 64.4 |
| Genes are inside of cells. (true) | 63.7 |
| Genes are instructions for making proteins, which help the body grow and work properly. (true) | 49.3 |
| Identical twins have different sets of genes. (false) | 48.1 |
| Parents pass both copies of each chromosome to their child. (false) | 36.5 |
| Humans have 20 pairs of chromosomes. (false) | 28.4 |
When a median split was used to designate high and low knowledge groups, the mean percentage of correct items for the high category was 89.9% (41.8% of participants) and 62.2% (58.2% of participants) for the low category. In univariate analyses, educational attainment and household income were associated with high knowledge (Table III). When modeled together, only education remained significant at p=.001. Participants who had completed some college or more were 3.2 (95% C.I., 1.6 – 6.5) times more likely to demonstrate high genetic knowledge compared with those who had completed high school or less education.
Attitudes about Genetic Testing
The majority of participants held positive attitudes about the health effects of genetic testing (Supplementary Data) with 57.9% to 89.4% of participants responding that it was somewhat or very likely that hypothetical genetic testing would be used for each of the health effects. Conversely, a minority of participants (15.8%–39.9%) thought insurance and employment discrimination was likely. Similarly, only 8.8–11.2% of participants thought racial or social discrimination was likely. The twelve genetic attitudes items had a Cronbach’s alpha of 0.892, indicating good internal consistency.
Several attitude items were associated with parent demographic or proband characteristics (Table IV). Participants who reported an annual household income of $75,000 or more were significantly less likely to respond that genetic testing would be used to help them decide whether to have any, or more, children compared with participants reporting less than $35,000 in household income. Parents of children with CoA, AS, and BAV were more likely to agree that genetic test results would be used to prevent their family from getting health insurance as compared to parents of children with HLHS. Parents of younger probands (0–1, 2–8, and 9–15 versus 16–21 years old) were significantly less likely to agree that results would prevent themselves from getting a job (p=.009) and would be used to discriminate against certain racial or ethnic groups (p=.005). Only the parents of children 0–1 year old were less likely to agree that test results would allow the government to label certain groups as inferior (p=.002).
Table IV.
Adjusted associations of participants’ attitudes about how genetic testing is used.
| ‘Likely’ that a genetic test would be used……… | Odds ratio | 95% CI | p value | |
|---|---|---|---|---|
| To help you decide to have any, or more, children | Income | 0.003 | ||
| <$35,000 | 1 | |||
| $35,000–$74,999 | 0.6 | 0.46–1.93 | 0.89 | |
| ≥$75,000 | 0.36 | 0.19–0.71 | 0.003 | |
| To prevent your family from getting health insurance | Congenital Heart Defect | 0.003 | ||
| HLHS | 1 | |||
| CoA | 4.28 | 1.26–14.51 | 0.02 | |
| AS | 5.54 | 1.55–20.04 | 0.009 | |
| BAV | 10.11 | 2.66–38.41 | 0.0007 | |
| Other | 3.2 | 0.70–14.51 | 0.132 | |
| To prevent you from getting a new job or promotion | Proband Age | 0.009 | ||
| 16–21 years | 1 | |||
| 9–15 years | 0.31 | 0.11–0.82 | 0.019 | |
| 2–8 years | 0.24 | 0.09–0.66 | 0.006 | |
| 0–1 year | 0.11 | 0.03–0.35 | 0.0002 | |
| To allow the government to label certain groups as inferior | Proband Age | 0.005 | ||
| 16–21 years | 1 | |||
| 9–15 years | 0.39 | 0.14–1.15 | 0.088 | |
| 2–8 years | 0.41 | 0.14–1.23 | 0.113 | |
| 0–1 year | 0.08 | 0.02–0.39 | 0.002 | |
| To discriminate against certain racial or ethnic groups | Proband Age | 0.005 | ||
| 16–21 years | 1 | |||
| 9–15 years | 0.29 | 0.09–0.95 | 0.040 | |
| 2–8 years | 0.26 | 0.08–0.83 | 0.024 | |
| 0–1 year | 0.04 | 0.004-.031 | 0.002 |
Association between Genetic Knowledge and Attitudes
Genetic knowledge was not found to be associated with any attitude item (Supplementary Data). Although it did not reach statistical significance, the association between genetic knowledge and agreeing that genetic test results could be used “to help scientists find cures for diseases” was verging on statistical significance (p=0.02).
