

Abstract
Erectile dysfunction (ED) is a major complication after radical prostatectomy (RP); however, debate continues regarding the efficacy of penile rehabilitation in the recovery of the postoperative erectile function (EF). This study included a total of 103 consecutive sexually active Japanese men with localized prostate cancer undergoing nerve-sparing RP, and analyzed the postoperative EF, focusing on the significance of penile rehabilitation. In this series, 24 and 79 patients underwent bilateral and unilateral nerve-sparing RPs, respectively, and 10 or 20 mg of vardenafil was administered to 35 patients at least once weekly, who agreed to undergo penile rehabilitation. Twelve months after RP, 48 (46.6%) of the 103 patients were judged to have recovered EF sufficient for sexual intercourse without any assistance. The proportion of patients who recovered EF in those undergoing penile rehabilitation (60.0%) was significantly greater than that in those without penile rehabilitation (38.2%). Of several parameters examined, the preoperative International Index of Erectile Function-5 (IIEF-5) score and nerve-sparing procedure were significantly associated with the postoperative EF recovery rates in patients with and without management by penile rehabilitation, respectively. Furthermore, univariate analysis identified the preoperative IIEF-5 score, nerve-sparing procedure and penile rehabilitation as significant predictors of EF recovery, among which the preoperative IIEF-5 score and nerve-sparing procedure appeared to be independently associated with EF recovery. Considering these findings, despite the lack of independent significance, penile rehabilitation with low-dose vardenafil could exert a beneficial effect on EF recovery in Japanese men following nerve-sparing RP.
Keywords: erectile function, nerve-sparing radical prostatectomy, penile rehabilitation, vardenafil
INTRODUCTION
Radical prostatectomy (RP) is the most widely performed procedure as a curative therapy for patients with clinically localized prostate cancer, and could offer a life expectancy of longer than 10 years to such patients.1 Since the introduction of the prostate-specific antigen test into clinical practice, the diagnosis of prostate cancer is now possible in significantly earlier stages and at younger ages, suggesting that the number of patients, who could be optimal candidates for RP, has markedly increased.1 Accordingly, it is important to minimize the impact of adverse events associated with RP in order to promote a favorable postoperative quality of life.
The incidence of erectile dysfunction (ED) after RP has been reported to vary, ranging between 20% and 90%; however, a significant proportion of patients has been shown to have ED even after bilateral nerve-sparing RP.2,3,4,5 In recent years, the pathophysiology of ED following RP has been well-characterized, and the major causes of postoperative ED are regarded as cavernous nerve injury during surgery and subsequent structural changes in corporal smooth muscle; that is, damage to the cavernous nerves during surgery has been shown to decrease the production of nitric oxide, resulting in the induction of atrophy and fibrosis of the corpus cavernosum accompanying poor corporal oxygenation.6 Furthermore, even if nerve preservation is successfully performed, it is unavoidable that nerve fibers receive a certain level of damage due to dissection, traction and other manipulations during surgery.7 Collectively, these findings suggest that preservation of the erectile function (EF) after RP remains a major challenge for most urological surgeons.
In an attempt to abrogate ED after RP, the concept of penile rehabilitation, defined as the use of any drug or device at or after RP to maximize the recovery of EF, was introduced by Montorsi et al.8 in 1997, who reported the efficacy of penile rehabilitation with the injection of prostaglandin E1 into the corpus cavernosum in a randomized clinical trial. To date, several approaches of penile rehabilitation have been applied, such as vacuum device, prostaglandin E1 injection and phosphodiesterase type 5 inhibitor (PDE5I), of which PDE5I has become the first-line treatment in penile rehabilitation due to the convenience of its oral administration.6,7 In some small randomized trials, significant benefits of penile rehabilitation with PDE5Is after RP have been reported;9,10,11 however, the largest trial, conducted in 2008, failed to show the superiority of the daily use of PDE5I as penile rehabilitation over on-demand treatment with PDE5I in the recovery of EF after RP.12 Therefore, debate continues concerning the significance of postoperative penile rehabilitation, particularly that in Japanese men who are characterized by sexual profiles different from Western populations.13 Considering these findings, we retrospectively analyzed the features of ED in a total of 103 consecutive Japanese men who underwent nerve-sparing RP, focusing on the significance of penile rehabilitation using low-dose vardenafil in the recovery of postoperative EF.
