

Abstract
Background:
The ultimate goal of periodontal therapy entails regeneration of the periodontal tissues lost as a consequence of periodontitis. Predictable correction of vertical osseous defects has however posed as a constant therapeutic challenge. The aim of our present study is to evaluate the relative efficacy of demineralized freeze-dried bone allograft (DFDBA) vs anorganic bovine bone xenograft (ABBX) in the treatment of human infrabony periodontal defects.
Materials and Methods:
15 patients with 30 bilaterally symmetrical defect sites in either of the arches, in the age group of 25-50 years were selected as part of split-mouth study design. Defect-A (right side) was grafted with DFDBA while Defect-B (left side) was grafted with ABBX. Various clinical and radiographic parameters viz. probing depth(PD), clinical attachment level(CAL) and linear bone fill were recorded preoperatively, 12- & 24-weeks postoperatively.
Results:
Both defect-A & defect-B sites exhibited a highly significant reduction in probing depth, and gain in clinical attachment level and linear bone fill at 12-weeks & at the end of 24-weeks. Comparative evaluation between the study groups revealed a statistically non-significant reduction in probing depth (P<0.1) and mean gain in linear bone fill (P<0.1). However, there was a statistically significant gain in clinical attachment level (P<0.05) in Defect-A (CD=0.356) as compared to Defect-B (CD=0.346).
Conclusions:
Within the limits of this study, both the materials viz. ABBX and DFDBA are beneficial for the treatment of periodontal infrabony defects. Both the materials were found to be equally effective in all respects except the gain in attachment level, which was found to be more with DFDBA. Long-term studies are suggested to evaluate further the relative efficacy of the two grafts.
Keywords: Anorganic bovine bone xenograft, bone grafts, demineralized freeze-dried bone allograft, infrabony defects, regeneration
INTRODUCTION
Periodontal disease, one of the most common reasons for the loss of teeth, results in the extension of the inflammation from the marginal gingiva into the supporting periodontal tissues viz. periodontal ligament, cementum, and alveolar bone. The consequent destruction of the alveolar bone is ultimately responsible for the exfoliation of the tooth. Hence, the aim of the periodontal therapy is to regenerate the lost supporting tissues thus requiring the formation of new cementum, deposition of bone, insertion of functionally oriented new connective tissue fibers in the newly formed bone and cementum, and organization of a competent gingival unit.[1]
These days clinical periodontal research focuses on the utilization of bone grafts,[2,3,4] the principles of guided tissue regeneration[5] or combination of the both[6] to achieve regeneration. Until date, the materials demonstrated to meet the histologic criteria for periodontal regeneration are autografts, allografts, anorganic bovine bone xenografts (ABBXs), and xenogenic enamel matrix derivative.[2]
Although osseous autografts have a laudable record for many applications in dentistry, yet due to the morbidity associated with them, allografts have been introduced as an alternative among which demineralized freeze-dried bone allograft (DFDBA) has shown promising results due to its availability, safety, osteoinductive, and osteoconductive properties.
Results of human histologic studies have shown that DFDBA can successfully regenerate bone as well as cementum in the treatment of periodontal defects,[7,8] and also regenerate bone around implants,[9] in localized alveolar ridge augmentation procedures, in nonorthoptic sites viz., muscles and connective tissues,[10] in sinus elevation[11] etc.
At the present times xenograft, obtained from a donor of different species, is another option for use as a bone graft material. ABBX is a natural microporous hydroxyapatite skeleton,[12] which is similar in structure to human cancellous bone. This material enhances the bone formation due to its osteoconductive properties[3,13] and undergoes remodeling during a slow resorption process.[3] Although it lacks osteoinductive activity, in many studies it has been reported to facilitate osteogenesis in the presence of osteogenic precursor cells.[14]
Both these materials viz., DFDBA and ABBX, have shown good results when tried individually, but the literature is still deficient in their comparative studies. In this study, an attempt has been made to evaluate and compare clinically and radiographically, the efficacy of DFDBA and ABBX in the treatment of periodontal osseous defects [Figure 1].
Figure 1.