DISCUSSION
Genetic testing is available for a number of congenital conditions diagnosed in childhood, yet little is known about parents’ knowledge and attitudes of genetics and genetic testing. Parents of children with genetic diseases or multifactorial diseases with a genetic etiology [Brunger et al., 2000; Fitzgerald-Butt et al., 2010; Henneman et al., 2001; Kocken et al., 2013; Skinner et al., 2003; Umans-Eckenhausen et al., 2002], in general, have a positive attitude towards genetic testing and are interested in testing their children. Previous research has not shown whether parents understand genetics, genetic testing, and the implications of genetic testing for their child and family. This has implications for the uptake of genetic tests for a wide variety of pediatric diseases including CHD as well as what type of educational and decision support tools should be made available for parents.
To our knowledge, this is the first study to examine the genetic knowledge and attitudes towards genetic testing of parents of children with congenital heart defects. Our large sample size, almost 300 parents, allowed us to capture a cross-section of this parent population and also detect significant associations. Lastly, the instruments used to measure genetic knowledge and genetic attitudes had high internal consistency, suggesting stability among the items for measuring genetic knowledge and attitudes. Further testing of their concurrent validity when compared to other validated measures and their test-retest reliability is warranted.
Participants in this study, in general, had a better understanding of how genes and the environment interact to cause disease as compared to basic genetic concepts. This is consistent with previous findings in the Finnish population [Jallinoja et al., 1999]. Our cohort performed better on most items, with correct responses ranging from 28% to 97%, as compared to 18% to 88%, which may be explained by our cohort being younger and having higher educational attainment, on average. Also, our study was conducted more than a decade later, which may suggest that our cohort had increased media and educational exposure to genetics.
Previous studies on genetic knowledge have found a relationship between high genetic knowledge and educational attainment [Jallinoja et al., 1999; Rose et al., 2005a], a finding that this study confirms. As only a minority of adults who attend college complete a genetics course, it is likely that those adults with at least some college education are able to learn complex information more easily. Careful planning on the part of health educators and genetic counselors could fill in the knowledge gaps experienced by these parents prior to genetic testing. Quantitative surveys, such as the one used in this study, could provide a framework for these healthcare professionals to meet the individual genetic education needs.
The parents in this study have relatively positive views toward predictive genetic testing. At least 70% agreed that it was likely that genetic testing could be used to improve health care, research, and lifestyle choices. These results are similar to those found utilizing the same and alternative attitudes instruments with the general population in the United States and Europe [Henneman et al., 2006; Rose et al., 2005a].
Compared to the Rose study, we found that a slightly higher proportion of participants agreed with using genetic information for family planning which is likely related to the younger average age of our cohort. This result varied significantly according to income level, with parents of higher income levels being less likely to agree. This may be explained by lower income families being more concerned about having another child with a CHD due to the potential financial burden, particularly if they lack or have inadequate health insurance.
We found that parents of children with HLHS are less concerned about genetic test results preventing their family from getting insurance when compared to the parents of children with all of the other, less severe, heart defects. Children with HLHS incur huge medical bills in the first few months of life which may make parents less concerned about the effects of a genetic test on insurability. On the other hand, many children with the other CHDs have only had a minor procedure or simply have regular follow-up with their cardiologist, and therefore the potential risk of the genetic test affecting insurability is greater.
In this study, parents of probands younger than 16 years old were less likely to endorse genetic test results being used for employment, governmental, and racial discrimination. Younger age has been associated with positive attitudes toward genetic testing in previous studies of adults. However, our study found that this relationship depended upon the age of the child, not the parent. Perhaps, expanded newborn screening and prenatal genetic counseling in the past decade may have dispelled some of the fears related to genetic testing for parents of younger children. Additionally, the passage of the Genetic Information Nondiscrimination Act (GINA) of 2008 prevents health insurance companies from refusing coverage to individuals based on their genetic predisposition to disease. Parents of younger probands may be more aware of this law, particularly if they underwent expanded genetic testing during pregnancy.
Finally, we found no relationship between genetic knowledge and attitudes in our study. Although high genetic knowledge has often been associated with more positive attitudes about genetic testing [Buseh et al., 2014; Jallinoja et al., 2000; Quinlivan et al., 2014; Rose et al., 2005a], a study of Australian adults with Parkinson disease also found no correlation between genetic knowledge and attitudes. The null findings in this study indicate that there may be experiential factors related to attitudes not measured in this study, such as family history of genetic disorders, negative experience with insurance companies, or information gained from discussing genetic testing with others. Additionally, this null finding may be related to the instruments that we utilized perhaps lacking the sensitivity to detect this relationship. Lastly, this cohort could have more homogenous knowledge and/or attitudes since they had already consented to participate in a genetic research study.