MATERIALS AND METHODS
Patients
At our institution, RP was performed for 451 Japanese patients with clinically localized prostate cancer between January 2009 and March 2011. After excluding patients treated with androgen deprivation and/or radiotherapy from these 451, this study included a total of 103 consecutive patients who were judged to be sexually active with preoperative International Index of Erectile Function-5 (IIEF-5)14 score ≥8 and subsequently underwent either bilateral or unilateral RP. Informed consent for performing the present study was obtained from all patients, and the study design was approved by the Research Ethics Committee of our institution. In this series, the procedures for RP and the nerve-spring technique generally followed the methods described by Walsh et al.15 and the criteria to consider a nerve-sparing procedure were prostate-specific antigen ≤10 ng ml−1, clinically organ-confined tumor and Gleason sum <7.
Evaluation
Preoperative data, including the age at surgery, body mass index, comorbidities (diabetes mellitus, hypertension, hyperlipidemia and cardiovascular disease), serum prostate-specific antigen value and IIEF-5 score, were obtained from all patients. All pathological examinations of resected RP specimens were performed under the guidance of a single pathologist according to the 2002 Tumor, Node and Metastasis classification system. Of the included patients who agreed to receive penile rehabilitation, 10 or 20 mg of vardenafil was administered according to the degree of cardiovascular comorbidities as well as the wishes of the patient at least once weekly within 1 month after RP for 12 months; whereas, the remaining patients did not receive any PDE5Is even as on-demand treatment. Medication compliance of vardenafil was confirmed, when the patients visited the outpatient clinic every 3 months. Twelve months after RP, it was assessed in all patients whether the recovery of EF, defined as the ability to have an erection sufficient for sexual intercourse without any assistance, could be achieved.
Statistical analysis
All statistical analyses were performed using Statview 5.0 software (Abacus Concepts Inc, Berkley, CA, USA). Differences in several parameters according to the postoperative recovery of EF were compared using the chi-square test. Forward stepwise logistic regression analysis was used to determine the association between several parameters and postoperative EF recovery. A value of P < 0.05 was considered significant.
RESULTS
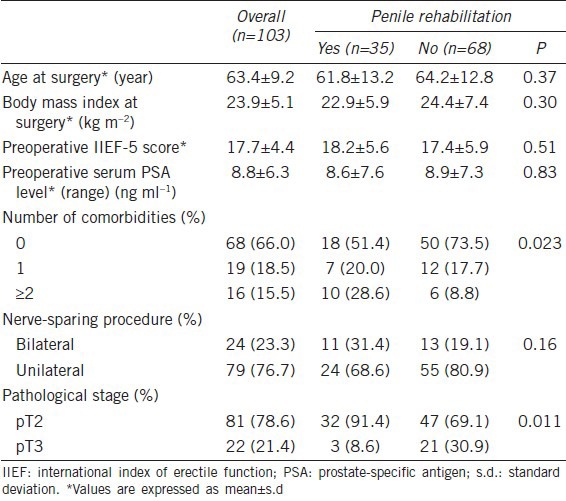
The characteristics of the 103 Japanese patients included in this study are summarized in Table 1. Of the 103 patients, 24 (23.3%) and 79 (76.7%) underwent bilateral and unilateral RPs, respectively, and 35 (34.0%) agreed to undergo penile rehabilitation. Of these 35 patients, 30 and 5 took 10 and 20 mg of vardenafil, respectively, at least once weekly for 12 months, and there was no patient who withdrew from this study because of the side effects associated with vardenafil. There were significant differences in the comorbidities (P = 0.023) and pathological stage (P = 0.011) between patients with and without penile rehabilitation; however, no significant differences were observed in the remaining characteristics examined in this study between these two groups.
