

Abstract
Background:
There is growing concern among policy makers with respect to alarming growth in smoking prevalence among women in the developing countries.
Methods:
Using disaggregated data from five nationally representative surveys: Global Adult Tobacco Survey 2010, National Family Health Survey-III (NFHS-III) 2004–2005, NFHS-II 1998-1999, National Sample Survey (NSS) 52nd Round 1995–1996, NSS 50th Round 1993-1994 we analysed female smoking trend from 1993-2009. Tobacco use among females was monitored for almost two decades focusing on gender, literacy, and state-specific trends among respondents aged >15 years.
Results:
Smoking use among women has doubled from 1.4% to 2.9% (P < 0.001) during the period 2005-2010. The prevalence of smoking increased with decrease in per capita State Gross Domestic Product and literacy status for both men and women.
Conclusion:
As the overall smoking prevalence grows, female smoking is growing at a faster rate than smoking among males, which is an emerging concern for tobacco control in India and requires the attention of policymakers.
Keywords: Female smoking, India, Global Adult Tobacco Survey
Introduction
Tobacco use is the leading preventable cause of death and disease in the world taking more than five million lives each year.[1] Over the past couple of decades, there has been an added concern among the policy makers and implementers regarding the alarming rise in smoking prevalence among women in both developed and developing countries.[2] Unless sustained and effective initiatives are implemented the prevalence of female smoking is likely to rise to 20% by 2025.[3] WHO Framework Convention on Tobacco Control has emphasized the need for gender specific tobacco control strategies in their tobacco control programs. Effective tobacco control policies will lead to significant gains in the form of improvements in public health, reduced morbidity and mortality, gains in terms of productivity, and a healthier and more active workforce, more so with a gender equity lens.[4]
Smoking trend inform policy makers to monitor the effectiveness of existing policy and help design future tobacco control policies. Nationally representative surveys have assessed tobacco prevalence and pattern of use at different periods of time over the past three decades. This study attempts to review nationwide surveys on tobacco use prevalence and estimate the trend across gender, literacy, and regions.
Methods
Nationally representative surveys have collected data on socio-demographic indicators, reproductive health, health services and other aspects of health, which include tobacco use. Estimates from such nationwide surveys at different time periods (during 1993–2009) were analyzed to monitor the trend of female smoking. Tobacco use was also studied across literacy levels, and per capita Gross Domestic Product (GDP).[5]
Sources of data
The estimates of tobacco consumption were obtained from five surveys, namely Global Adult Tobacco Survey (GATS) 2010, National Family Health Survey-III (NFHS-III) 2004–2005, NFHS-II 1998-1999, National Sample Survey (NSS) 52nd Round 1995-1996, NSS 50th Round 1993–1994. The trends of prevalence and use of tobacco was estimated according to gender, literacy and states among respondents aged >15years. Literacy status was categorized into four grades: No formal schooling (illiterate), less than primary education (<5years), primary, but less than secondary (5-9years), secondary and above (≥10years). All the surveys employed multistage stratified sampling methodology with 3-stage sampling in urban and 2-stage sampling in rural areas. The response rates of GATS, NFHS-III and NFHS-II were 92%, 98% and 96% respectively.
Global Adult Tobacco Survey (2010)
Global Adult Tobacco Survey (2010) was carried out in all 29 states of the country and two Union Territories of Chandigarh and Pondicherry among persons aged 15 and above. A total of 69,296 respondents participated in the survey.
National Family Health Survey-III
National Family Health Survey-III (2005–2006) interviewed a nationally representative sample of 109,041 households, 124,385 women aged 15-49 and 74,369 men aged 15-54 in all 29 states of India.
National Family Health Survey-II
National Family Health Survey-II (1998–1999) covered a representative sample of over 91,000 ever-married women age 15-49 years across 26 states of India.
Results
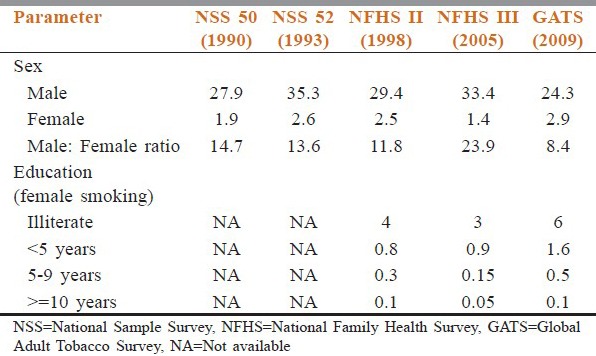
The survey estimates show that smoking prevalence among males over the last two decades has an overall declining trend with a significant decline (P < 0.001) in smoking prevalence (33.4-24.3%) during the period 2005–2009. However, an overall rising trend of female smoking was observed with a significant (P < 0.001) rise (1.4–2.9%) during the period 2005–2009. The male: female smoking ratio dipped significantly during the period 2005-2009 due to the twin effect of rise in female smoking and decline in male smoking [Table 1].