Regenerative bone graft materials employed
MATERIALS AND METHODS
Study population
A split mouth study was designed with an age group of 25-50 years. A total of 15 patients were selected from among the patients visiting the Department of Periodontology, Punjab Government Dental College and Hospital, Amritsar. The criteria for the selection of the patients were as follows:
Presence of almost identical bilateral infrabony defects in relation to the posterior teeth, of either the maxilla or the mandible, as determined by clinical and radiological evaluation
Patients who were not suffering from any systemic disease
Patients who had no known history of allergy
Patients who were nonsmokers.
After an explanation of the proposed study criteria, including alternative treatments and potential risks and benefits, the participants were asked to sign a consent form prior to surgery. The study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2000 after receiving clearance from the ethical clearance committee of the institute.
Materials
DFDBA: In this study was prepared, according to a standardized technique,[15] from the parts of long bones obtained from the Department of Orthopedics, Government Medical College, Amritsar and stored in 10% formaldehyde solution until the time of preparation. The cortical portion of the bone was selected for the same since it is known to contain more bone morphogenetic proteins (BMPs) in comparison to the cancellous bone[16] (particle size 0.3-1 mm)
ABBX: Bio-Oss® spongiosa granules (geistlich Pharma AG, bahnhofstrasse 40CH-6110, Wolhusen, Switzerland) (particle size 0.25-1 mm, Geistlich Biomaterials) was used.
Methods
Preoperative
Routine laboratory investigations were carried out for each patient following which oral prophylaxis was performed and the patient was instructed to adopt meticulous home care measures to control the dental plaque. The oral hygiene status was reviewed by disclosing the presence or absence of tooth accumulated material at weekly intervals until he/she could maintain a satisfactory level of oral hygiene. Occlusal adjustment was performed, if trauma from occlusion was diagnosed
Radiographs by standardized technique (using a millimeter grid along with the X-ray film and employing long cone/paralleling technique) were taken preoperatively to ascertain the depth of the infrabony defect [Figures 2a 3a]. The defect depth was measured from a fixed reference point (the adjacent cuspal tip) to the most apical point of the base of the defect
Preoperative assessment of clinical parameters viz., probing depth (PD), and clinical attachment level (CAL) was performed using stents, immediately prior to surgery.
Figure 2.
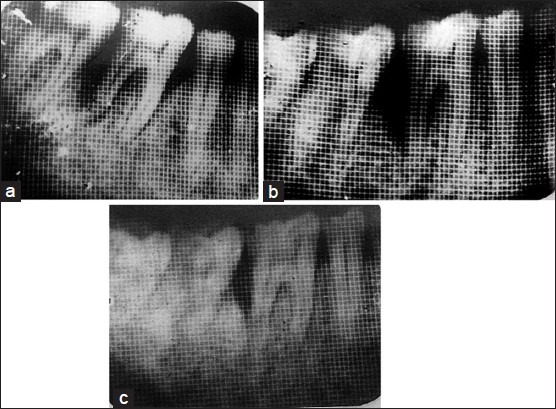
(a) Radiographic comparison of osseous defect fill at DFDBA site at Baseline, (b) 12 weeks post-operative, (c) 24 weeks post-operative
Figure 3.
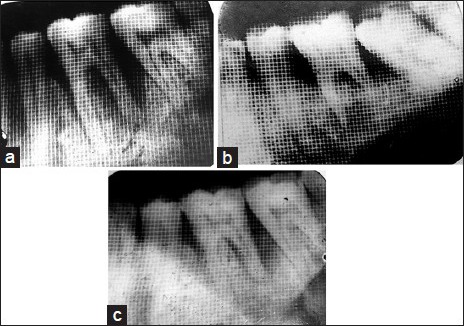
(a) Radiographic comparison of osseous defect fill at ABBX site at Baseline (b) 12 weeks post-operative (c) 24 weeks post-operative
Operative
The identical infrabony defects were designated as “defect-A” for right infrabony defect [Figure 4] and “defect-B” for left infrabony defect [Figure 5]. Full thickness mucoperiosteal flaps were raised to gain access to the infrabony defects. Following the root planning and debridement of the defect sites [Figures 6 and 7], DFDBA was placed in “defect-A” [Figure 8] and ABBX was placed in “defect-B” [Figure 9] and interrupted interdental sutures were given [Figures 10 and 11].
Figure 4.