Table 1.
Patient characteristics
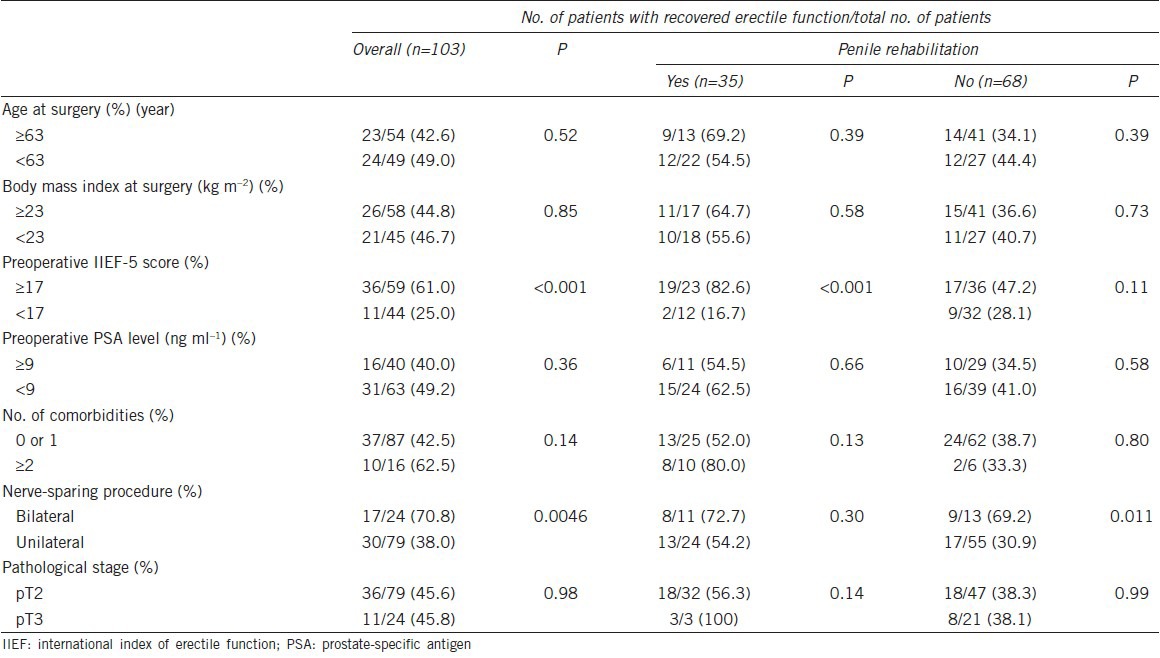
Twelve months after RP, 47 (45.6%) of the 103 patients were judged to have recovered EF sufficient for sexual intercourse without any assistance, consisting of 21 with penile rehabilitation and 26 without penile rehabilitation. Therefore, the proportion of patients who recovered EF in those undergoing penile rehabilitation (60.0%) was significantly greater than that in those without penile rehabilitation (38.2%) (P = 0.036). However, there was no significant difference in the IIEF-5 score 12 months after RP between 35 patients with penile rehabilitation (11.1 ± 7.4) and 68 without penile rehabilitation (9.3 ± 7.7). Table 2 shows the impact of several parameters on EF recovery 12 months after RP. Of several parameters examined, the preoperative IIEF-5 score (P < 0.001; <17 vs ≥17) and nerve-sparing procedure (P = 0.0046; bilateral vs unilateral) were significantly correlated with the postoperative EF recovery rate. When patients were divided into two groups according to management with/without penile rehabilitation, the preoperative IIEF-5 score had a significant effect on the postoperative EF recovery in patients undergoing penile rehabilitation (P < 0.001), while the nerve-sparing procedure was significantly associated with the recovery of EF after RP in patients without penile rehabilitation (P = 0.011).
Table 2.