Table 1.
Current smoking trends according to sex and literacy during 1993-2009
Evidence in this study suggests that smoking prevalence decreases with increase in per capita GDP irrespective of gender status [Figure 1]. According to GATS (2009-10), the states categorized among the highest per capita GDP states such as Delhi, Goa had low female smoking prevalence whereas other states with high per capita GDP like Maharashtra and Kerala (near) zero prevalence of female smoking. The currently smoking females in low per capita GDP states of Mizoram, Sikkim and Nagaland were much higher at 19%, 15.9%, and 12.4% respectively. In NFHS-III (2005), similar pattern was observed wherein the affluent states such as Tamil Nadu, Kerala, and Karnataka recorded near zero female smoking prevalence. Mizoram, with low per capita GDP had the highest prevalence of smoking among women with 16.1%.
Figure 1.
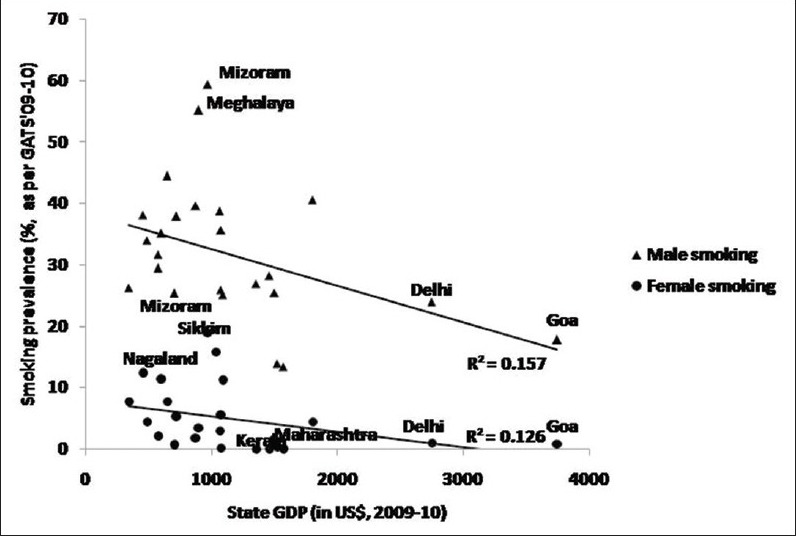
Relationship between State Gross Domestic Product and prevalence of current smoking
Figure 2 shows the state-wise trend of female smoking, wherein, there had been an increasing trend of female smoking across all states since the year 2005 (except states of Punjab, Maharashtra, and Kerala). Overall, the north-eastern states such as Mizoram, Meghalaya, Sikkim, and Manipur have always had high female smoking rates. On the other hand, southern states such as Kerala, Tamil Nadu, and Maharashtra have consistently remained on the lowest side of the range with near zero prevalence.
Figure 2.
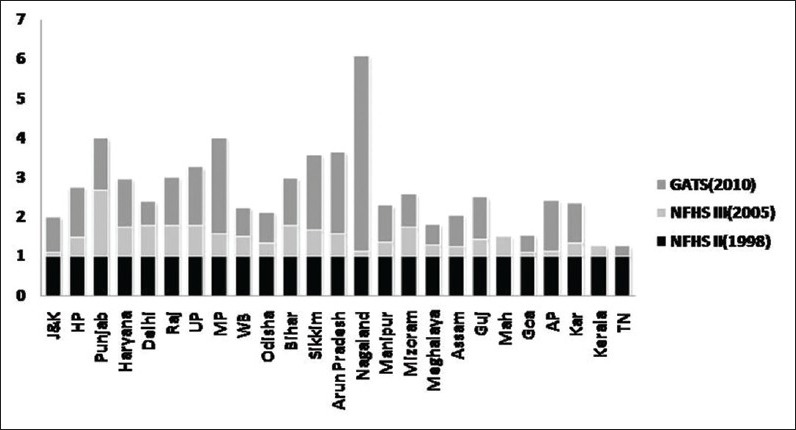
Interstate comparison of current female smoking across three nationwide surveys. Taking prevalence of smoking during 1998–1999 as one unit (baseline value), prevalence of smoking during 2005 and 2010 were estimated. The length of each color component in a bar is shown to be directly proportional to the prevalence of current smoking
The prevalence of current smoking among females was much higher among those who are illiterate, which decreased with increasing years of schooling at different time periods. According to NFHS III, the prevalence of female smoking nosedived from 3% to a mere 0.05% as we moved across various levels of literacy from illiterate to >10 years of schooling [Table 1].