Crevicular incision at the surgical site (Defect-A)
Figure 5.

Crevicular incision at the contra-lateral surgical site (Defect-B)
Figure 6.

Osseous defect subsequent to debridement (Defect-A)
Figure 7.

Osseous defect subsequent to debridement (Defect-B)
Figure 8.

Following the placement of demineralized freeze-dried bone allograft
Figure 9.

Following the placement of anorganic bovine bone xenograft
Figure 10.

Surgical site after suturing (Defect-A)
Figure 11.

Surgical site after suturing (Defect-B)
Postoperative
Immediate postoperatively, the patients were prescribed antibiotic therapy along with an antiinflammatory agent. Routine written and oral postoperative care instructions were given to each patient. Sutures were removed 1 week after the surgery. Postsurgical examination and supragingival cleaning of the surgical site was done. The patients were recalled at monthly intervals for oral hygiene assessments by disclosing the presence/absence of tooth accumulated materials and to carry out supragingival scaling. Postoperative assessments viz. PD, attachment level and radiographs for calculating the linear bone fill were performed at 12 and 24 weeks postoperatively. The observations, thus, made were statistically analyzed.
RESULTS
It was observed that both the materials were well-tolerated by all the patients with no adverse tissue reaction, infection or delayed healing reported during the course of the study.
The mean preoperative and postoperative PD, CAL and linear bone fill at baseline, 12 weeks and 24 weeks postoperative for both defect-A and defect-B are enumerated in Table 1.
Table 1.
Mean PD, CAL and infrabony defect depth for defect-A (DFDBA) and defect-B (ABBX) in mm

The mean reduction or gain in postoperative PD, CAL and linear bone fill for both defect-A and defect-B after 12 weeks and 24 weeks postoperatively [Figures 2b, c and 3b, c] and between 12 weeks and 24 weeks postoperatively are summarized in Table 2.
Table 2.
Mean reduction in PD and gain in CAL and linear bone fill for defect-A (DFDBA) and defect-B (ABBX) in mm

A comparison of defect-A and defect-B for mean reduction in PD, mean gain in CAL and mean linear bone fill is presented in Table 3.
Table 3.
Comparison of defect-A (DFDBA) and defect-B (ABBX) for the chosen parameters in mm

Student's t-test (for paired samples) was applied to statistically evaluate the data since the observation at the two points in time were expected to be closely related to each other. A statistically significant reduction in PD with both DFDBA and ABBX was observed at all 3 time-intervals. In addition, a significant gain in CAL and linear bone fill was seen with DFDBA alone at all 3 time-intervals.
In order to examine whether the improvement in PD, CAL and linear bone fill during the three successive points in time for the two materials were of similar nature or not, the data were subjected to two-way analysis of variance (ANOVA). The patients were regarded as replicates and the combination of materials and time-intervals as treatments and results thus obtained have been tabulated in Tables 4-6.
Table 4.
Two-way ANOVA table for comparing reduction in PD in respect of defect-A (DFDBA) and defect-B (ABBX)

Table 6.
Two-way ANOVA table for comparing gain in linear bone fill in respect of defect-A (DFDBA) and defect-B (ABBX)

Table 5.
Two-way ANOVA table for comparing gain in attachment level in respect of defect-A (DFDBA) and defect-B (ABBX)

A break-up of the variability between treatment combinations into three components; that is, due to (a) The materials used in the defects, (b) the time-intervals and (c) the interaction between materials and time-intervals revealed that the difference in between the materials with respect to the reduction in PD was not significant. An almost similar pattern of reduction in PD was experienced in both the defects. The computed values of critical difference also reveal a statistically significant reduction in PD during all time-intervals as depicted in Table 7.
Table 7.
Mean values of reduction in PD in mm

The ANOVA approach displayed a statistically significant difference in the results between the materials used with respect to CAL, though the interaction between individual materials and time-intervals was nonsignificant. The observed values of critical difference revealed that over the entire period of the study span, the material used in defect-A was significantly superior to that for defect-B [Table 8].
Table 8.
Mean values of gain in attachment level in mm