Recovery of postoperative erectile function according to management with penile rehabilitation
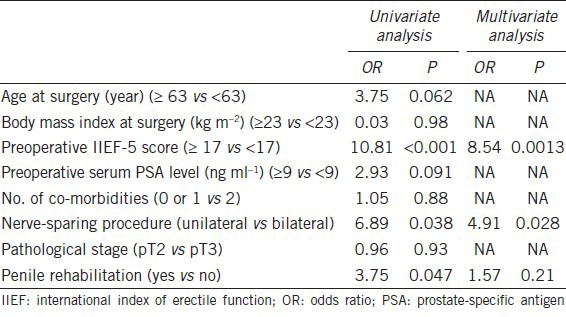
We then conducted uni- and multivariate analysis in order to identify factors predicting the preservation of EF following RP. As shown in Table 3, univariate analysis showed that the preoperative IIEF-5 score (P < 0.001), nerve-sparing procedure (P = 0.038) and penile rehabilitation (P = 0.047) were significantly correlated with the postoperative EF recovery. Furthermore, of these three significant factors, the preoperative IIEF-5 score (P = 0.0013) and nerve-sparing procedure (P = 0.028), but not penile rehabilitation, were identified as independent predictive factors of the recovery of EF after RP.
Table 3.
Uni-and multivariate analyses of several factors predicting postoperative recovery of erectile function
DISCUSSION
RP is the most widely accepted therapeutic option for the treatment of patients with localized prostate cancer; however, it has been well recognized that ED, which adversely influences the postoperative quality of life, frequently occurs in patients undergoing RP even with the nerve-spring technique.1,2,3,4,5 In recent years, the concept of penile rehabilitation was introduced based on the idea that early sexual stimulation and augmented blood flow to the penile tissue would facilitate the return of natural EF as well as the resumption of medically unassisted sexual activity.6,7 Although the mainstay of the current penile rehabilitation strategy is the administration of PDE5I, which has been shown to enhance nocturnal erections and oxygenation of the cavernosal tissues,6,7,9,10,11,12 there has not been a standard approach with respect to the use of PDE5I as penile rehabilitation, particularly in Japanese men whose sexual profile is different from that of Western populations.13 In this study, therefore, we retrospectively reviewed data from a total of 103 consecutive Japanese men who underwent nerve-sparing RP and evaluated the clinical significance of penile rehabilitation with the use of low-dose vardenafil in the recovery of postoperative EF.
In this series, 46.6% of patients were regarded as having EF sufficient for sexual intercourse without any assistance, and the EF recovery rate in patients with penile rehabilitation was significantly higher than that in those without penile rehabilitation. To date, there have been several clinical studies investigating the efficacy of penile rehabilitation using PDE5I; however, the outcomes have not been consistent.9,10,11,12,16 For example, Montorsi et al.12 showed no benefit of daily vardenafil on EF recovery compared with its on-demand use in a randomized trial including 628 patients who were treated with bilateral nerve-sparing RP; however, Briganti et al.16 reported no difference in terms of EF recovery between patients receiving on-demand versus daily PDE5I following bilateral nerve-sparing RP. Such conflicting findings regarding the efficacy of penile rehabilitation with PDE5I could be explained mainly by differences in preoperative parameters, such as the age, EF and comorbidity profile, among these studies; therefore, it is currently recognized that the effectiveness of penile rehabilitation remains ‘unknown’ in humans.17
In this series, the preoperative IIEF-5 score was significantly associated with postoperative EF recovery in patients undergoing penile rehabilitation, while the nerve-sparing procedure significantly affected EF recovery in patients who did not receive penile rehabilitation. These findings suggest that it is difficult to expect the sufficient recovery of EF in patients with a lower preoperative IIEF-5 score even after treatment with penile rehabilitation, and that, if bilateral nerve-sparing RP is performed, the recovery of postoperative EF might be favorable irrespective of management by penile rehabilitation. In fact, it had no significant effects on the recovery rate of EF in patients with a lower preoperative IIEF-5 score whether they received penile rehabilitation or not, and there was no significant difference in EF recovery rates between patients with and without penile rehabilitation following bilateral nerve-sparing RP.