States with lower female literacy rates (lower than national average) such as Jammu and Kashmir, Uttar Pradesh (UP), Arunachal Pradesh, Manipur, and Nagaland have high prevalence of current female smoking, whereas states such as Kerala, Goa, Maharashtra, and Tamil Nadu, which have high female literacy rates (higher than national average) have lower female smoking rates. However, there are exceptions like Mizoram and Sikkim, which have high smoking prevalence in spite of higher literacy rates.
Discussion
Female smoking has enormous consequences not only for women's health, and economic wellbeing, but also for their families. Apart from the health risks that women share with men, women face additional hazards like adverse pregnancy outcomes, female specific cancers such as cancer of breast, cervix, and increased cardiovascular risks.[6] An increasing prevalence of smoking among women is a matter of serious public health concern.
The analysis of the present study finds that there is significant rise in female smoking in India during the period 1993-2009. Similar rising trend of female smoking has been observed among young women in Western Pacific Region countries and Singapore.[7,8] In another study, the authors found that young, elite women in China have started to smoke in greater numbers than their less affluent peers following the introduction of two women's cigarette brands.[9] Even in Vietnam, there was concern about potential uptake of tobacco use among women.[8] In Japan, there was a sharp rise in the smoking prevalence among women aged 20–29 from 12% to 22% over the last three decades.[10] WHO in its report on regional analysis of women and tobacco has documented that despite the alarming signals from several South-East Asian countries, there has been no mention of gender in their tobacco control policies.[8]
These studies echo the facts that while the epidemic of tobacco use among men is in declining phase albeit slowly, the prevalence of use among women is increasing. The findings of the study goes in consonance with Lopez et al.'s (1994) descriptive model of the tobacco epidemic, which predicts that the female-to-male ratio in smoking prevalence will rise in many low-and-middle-income countries where females currently smoke at much lower rates than males.[11]
Greater female autonomy historically has been linked to smoking uptake among Western women[12] pushing predictions of similar patterns in developing countries. One study finds that a proportionate increase is observed in women's smoking rates with greater empowerment of women in several countries.[13] There are various factors which interplay to explain the rise in female smoking in India over the past decade or so. The growing spending power among women[3] and weakening of social and cultural constraints due to globalization and economic transition are to name a few.
The current focus of tobacco industry to target women to become smokers is through seductive but false images of vitality, slimness, modernity, emancipation, sophistication, and sexual allure.[14] A study in Russia has documented a two-fold rise in the prevalence of smoking among women following aggressive women focused tobacco advertising campaigns during the economic transition in Russia.[15] Thus, the ever growing expenditure on new marketing strategies for promoting tobacco use, primarily focused toward the women and youths puts them at an increased risk.
The results of this study suggest with lower levels of literacy smoking prevalence increases irrespective of gender supported by other studies in India which showed high tobacco consumption among poor, less educated populations.[16,17] Studies in other South-East Asian countries like Bangladesh and Nepal have also shown that smoking prevalence was much higher among illiterate female than those who are educated.[17] Disaggregated analysis of the state-wise smoking rates presented here shows that states having high per capita GDP and high literacy rates such as Kerala, Maharashtra, Tamil Nadu, and Punjab have very low female smoking rates, whereas females in states with low per capita GDP and literacy such as Bihar, UP, Nagaland, Manipur, and other North Indian states smoke more.
Women's smoking prevalence is further projected to rise in many low-and-middle-income countries. This finds support from the findings of the Global Youth Tobacco Survey, which show that worldwide smoking rates among boys and girls resemble each other more than smoking rates among adult women and men.[13]
Over the last three to four decades, we also have success stories from developing nations in the area of tobacco legislation with special focus on women. Thailand has its own program known as “Thai women do not smoke,” which aimed at preserving the non-smoking norm among Thai women. The project focuses on the effects of smoking on beauty and on children's health and promotes the view that smart women do not smoke.[17] Many other initiatives across the globe have been proved to be successful to counteract the tobacco industry's techniques to lure women into the habit of smoking cigarettes. However, gender-blind policies have compounded the problem of ever increasing rates of female smoking in India. Policymakers have to recognize female smoking epidemic as a threat to global public health.