The results of the ANOVA approach showed that the difference between the materials used was not significant. However, the gain in linear bone fill during different time-intervals differed significantly at 1% probability level. The critical difference values express an almost uniform rate of linear bone fill over the entire study span as depicted in Table 9.
Table 9.
Mean values of gain in linear bone fill in mm

DISCUSSION
Periodontal disease occasionally involves the alteration in the morphological features of the bone, which may include the reduction in bone height, formation of infrabony defects, osseous craters, ledges, etc.
Demineralized freeze-dried bone allograft by virtue of its osteoinductive[17,18] and osteoconductive[19] properties has provided sufficient evidence in the literature that it supports the formation of new attachment apparatus in the infrabony defects. The osteoinductive property has been attributed to the exposure of the BMPs and growth factors following the acid demineralization process of the allograft.[20,21,22] These BMPs and growth factors permit rapid revascularization and hard tissue in growth in the osseous defects thereby promoting periodontal regeneration. However, studies have shown that the amount of BMPs present in the graft particles may vary depending on the donor source.[23] This lead us to evaluate the relative efficacy of another bone graft material, that is, ABBX with respect to DFDBA.
However, ABBX has been proved to be osteoconductive only though a few studies have stated that it facilitates osteogenesis in the presence of osteogenic precursor cells.[10,12]
The selection of two- and three-walled infrabony defects was based on the results obtained from controlled clinical trials providing evidence that three-walled osseous defects allow better containment, stability, and increased blood supply to the graft.[24] Hence, two- and three-walled defects have a greater healing potential than one-walled defects after conventional and regenerative surgery.
In this study, it was observed that both the materials were well-tolerated by the patients as no unusual findings with regard to the postoperative healing as well as no sign or symptom of any other allergic manifestation was elicited. These findings concur with the findings of Schwartz et al.[25] and Hernandez et al.[26]
The soft tissue parameters viz. PD and attachment level were ascertained clinically, whereas, the hard tissue parameter such as depth of the infrabony defect was ascertained radiographically and the results thus obtained were subjected to statistical evaluation.
The defect-A showed a mean reduction of PD to be 2.13 ± 0.32 mm at 12 weeks postoperatively and 2.80 ± 0.39 mm at 24 weeks postoperatively, which were statistically significant at 1% probability level, implying thereby, that substantial pocket depth reduction had taken place as also shown by Lovelace et al.[27] and Katuri et al.[28]
The defect-B showed a mean reduction of PD to be 1.47 ± 0.26 mm at 12 weeks postoperatively and 2.27 ± 0.35 mm at 24 weeks postoperatively, which were also statistically significant at 1% probability level. These findings compare favorably with those found by Hutchens[29] and Yukna et al.[30]
This reduction in both the cases may be attributed to the resolution of the inflammatory component consequent to access flap surgery and the subsequent plaque control regime adopted by the patients.[31,32]
On comparing the mean pocket depth reduction obtained with the two materials (by ANOVA approach), we infer that the difference in their results was not significant. A similar pattern of pocket depth reduction with respect to time was experienced in both the defects. However, significant difference was presented by both the materials during each of the time-intervals (i.e. preoperative to 12 weeks postoperative, preoperative to 24 weeks postoperative, and 12 weeks postoperative to 24 weeks postoperative) indicating that the reduction was taking place throughout the span of the study.