This study has several limitations that may affect its generalizability to other populations. Our response rate was somewhat low, which is not atypical of mail surveys. Our sample was largely white, educated, and more affluent compared with other pediatric populations although the LVOT probands are generally comparable to the cardiology clinic population at our institution. It is also important to note that our sample was comprised of parents participating in a genetic research study with their children. Therefore, these parents may have more favorable attitudes towards genetic testing and may have higher genetic knowledge than the general population. Additionally, as we did not differentiate between clinical and research genetic testing, these parents may have been relying on their knowledge of and attitude towards research genetic testing which may not be directly applicable to clinical genetic testing. In regards to clinical genetic testing/evaluation/counseling, we were unable to quantitate the number of participants who had previously participated in these clinical activities. At the time the LVOT probands were initially diagnosed with CHD, the standard practices at out institution did not include genetic testing unless a syndrome was suspected. Thus only a small percentage of probands had undergone genetic testing, evaluation, or counseling.
While the factors associated with high genetic knowledge in this study, income and education, are similar to those found in numerous other studies, the factors affecting attitudes are contradictory, in that we did not find an association with age, education, or genetic knowledge. This suggests that the experiences of parents of children with CHDs may be different from those of the adults in other studies and may be related to factors that have not yet been studied. Therefore, when genetic testing is discussed with parents of children with CHD, it is necessary to probe for their attitudes towards genetic testing and not assume specific attitudes based on their genetic knowledge, age, or education. Genetic counselors are the appropriately trained health care providers to assess genetic knowledge and attitudes and tailor information provision accordingly. While other health care providers may also provide this level of care, they often do not have the time necessary to do so. Additional studies in this and other parental populations are needed to confirm the results of this study, as well as examine other factors that may contribute to parental attitudes towards genetic testing.
Supplementary Material
Figure A. Family Recruitment.
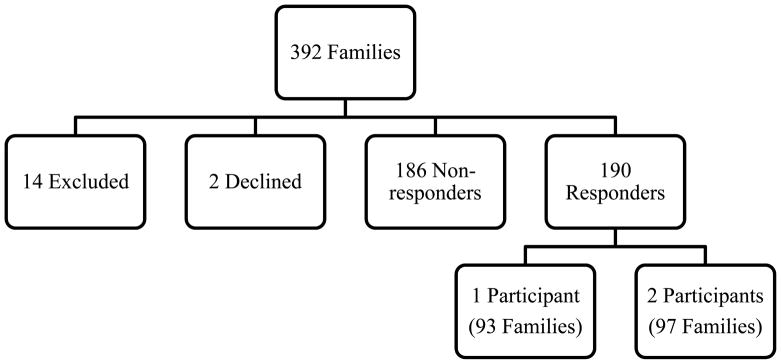
Reasons for exclusion: lack of custody of the proband (2 families), proband deceased (1 family), lack of valid address (11 families).
Acknowledgments
We would like to thank all of the participants of this study who took the time to complete and return our survey. This work has been supported by the 2012 Jane Engelberg Memorial Fellowship, an annual grant from the Engelberg Foundation to the National Society of Genetic Counselors, Inc., the Ohio State University Graduate School’s Alumni Grants for Graduate Research and Scholarship, Nationwide Children’s Hospital, and NIH R01HL090506 and R01HL109758.