Limitations
The surveys compared in this study followed a more or less similar methodology in terms of sampling, representativeness, and study subjects. However, the only limitation is that NFHS-II had household female informant as the respondent, whereas in other surveys all the household members were interviewed. This may underestimate the prevalence data, which has been calculated by Rani et al. to be 5% and 0.5% for smoking among men and women. However, this underestimation is not going to undermine the significant findings in the present study.[16] These surveys being cross-sectional provide limited scope for causal inference. NFHS also does not provide detailed data by type or volume of tobacco. Finally, NFHS is a reproductive health survey where women in the ages of 15-49 years are sampled which might cause lead to social desirability bias. But this might only underestimate the smoking behaviour among women. Although current smoking was compared across all three surveys, comparability of surveys becomes difficult due to varied definitions of the question of interest.
Conclusion
The findings of this study clearly provide a basis to institute gender based tobacco control policies to stop the rise in women's smoking rates.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.World Health Organization. Geneva: World Health Organization; 2008. WHO Report on the Global Tobacco Epidemic 2008: The MPOWER Package. [Google Scholar]
- 2.Amos A. Women and smoking. Br Med Bull. 1996;52:74–89. doi: 10.1093/oxfordjournals.bmb.a011534. [DOI] [PubMed] [Google Scholar]
- 3.Mackay J, Amos A. Women and tobacco. Respirology. 2003;8:123–30. doi: 10.1046/j.1440-1843.2003.00464.x. [DOI] [PubMed] [Google Scholar]
- 4.Samet JM, Yoon SY. Geneva: World Health Organization; 2010. Gender, Women, and the Tobacco Epidemic. [Google Scholar]
- 5.Per capita State Gross Domestic Product. Directorate of Economics and Statistics, Government of India. [Last accessed on 2014 Jul 03]. Available from: http://mospi.nic.in/Mospi_New/upload/State_wise_SDP_2004.05_14mar12.pdf .
- 6.Health Consequences of Tobacco Use Among Women. Chapter 3. Atlanta (GA): Centers for Disease Control and Prevention (US); 2001. Mar, Office on Smoking and Health (US). Women and Smoking: A Report of the Surgeon General. Available from: http://www.ncbi.nlm.nih.gov/books/NBK44312 . [PubMed] [Google Scholar]
- 7.Morrow M, Ngoc DH, Hoang TT, Trinh TH. Smoking and young women in Vietnam: The influence of normative gender roles. Soc Sci Med. 2002;55:681–90. doi: 10.1016/s0277-9536(01)00310-0. [DOI] [PubMed] [Google Scholar]
- 8.Morrow M, Barraclough S. Tobacco control and gender in south-east Asia. Part II: Singapore and Vietnam. Health Promot Int. 2003;18:373–80. doi: 10.1093/heapro/dag403. [DOI] [PubMed] [Google Scholar]
- 9.Kaufman NJ, Nichter M. The marketing of tobacco to women: Global perspectives. In: Samet J, Yoon SY, editors. Women and the Tobacco Epidemic: Challenges for the 21st Century. Geneva: World Health Organization; 2001. pp. 69–98. [Google Scholar]
- 10.Tominaga S. Leaving the pack behind: Tobacco control in Japan. Paper Presented at the WHO Kobe Centre, Tobacco or Health: It's Time to Leave the Pack Behind. Report of the International Symposium, Kobe; 1999 [Google Scholar]
- 11.Lopez AD, Collishaw NA, Piha T. A descriptive model of the cigarette epidemic in developed countries. Tob Control. 1994;3:242–7. [Google Scholar]
- 12.Worth R. Making it uncool: Ways to prevent teenage smoking. Washington Mon. 1999;31:8–12. [Google Scholar]
- 13.Hitchman SC, Fong GT. Gender empowerment and female-to-male smoking prevalence ratios. Bull World Health Organ. 2011;89:195–202. doi: 10.2471/BLT.10.079905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Geneva: World Health Organization; 2007. [Last accessed on 2014 Jul 3]. Gender and tobacco control: A policy brief. Available from: http://www.who.int/tobacco/resources/publications/general/policy_brief.pdf . [Google Scholar]
- 15.Perlman F, Bobak M, Gilmore A, McKee M. Trends in the prevalence of smoking in Russia during the transition to a market economy. Tob Control. 2007;16:299–305. doi: 10.1136/tc.2006.019455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rani M, Bonu S, Jha P, Nguyen SN, Jamjoum L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob Control. 2003;12:e4. doi: 10.1136/tc.12.4.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gupta R. Smoking, educational status and health inequity in India. Indian J Med Res. 2006;124:15–22. [PubMed] [Google Scholar]