The DFDBA group showed a mean gain in attachment level of 2.07 ± 0.32 mm at 12 weeks postoperatively and 2.80 ± 0.34 mm at 24 weeks postoperatively, which was found to be a substantial gain, statistically (P < 0.01), which is in accordance with those of Pearson et al.[33] and Oreamuno et al.[34]
The ABBX group showed a mean gain in attachment level of 1.40 ± 0.19 mm at 12 weeks postoperatively and 2.27 ± 0.28 mm at 24 weeks postoperatively, which was proved to be a substantial gain, statistically (P < 0.01). These findings are similar to those of Hutchens[29] and Yukna et al.[30]
On comparing the gain in mean attachment level obtained with the two materials (by ANOVA approach), we infer that a significant difference (P < 0.05) was present in the amount of gain obtained between the two defect sites. Better results are obtained with DFDBA as compared to ABBX. The gain in attachment level followed a similar pattern over both the defects and a substantial gain was noticed on the completion of the study span.
A mean linear bone fill of 1.45 ± 0.21 mm at 12 weeks postoperatively and 3.17 ± 0.55 mm at 24 weeks postoperatively was obtained with the DFDBA group. The result was found to be statistically significant at 1% probability level and was shown to be in conformity with those of Richardson et al.[35]
Concurrent to the findings of Yukna et al.[30] in our study a mean linear bone fill of 1.44 ± 0.23 mm at 12 weeks postoperatively and 3.76 ± 0.57 mm at 24 weeks postoperatively was obtained with the ABBX group and this was also significant at 1% probability level.
On comparing the mean linear bone fill obtained with the two materials (by ANOVA approach) we infer that the difference in their results was not significant. A similar pattern of linear bone fill with respect to time was obtained in both the defects. It was also observed that the rate of linear bone fill progressed in an almost uniform/similar rate over the entire study span.
The results of this study match those of a previous study by Richardson et al.,[35] which compared DFDBA and ABBX in the treatment of infrabony defects, in all respects except the gain in attachment level. In our study, the gain in attachment level was found to be more significant with the DFDBA (CD = 0.356) than with the ABBX at 5% probability level (CD = 0.346).
The difference in the mean measurements of this study and those cited above may be contributed by factors such as the differences in study designs, differences in patient populations, initial defect depth, criteria used in recording and analyzing the variable, operator's experience, and other variables.
It is important to emphasize that the data generated by this study derived from 24 weeks observations, a relatively short period of time when one considers the long term success of regenerative procedures. Hence, long-term studies are suggested to evaluate further the relative efficacy of the two grafting materials.
CONCLUSION
Within the constraints of this study, both the materials viz. ABBX and DFDBA have shown promising results for the treatment of periodontal infrabony defects thus warranting long-term studies with a larger sample size to explore their true regenerative potential to the maximum.
ACKNOWLEDGEMENT
We express special thanks to Dr. A.S. Sethi, Professor, Punjab School of Economics, Guru Nanak Dev University, Amritsar, for his help with the statistical analysis of the data and its interpretation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ripamonti U, Reddi AH. Periodontal regeneration: Potential role of bone morphogenetic proteins. J Periodontal Res. 1994;29:225–35. doi: 10.1111/j.1600-0765.1994.tb01216.x. [DOI] [PubMed] [Google Scholar]
- 2.Bowen JA, Mellonig JT, Gray JL, Towle HT. Comparison of decalcified freeze-dried bone allograft and porous particulate hydroxyapatite in human periodontal osseous defects. J Periodontol. 1989;60:647–54. doi: 10.1902/jop.1989.60.12.647. [DOI] [PubMed] [Google Scholar]