It is potentially useful to identify factors that can be used to predict the recovery of EF following RP. In this series, postoperative EF recovery was significantly associated with the preoperative IIEF-5 score, nerve-sparing procedure and penile rehabilitation, of which the IIEF-5 score and nerve-sparing procedure were identified as independent predictive factors in EF recovery. This outcome is supported by several previous studies.6,7,18,19 For example, Marien et al.18 reported that the age, adult-onset diabetes mellitus and nerve-sparing procedure were independently related to the preservation of postoperative potency in 634 patients undergoing RP, while Gallina et al.19 analyzed the data from 293 patients treated with bilateral nerve-sparing RP, and concluded that younger patients with a good preoperative EF may experience a favorable EF recovery. Considering these findings, it may be possible to accurately predict the recovery of postoperative EF following RP using the preoperative IIEF-5 score and nerve-sparing procedure, irrespective of management by penile rehabilitation.
Currently, there is no established consensus on the most effective strategy of penile rehabilitation using PDE5I, including the timing, duration and regimen, in each patient. In this series, patients, who agreed to undergo penile rehabilitation, were scheduled to take 10 or 20 mg of vardenafil at least once weekly. Such a very low dose of PDE5I for penile rehabilitation was administered for the following reasons: no significant benefit in doubling the daily dose of vardenafil (5–10 mg) to improve the recovery of EF,20 avoidance of discontinuation of the rehabilitation program owing to excessive treatment costs and low sexual drive in Japanese men compared with that of Caucasian men.13 However, it has been well-documented that the prompt initiation of rehabilitation after RP and extension of its duration are associated with favorable EF outcomes;21 therefore, treatment with vardenafil was scheduled to start within 1 month after RP and continue for 12 months. Considering the significantly higher recovery rate of EF in men with penile rehabilitation than those without such rehabilitation in this study, the current rehabilitation schedule could be applied as one of the therapeutic options for Japanese men after nerve-sparing RP who desire to preserve the postoperative EF.
Here, we would like to mention several limitations of this study. Firstly, this was a retrospective study including a relatively small number of patients and non-randomization may result in the application of rehabilitation for men likely to have more active sexual profiles prior to surgery. Secondly, several surgeons were involved in RP in this series and the data from patients undergoing two different surgical procedures (open and laparoscopic RP) were simultaneously analyzed, which may possibly affect the outcomes of this study. Thirdly, the investigation of parameters possibly influencing the recovery of EF, such as serum testosterone, may not be sufficient in this study. In addition, despite the absence of patients who received surgical management for benign prostatic hypertrophy prior to RP in this series, this history may affect the recovery of postoperative EF, while psychological factors are also likely to play an important role in the EF recovery. Finally, it is necessary to consider racial difference in sexual profiles between the Japanese and Western men in order to interpret the findings of this study, since ED and decreased libido were shown to be noted in a greater proportion of Japanese men than in Western men.22 However, previous studies reported that Japanese men were unlikely to perceive their sexual difficulties as a medical issue that requires intervention, and sexual intercourse itself was not always associated with a satisfactory sexual life in the Japanese partners.23,24
In conclusion, this retrospective study included a total of 103 consecutive Japanese men who were judged to be sexually active and subsequently underwent nerve-sparing RP, of whom 35 (34.0%) received penile rehabilitation with low-dose vardenafil. The postoperative recovery rate of EF in men with penile rehabilitation was significantly greater than that in those without penile rehabilitation. Furthermore, despite the lack of independent significance on multivariate analysis, penile rehabilitation appeared to be significantly associated with the sufficient recovery of EF for sexual intercourse. Collectively, these findings suggest that penile rehabilitation using low-dose vardenafil may help preserve the postoperative EF in Japanese men following nerve-sparing RP.
AUTHOR CONTRIBUTION
YN designed the study, analyzed the data and wrote the paper. HM supervised the project and wrote the paper. KC analyzed the data and performed the statistical study. MF supervised the project.
