

Abstract
Background:
The purpose of this study was to determine the effect of three chewing gums and paraffin on the remineralization and the hardness of demineralized enamel.
Materials and Methods:
A total of 12 subjects wore intraoral palatal appliances with two demineralized bovine enamel slabs. The study consisted of four experimental periods each lasting 21-days, during which subjects were assigned to one of three gum-chewing regimens: gum containing sorbitol, xylitol and a mixture of sorbitol and xylitol and with paraffin as control. The appliances were worn during gum-chewing for 20 min and then retained for 20 min 4 times/day. The slabs were subjected to energy dispersive X-ray spectroscopy analysis and surface microhardness measurements before in setting into the appliance and after the experimental period. The data were subjected to analysis of variance for repeated measures. A P < 0.05 was considered statistically significant.
Results:
Mineral analysis revealed no significant difference between the baseline and after chewing periods for all groups (P > 0.05). No significant difference was found among the groups either for the baseline measurements or after chewing periods (P > 0.05). All groups showed higher microhardness values after the chewing periods than the baseline except for the Vivident Xylit group (P < 0.05).
Conclusion:
The chewing of gum had no effect on the Ca/P ratio of demineralized enamel surfaces. The hardening of the demineralized enamel surfaces may vary according to the type of chewing gum.
Keywords: Chewing gum, enamel, energy dispersive X-ray spectroscopy, microhardness
INTRODUCTION
Dental caries is a major health problem.[1] Sugar-free chewing gums have been suggested to decrease the caries incidence as they have an anti-cariogenic effect.[2,3,4,5] This effect is based on the action of two factors: Saliva stimulation through the chewing process and integration of dietary polyols.[3]
In recent years, the use of chewing gum after meals has gained popularity as it prevents the formation of dental caries by stimulating salivary flow. The increase in flow enhances the buffering capacity of saliva, which effectively neutralizes the drop in plaque pH that occurs after eating.[6] Increased levels of calcium and phosphate in gum-stimulated saliva also limit demineralization and enhance remineralization.[7,8]
The most common dietary polyols used in sugar-free chewing gums are xylitol and sorbitol.[3,9] Most oral bacteria do not metabolize xylitol and sorbitol to form acid. Xylitol is a sugar alcohol derived from pentose sugar xylose and sorbitol is a sugar alcohol derived from glucose. Both stimulate a gustatory reflex that together with the chewing process, enhances saliva stimulation.[3] Thus, sugar substitution and salivary stimulation could be equally responsible for the non-cariogenicity of sugar-free chewing gum.[8] Sorbitol is metabolized not at all by most microorganisms, it can be fermented at a slow rate by all of the mutans streptococci including Streptococcus mutans while xylitol is considered to be non-acidogenic.[9] Xylitol is a caloric sugar substitute that is not readily fermented by oral microorganisms[1] and also actively protective against tooth decay through reduction in S. mutans and levels of lactic acid produced by these bacteria.[10]
There are various reports that evaluated the effect of polyol gums on the remineralization of denimeralized enamel.[11,12,13,14] There are contradictory findings regarding the effects of polyols’ types in chewing gums on caries lesions. In an in situ study, comparing the remineralizing effect of gums containing sorbitol and a mixture of sorbitol/xylitol on caries-like enamel lesions, no differences were observed between the gums.[15] On the other hand, the use of xylitol sweetened gum has been found to be more effective on rehardening of dentinal lesions than sorbitol sweetened gums.[16] A recent systematic review of clinical trials investigating the effects of xylitol challenged the greater caries reduction claimed for gums containing xylitol compared with other sugar alcohol.[17]
In the literature, it is a matter of controversy whether the main effect of polyols in gums is attributed to the sugar substitute per se or saliva stimulation.[4,9,18]
In a systematic review it has been reported that the caries-reducing effect was not due to the therapeutic action of polyol, but rather to the chewing process itself and subsequent saliva stimulation.[19]
Therefore, this in situ study was aimed to compare the effect of three chewing gums: Gum containing sorbitol (Trident Splash), xylitol (First Ice) and a mixture of sorbitol and xylitol (Vivident Xylit) and paraffin on the remineralization and the hardness of demineralized enamel.