- 3.Spector M. Anorganic bovine bone and ceramic analogs of bone mineral as implants to facilitate bone regeneration. Clin Plast Surg. 1994;21:437–44. [PubMed] [Google Scholar]
- 4.Quintero G, Mellonig JT, Gambill VM, Pelleu GB., Jr A six-month clinical evaluation of decalcified freeze-dried bone allografts in periodontal osseous defects. J Periodontol. 1982;53:726–30. doi: 10.1902/jop.1982.53.12.726. [DOI] [PubMed] [Google Scholar]
- 5.Cortellini P, Pini Prato G, Tonetti MS. Periodontal regeneration of human infrabony defects. II. Re-entry procedures and bone measures. J Periodontol. 1993;64:261–8. doi: 10.1902/jop.1993.64.4.261. [DOI] [PubMed] [Google Scholar]
- 6.Batista EL, Jr, Novaes AB, Jr, Simonpietri JJ, Batista FC. Use of bovine-derived anorganic bone associated with guided tissue regeneration in intrabony defects. Six-monthevaluation at re-entry. J Periodontol. 1999;70:1000–7. doi: 10.1902/jop.1999.70.9.1000. [DOI] [PubMed] [Google Scholar]
- 7.Bowers GM, Chadroff B, Carnevale R, Mellonig J, Corio R, Emerson J, et al. Histologic evaluation of new attachment apparatus formation in humans. J Periodontol. 1989;60(Part III):683–93. doi: 10.1902/jop.1989.60.12.683. [DOI] [PubMed] [Google Scholar]
- 8.Masters LB, Mellonig JT, Brunsvold MA, Nummikoski PV. A clinical evaluation of demineralized freeze-dried bone allograft in combination with tetracycline in the treatment of periodontal osseous defects. J Periodontol. 1996;67:770–81. doi: 10.1902/jop.1996.67.8.770. [DOI] [PubMed] [Google Scholar]
- 9.Hall EE, Meffert RM, Hermann JS, Mellonig JT, Cochran DL. Comparison of bioactive glass to demineralized freeze-dried bone allograft in the treatment of intrabony defects around implants in the canine mandible. J Periodontol. 1999;70:526–35. doi: 10.1902/jop.1999.70.5.526. [DOI] [PubMed] [Google Scholar]
- 10.Urist MR, Hay PH, Dubuc F, Buring K. Osteogenetic competence. Clin Orthop Relat Res. 1969;64:194–220. [PubMed] [Google Scholar]
- 11.Karabuda C, Ozdemir O, Tosun T, Anil A, Olgaç V. Histological and clinical evaluation of 3 different grafting materials for sinus lifting procedure based on 8 cases. J Periodontol. 2001;72:1436–42. doi: 10.1902/jop.2001.72.10.1436. [DOI] [PubMed] [Google Scholar]
- 12.Callan DP, Rohrer MD. Use of bovine-derived hydroxyapatite in the treatment of edentulous ridge defects: A human clinical and histologic case report. J Periodontol. 1993;64:575–82. doi: 10.1902/jop.1993.64.6.575. [DOI] [PubMed] [Google Scholar]
- 13.Bright RW, Friedlaender GE, Sell KW. Tissue banking: The United States Navy Tissue Bank. Mil Med. 1977;142:503–10. [PubMed] [Google Scholar]
- 14.Salama R, Burwell RD, Dickson IR. Recombined grafts of bone and marrow. The beneficial effect upon osteogenesis of impregnating xenograft (heterograft) bone with autologous red marrow. J Bone Joint Surg Br. 1973;55:402–17. [PubMed] [Google Scholar]
- 15.Mellonig JT. Freeze-dried bone allografts in periodontal reconstructive surgery. Dent Clin North Am. 1991;35:505–20. [PubMed] [Google Scholar]
- 16.Sonis ST, Kaban LB, Glowacki J. Clinical trial of demineralized bone powder in the treatment of periodontal defects. J Oral Med. 1983;38:117–22. [PubMed] [Google Scholar]
- 17.Marinak KW, Mellonig JT, Towle HJ. The osteogenic potential of two human demineralized bone preparations using a xenogeneic model. J Periodontol. 1989;60:12–8. doi: 10.1902/jop.1989.60.1.12. [DOI] [PubMed] [Google Scholar]
- 18.Mellonig JT. Decalcified freeze-dried bone allograft as an implant material in human periodontal defects. Int J Periodontics Restorative Dent. 1984;4:41–56. [PubMed] [Google Scholar]
- 19.Mellonig JT, Bowers GM, Bailey RC. Comparison of bone graft materials. Part I. New bone formation with autografts and allografts determined by Strontium-85. J Periodontol. 1981;52:291–6. doi: 10.1902/jop.1981.52.6.291. [DOI] [PubMed] [Google Scholar]
- 20.Urist MR, Dowell TA, Hay PH, Strates BS. Inductive substrates for bone formation. Clin Orthop Relat Res. 1968;59:59–96. [PubMed] [Google Scholar]