COMPETING INTEREST
The authors have no competing interests.
REFERENCES
- 1.Heidenreich A, Bellmunt J, Bolla M, Joniau S, Mason M, et al. European Association of Urology. EAU guidelines on prostate cancer. Part : screening, diagnosis, and treatment of clinically localised disease. Eur Urol. 2011;59:61–71. doi: 10.1016/j.eururo.2010.10.039. [DOI] [PubMed] [Google Scholar]
- 2.Tal R, Alphs HH, Krebs P, Nelson CJ, Mulhall JP. Erectile function recovery rate after radical prostatectomy: a meta-analysis. J Sex Med. 2009;6:2538–46. doi: 10.1111/j.1743-6109.2009.01351.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Anastasiadis AG, Salomon L, Katz R, Hoznek A, Chopin D, et al. Radical retropubic versus laparoscopic prostatectomy: a prospective comparison of functional outcome. Urology. 2003;62:292–7. doi: 10.1016/s0090-4295(03)00352-2. [DOI] [PubMed] [Google Scholar]
- 4.Goeman L, Salomon L, La De Taille A, Vordos D, Hoznek A, et al. Long-term functional and oncological results after retroperitoneal laparoscopic prostatectomy according to a prospective evaluation of 550 patients. World J Urol. 2006;24:281–8. doi: 10.1007/s00345-006-0054-6. [DOI] [PubMed] [Google Scholar]
- 5.Menon M, Shrivastava A, Kaul S, Badani KK, Fumo M, et al. Vattikuti Institute prostatectomy: contemporary technique and analysis of results. Eur Urol. 2007;51:648–57. doi: 10.1016/j.eururo.2006.10.055. [DOI] [PubMed] [Google Scholar]
- 6.McCullough AR. Rehabilitation of erectile function following radical prostatectomy. Asian J Androl. 2008;10:61–74. doi: 10.1111/j.1745-7262.2008.00366.x. [DOI] [PubMed] [Google Scholar]
- 7.Kaiho Y, Yamashita S, Arai Y. Optimization of sexual function outcome after radical prostatectomy using phosphodiesterase type 5 inhibitors. Int J Urol. 2013;20:285–9. doi: 10.1111/iju.12071. [DOI] [PubMed] [Google Scholar]
- 8.Montorsi F, Guazzoni G, Strambi LF, Da Pozzo LF, Nava L, et al. Recovery of spontaneous erectile function after nerve-sparing radical retropubic prostatectomy with and without early intracavernous injections of alprostadil: results of a prospective, randomized trial. J Urol. 1997;158:1408–10. [PubMed] [Google Scholar]
- 9.Bannowsky A, Schulze H, van der Horst C, Hautmann S, Jünemann KP. Recovery of erectile function after nerve-sparing radical prostatectomy: improvement with nightly low-dose sildenafil. BJU Int. 2008;101:1279–83. doi: 10.1111/j.1464-410X.2008.07515.x. [DOI] [PubMed] [Google Scholar]
- 10.Padma-Nathan H, McCullough AR, Levine LA, Lipshultz LI, Siegel R, et al. Study Group. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res. 2008;20:479–86. doi: 10.1038/ijir.2008.33. [DOI] [PubMed] [Google Scholar]
- 11.McCullough AR, Hellstrom WG, Wang R, Lepor H, Wagner KR, et al. Recovery of erectile function after nerve sparing radical prostatectomy and penile rehabilitation with nightly intraurethral alprostadil versus sildenafil citrate. J Urol. 2010;183:2451–6. doi: 10.1016/j.juro.2010.01.062. [DOI] [PubMed] [Google Scholar]
- 12.Montorsi F, Brock G, Lee J, Shapiro J, Van Poppel H, et al. Effect of nightly versus on-demand vardenafil on recovery of erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol. 2008;54:924–31. doi: 10.1016/j.eururo.2008.06.083. [DOI] [PubMed] [Google Scholar]