References
- Armstrong K, Calzone K, Stopfer J, Fitzgerald G, Coyne J, Weber B. Factors associated with decisions about clinical BRCA1/2 testing. Cancer Epidemiol Biomarkers Prev. 2000;9:1251–4. [PubMed] [Google Scholar]
- Armstrong K, Weber B, Ubel PA, Guerra C, Schwartz JS. Interest in BRCA1/2 testing in a primary care population. Prev Med. 2002;34:590–5. doi: 10.1006/pmed.2002.1022. [DOI] [PubMed] [Google Scholar]
- Bachman KK, Deward SJ, Chrysostomou C, Munoz R, Madan-Khetarpal S. Array CGH as a first-tier test for neonates with congenital heart disease. Cardiol Young. 2013:1–8. doi: 10.1017/S1047951113001868. [DOI] [PubMed] [Google Scholar]
- Brunger JW, Murray GS, O’Riordan M, Matthews AL, Smith RJ, Robin NH. Parental attitudes toward genetic testing for pediatric deafness. Am J Hum Genet. 2000;67:1621–5. doi: 10.1086/316901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buseh A, Kelber S, Millon-Underwood S, Stevens P, Townsend L. Knowledge, group-based medical mistrust, future expectations, and perceived disadvantages of medical genetic testing: perspectives of black african immigrants/refugees. Public Health Genomics. 2014;17:33–42. doi: 10.1159/000356013. [DOI] [PubMed] [Google Scholar]
- Calsbeek H, Morren M, Bensing J, Rijken M. Knowledge and attitudes towards genetic testing: a two year follow-up study in patients with asthma, diabetes mellitus and cardiovascular disease. J Genet Couns. 2007;16:493–504. doi: 10.1007/s10897-006-9085-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell E, Ross LF. Parental attitudes and beliefs regarding the genetic testing of children. Community Genet. 2005;8:94–102. doi: 10.1159/000084777. [DOI] [PubMed] [Google Scholar]
- Connor JA, Hinton RB, Miller EM, Sund KL, Ruschman JG, Ware SM. Genetic testing practices in infants with congenital heart disease. Congenit Heart Dis. 2014;9:158–67. doi: 10.1111/chd.12112. [DOI] [PubMed] [Google Scholar]
- Fitzgerald-Butt SM, Byrne L, Gerhardt CA, Vannatta K, Hoffman TM, McBride KL. Parental knowledge and attitudes toward hypertrophic cardiomyopathy genetic testing. Pediatr Cardiol. 2010;31:195–202. doi: 10.1007/s00246-009-9583-2. [DOI] [PubMed] [Google Scholar]
- Haga SB, Barry WT, Mills R, Ginsburg GS, Svetkey L, Sullivan J, Willard HF. Public knowledge of and attitudes toward genetics and genetic testing. Genet Test Mol Biomarkers. 2013;17:327–35. doi: 10.1089/gtmb.2012.0350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henneman L, Bramsen I, Van Os TA, Reuling IE, Heyerman HG, van der Laag J, van der Ploeg HM, ten Kate LP. Attitudes towards reproductive issues and carrier testing among adult patients and parents of children with cystic fibrosis (CF) Prenat Diagn. 2001;21:1–9. doi: 10.1002/1097-0223(200101)21:1<1::aid-pd967>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- Henneman L, Timmermans DR, Van Der Wal G. Public attitudes toward genetic testing: perceived benefits and objections. Genet Test. 2006;10:139–45. doi: 10.1089/gte.2006.10.139. [DOI] [PubMed] [Google Scholar]
- Ishiyama I, Nagai A, Muto K, Tamakoshi A, Kokado M, Mimura K, Tanzawa T, Yamagata Z. Relationship between public attitudes toward genomic studies related to medicine and their level of genomic literacy in Japan. Am J Med Genet A. 2008;146A:1696–706. doi: 10.1002/ajmg.a.32322. [DOI] [PubMed] [Google Scholar]
- Jallinoja P, Aro AR. Knowledge about genes and heredity among Finns. New Genetics and Society. 1999;18:101–110. [Google Scholar]
- Jallinoja P, Aro AR. Does knowledge make a difference? The association between knowledge about genes and attitudes toward gene tests. J Health Commun. 2000;5:29–39. doi: 10.1080/10810730050019546. [DOI] [PubMed] [Google Scholar]
- Klima J, Fitzgerald-Butt SM, Kelleher KJ, Chisolm DJ, Comstock RD, Ferketich AK, McBride KL. Understanding of informed consent by parents of children enrolled in a genetic biobank. Genet Med. 2014;16:141–8. doi: 10.1038/gim.2013.86. [DOI] [PubMed] [Google Scholar]