- 21.Urist MR, Iwata H. Preservation and biodegradation of the morphogenetic property of bone matrix. J Theor Biol. 1973;38:155–67. doi: 10.1016/0022-5193(73)90231-2. [DOI] [PubMed] [Google Scholar]
- 22.Mellonig JT. Decalcified freeze-dried bone allograft as an implant material in human periodontal defects. Int J Periodontics Restorative Dent. 1984;4:40–55. [PubMed] [Google Scholar]
- 23.Boyan BD, Ranly DM, Schwartz Z. Use of growth factors to modify osteoinductivity of demineralized bone allografts: Lessons for tissue engineering of bone. Dent Clin North Am. 2006;50:217–28. doi: 10.1016/j.cden.2005.11.007. viii. [DOI] [PubMed] [Google Scholar]
- 24.Camargo PM, Lekovic V, Weinlaender M, Nedic M, Vasilic N, Wolinsky LE, et al. A controlled re-entry study on the effectiveness of bovine porous bone mineral used in combination with a collagen membrane of porcine origin in the treatment of intrabony defects in humans. J Clin Periodontol. 2000;27:889–96. doi: 10.1034/j.1600-051x.2000.027012889.x. [DOI] [PubMed] [Google Scholar]
- 25.Schwartz Z, Mellonig JT, Carnes DL, Jr, de la Fontaine J, Cochran DL, Dean DD, et al. Ability of commercial demineralized freeze-dried bone allograft to induce new bone formation. J Periodontol. 1996;67:918–26. doi: 10.1902/jop.1996.67.9.918. [DOI] [PubMed] [Google Scholar]
- 26.Hernandez M, Pette GA, Grenier A, Villanueva C, Lask E, Parker W. A clinical and histological comparison of two different bone augmentation materials in the atrophic pre-maxilla. Compend Contin Educ Dent. 2012;33:e26–32. [PubMed] [Google Scholar]
- 27.Lovelace TB, Mellonig JT, Meffert RM, Jones AA, Nummikoski PV, Cochran DL. Clinical evaluation of bioactive glass in the treatment of periodontal osseous defects in humans. J Periodontol. 1998;69:1027–35. doi: 10.1902/jop.1998.69.9.1027. [DOI] [PubMed] [Google Scholar]
- 28.Katuri KK, Kumar PJ, Swarna C, Swamy DN, Arun KV. Evaluation of bioactive glass and demineralized freeze dried bone allograft in the treatment of periodontal intraosseous defects: A comparative clinico-radiographic study. J Indian Soc Periodontol. 2013;17:367–72. doi: 10.4103/0972-124X.115660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hutchens LH., Jr The use of a bovine bone mineral in periodontal osseous defects: Case reports. Compend Contin Educ Dent. 1999;20:365. [PubMed] [Google Scholar]
- 30.Yukna RA, Krauser JT, Callan DP, Evans GH, Cruz R, Martin M. Multi-center clinical comparison of combination anorganic bovine-derived hydroxyapatite matrix (ABM)/cell binding peptide (P-15) and ABM in human periodontal osseous defects 6-month results. J Periodontol. 2000;71:1671–9. doi: 10.1902/jop.2000.71.11.1671. [DOI] [PubMed] [Google Scholar]
- 31.Athanasiou KA, Niederauer GG, Agrawal CM. Sterilization, toxicity, biocompatibility and clinical applications of polylactic acid/polyglycolic acid copolymers. Biomaterials. 1996;17:93–102. doi: 10.1016/0142-9612(96)85754-1. [DOI] [PubMed] [Google Scholar]
- 32.Friedman N. Mucogingival surgery. Texas Dent J 1957. In: Lindhe J, Karring T, Lary NP, editors. Clinical Periodontology and Implant Dentistry. 4th ed. Vol. 75. New Delhi: Blackwell Munksgaard, Jaypee Brothers; 2003. pp. 358–62. [Google Scholar]
- 33.Pearson GE, Rosen S, Deporter DA. Preliminary observations on the usefulness of a decalcified, freeze-dried cancellous bone allograft material in periodontal surgery. J Periodontol. 1981;52:55–9. doi: 10.1902/jop.1981.52.2.55. [DOI] [PubMed] [Google Scholar]
- 34.Oreamuno S, Lekovic V, Kenney EB, Carranza FA, Jr, Takei HH, Prokic B. Comparative clinical study of porous hydroxyapatite and decalcified freeze-dried bone in human periodontal defects. J Periodontol. 1990;61:399–404. doi: 10.1902/jop.1990.61.7.399. [DOI] [PubMed] [Google Scholar]
- 35.Richardson CR, Mellonig JT, Brunsvold MA, McDonnell HT, Cochran DL. Clinical evaluation of Bio-Oss: A bovine-derived xenograft for the treatment of periodontal osseous defects in humans. J Clin Periodontol. 1999;26:421–8. doi: 10.1034/j.1600-051x.1999.260702.x. [DOI] [PubMed] [Google Scholar]