- 13.Namiki S, Carlile RG, Namiki TS, Fukagai T, Takegami M, et al. Racial differences in sexuality profiles among American, Japanese, and Japanese American men with localized prostate cancer. J Sex Med. 2011;8:2625–31. doi: 10.1111/j.1743-6109.2011.02362.x. [DOI] [PubMed] [Google Scholar]
- 14.Rhoden EL, Telöken C, Sogari PR, Vargas Souto CA. The use of the simplified International Index of Erectile Function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunction. Int J Impot Res. 2002;14:245–50. doi: 10.1038/sj.ijir.3900859. [DOI] [PubMed] [Google Scholar]
- 15.Walsh PC. The discovery of the cavernous nerves and development of nerve sparing radical retropubic prostatectomy. J Urol. 2007;177:1632–5. doi: 10.1016/j.juro.2007.01.012. [DOI] [PubMed] [Google Scholar]
- 16.Briganti A, Di Trapani E, Abdollah F, Gallina A, Suardi N, et al. Choosing the best candidates for penile rehabilitation after bilateral nerve-sparing radical prostatectomy. J Sex Med. 2012;9:608–17. doi: 10.1111/j.1743-6109.2011.02580.x. [DOI] [PubMed] [Google Scholar]
- 17.Hatzimouratidis K, Burnett AL, Hatzichristou D, McCullough AR, Montorsi F, et al. Phosphodiesterase type 5 inhibitors in postprostatectomy erectile dysfunction: a critical analysis of the basic science rationale and clinical application. Eur Urol. 2009;55:334–47. doi: 10.1016/j.eururo.2008.10.028. [DOI] [PubMed] [Google Scholar]
- 18.Marien T, Sankin A, Lepor H. Factors predicting preservation of erectile function in men undergoing open radical retropubic prostatectomy. J Urol. 2009;181:1817–22. doi: 10.1016/j.juro.2008.11.105. [DOI] [PubMed] [Google Scholar]
- 19.Gallina A, Ferrari M, Suardi N, Capitanio U, Abdollah F, et al. Erectile function outcome after bilateral nerve sparing radical prostatectomy: which patients may be left untreated? J Sex Med. 2012;9:903–8. doi: 10.1111/j.1743-6109.2011.02622.x. [DOI] [PubMed] [Google Scholar]
- 20.Bannowsky A, van Ahlen H, Loch T. Increasing the dose of vardenafil on a daily basis does not improve erectile function after unilateral nerve-sparing radical prostatectomy. J Sex Med. 2012;9:1448–53. doi: 10.1111/j.1743-6109.2012.02705.x. [DOI] [PubMed] [Google Scholar]
- 21.Mulhall JP, Parker M, Waters BW, Flanigan R. The timing of penile rehabilitation after bilateral nerve-sparing radical prostatectomy affects the recovery of erectile function. BJU Int. 2010;105:37–41. doi: 10.1111/j.1464-410X.2009.08775.x. [DOI] [PubMed] [Google Scholar]
- 22.Namiki S, Kwan L, Kagawa-Singer M, Saito S, Terai A, et al. Sexual function reported by Japanese and American men. J Urol. 2008;179:245–9. doi: 10.1016/j.juro.2007.08.164. [DOI] [PubMed] [Google Scholar]
- 23.Moreira ED, Jr, Brock G, Glasser DB, Nicolosi A, Laumann EO, et al. GSSAB Investigators’ Group. Help-seeking behaviour for sexual problems: the global study of sexual attitudes and behaviors. Int J Clin Pract. 2005;59:6–16. doi: 10.1111/j.1742-1241.2005.00382.x. [DOI] [PubMed] [Google Scholar]
- 24.Hisasue S, Kumamoto Y, Sato Y, Masumori N, Horita H, et al. Prevalence of female sexual dysfunction symptoms and its relationship to quality of life: a Japanese female cohort study. Urology. 2005;65:143–8. doi: 10.1016/j.urology.2004.08.003. [DOI] [PubMed] [Google Scholar]