- Kocken PL, Theunissen MH, Schonbeck Y, Henneman L, Janssens AC, Detmar SB. Ethnicity, educational level and attitudes contribute to parental intentions about genetic testing for child obesity. J Community Genet. 2013;4:243–50. doi: 10.1007/s12687-013-0137-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lang CW, Stark AP, Acharya K, Ross LF. Maternal knowledge and attitudes about newborn screening for sickle cell disease and cystic fibrosis. Am J Med Genet A. 2009;149A:2424–9. doi: 10.1002/ajmg.a.33074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lerman C, Narod S, Schulman K, Hughes C, Gomez-Caminero A, Bonney G, Gold K, Trock B, Main D, Lynch J, Fulmore C, Snyder C, Lemon SJ, Conway T, Tonin P, Lenoir G, Lynch H. BRCA1 testing in families with hereditary breast-ovarian cancer. A prospective study of patient decision making and outcomes. JAMA. 1996;275:1885–92. [PubMed] [Google Scholar]
- Molster C, Charles T, Samanek A, O’Leary P. Australian study on public knowledge of human genetics and health. Public Health Genomics. 2009;12:84–91. doi: 10.1159/000164684. [DOI] [PubMed] [Google Scholar]
- Morren M, Rijken M, Baanders AN, Bensing J. Perceived genetic knowledge, attitudes towards genetic testing, and the relationship between these among patients with a chronic disease. Patient Educ Couns. 2007;65:197–204. doi: 10.1016/j.pec.2006.07.005. [DOI] [PubMed] [Google Scholar]
- Patenaude AF, Basili L, Fairclough DL, Li FP. Attitudes of 47 mothers of pediatric oncology patients toward genetic testing for cancer predisposition. J Clin Oncol. 1996;14:415–21. doi: 10.1200/JCO.1996.14.2.415. [DOI] [PubMed] [Google Scholar]
- Peters N, Domchek SM, Rose A, Polis R, Stopfer J, Armstrong K. Knowledge, attitudes, and utilization of BRCA1/2 testing among women with early-onset breast cancer. Genet Test. 2005;9:48–53. doi: 10.1089/gte.2005.9.48. [DOI] [PubMed] [Google Scholar]
- Peterson EA, Milliron KJ, Lewis KE, Goold SD, Merajver SD. Health insurance and discrimination concerns and BRCA1/2 testing in a clinic population. Cancer Epidemiol Biomarkers Prev. 2002;11:79–87. [PubMed] [Google Scholar]
- Quinlivan JA, Battikhi Z, Petersen RW. What Factors Impact upon a Woman’s Decision to Undertake Genetic Cancer Testing? Front Oncol. 2014;3:325. doi: 10.3389/fonc.2013.00325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rose A, Peters N, Shea JA, Armstrong K. The association between knowledge and attitudes about genetic testing for cancer risk in the United States. J Health Commun. 2005a;10:309–21. doi: 10.1080/10810730590950039. [DOI] [PubMed] [Google Scholar]
- Rose AL, Peters N, Shea JA, Armstrong K. Attitudes and misconceptions about predictive genetic testing for cancer risk. Community Genet. 2005b;8:145–51. doi: 10.1159/000086757. [DOI] [PubMed] [Google Scholar]
- Sawyer SM, Tully MA, Dovey ME, Colin AA. Reproductive health in males with cystic fibrosis: knowledge, attitudes, and experiences of patients and parents. Pediatr Pulmonol. 1998;25:226–30. doi: 10.1002/(sici)1099-0496(199804)25:4<226::aid-ppul2>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- Skinner D, Sparkman KL, Bailey DB., Jr Screening for Fragile X Syndrome: parent attitudes and perspectives. Genet Med. 2003;5:378–84. doi: 10.1097/01.gim.0000086480.69309.1e. [DOI] [PubMed] [Google Scholar]
- Tercyak KP, Hensley Alford S, Emmons KM, Lipkus IM, Wilfond BS, McBride CM. Parents’ attitudes toward pediatric genetic testing for common disease risk. Pediatrics. 2011;127:e1288–95. doi: 10.1542/peds.2010-0938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Umans-Eckenhausen MA, Oort FJ, Ferenschild KC, Defesche JC, Kastelein JJ, de Haes JC. Parental attitude towards genetic testing for familial hypercholesterolaemia in children. J Med Genet. 2002;39:e49. doi: 10.1136/jmg.39.9.e49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Deyk K, Moons P, Gewillig M, Budts W. Educational and behavioral issues in transitioning from pediatric cardiology to adult-centered health care. Nurs Clin North Am. 2004;39:755–68. doi: 10.1016/j.cnur.2004.07.010. [DOI] [PubMed] [Google Scholar]
- Wang SS, Fridinger F, Sheedy KM, Khoury MJ. Public attitudes regarding the donation and storage of blood specimens for genetic research. Community Genet. 2001;4:18–26. doi: 10.1159/000051152. [DOI] [PubMed] [Google Scholar]
- Willis TA, Potrata B, Ahmed M, Hewison J, Gale R, Downey L, McKibbin M. Understanding of and attitudes to genetic testing for inherited retinal disease: a patient perspective. Br J Ophthalmol. 2013;97:1148–54. doi: 10.1136/bjophthalmol-2013-303434. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.