MATERIALS AND METHODS
Subject recruitment
A total of 12 (11 female, 1 male) healthy adult subjects (mean age 28.5) were recruited from the staff of the Hacettepe University Faculty of Dentistry for this randomized, double-blind, cross-over study. The protocol of this study was approved by the University of Hacettepe Human Research Ethics Committee. Written informed consent was obtained from all participants prior to the treatment. Inclusion criteria were as follows: Having no current caries activity, having a minimum of 20 teeth in the mouth, having average oral hygiene (tooth brushing at least twice-a-day) and being willing not to use any remineralizing product during the study period except for the dentifrice used in the study. The following items were considered exclusion criteria: Periodontal disease; presence of any allergy to oral hygiene products or oral therapeutic agents; and use of any of the following remineralizing or fluoridated products in the 30 days prior to insertion of the appliances: Gels, pills, varnishes, fillings and use of any chewing gum, fluoridated toothpaste (except for the standard toothpaste that was used during the study and the washout phase) or mouthrinse in the days prior to insertion of the appliances.
All volunteers were clinically and radiographically determined. Volunteers who did not satisfy the inclusion criteria were excluded. For the rest of the volunteers, the stimulated salivary flow rate and buffer capacity were measured by a commercially available test kit (caries risk test [CRT] buffer, Ivoclar Vivadent, Schaan, Liechtenstein), pH of saliva was measured using a pH stick (IsoLab Laborgerate, Wertheim, Germany) and levels of Mutans Streptococcus and Lactobacillus were measured using a saliva check test (CRT bacteria, Ivoclar Vivadent, Schaan, Liechtenstein). According to the results of these examinations, 12 volunteers who had low caries risk were enrolled in the study.
Preparation and demineralization of enamel specimens
Two square-shaped enamel slabs were cut from each bovine incisor and sterilized by storage in 2% formaldehyde solution[20,21] [Figure 1a and b].
Figure 1.
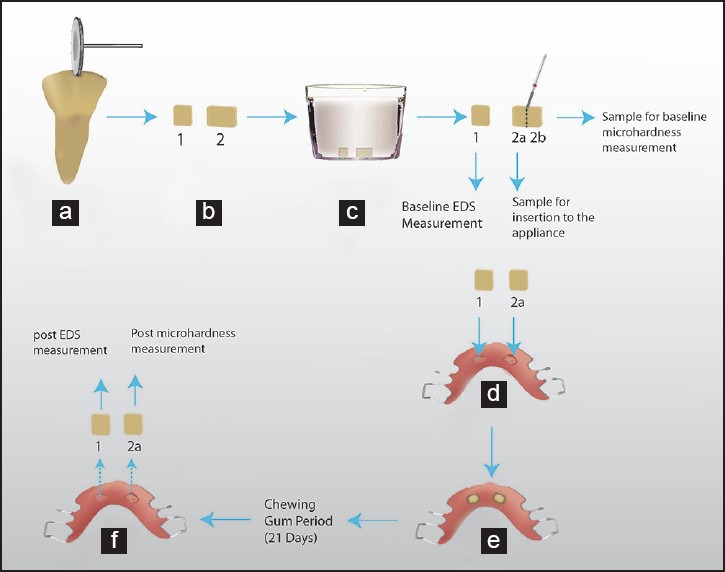
Schematic representation of sequence of the experimental protocol: (a) Sectioning of bovine tooth, (b) prepared enamel samples, (c) keeping of samples in demineralization solution, (d) appliance used in the study, (e) inserted samples in the appliance, (f) removal of samples from the appliance
After the samples were glued to a mold using nail varnish, the enamel surfaces were ground flat and polished, thereby removing the outer surface of enamel.[11] Then, the slabs were flattened from the dentin side to a thickness of 2 mm (Mecapol P230, Presi, Grenoble, France).
Demineralization of slabs was achieved using methylcellulose gel according to ten Cate et al.[22] [Figure 1c]. Demineralizing solution was prepared freshly before each study period to create initial caries lesions. The prepared enamel slabs (n:24 for each period, totally n:96) were placed in a glass holder and fixed to the holder using nail varnish from the bottom of the slabs. The solution was added to the holder and the demineralization process was applied for 10 days at 37°C. The pH value of the solution was adjusted to 4.6. After demineralization, the solution was removed from the holder and the slabs were washed under running water. One slab of each pair was used for surface hardness measurements and the other one for energy dispersive X-ray spectroscopy (EDS) analysis [Figure 1b].
Intra-oral palatal appliance
A removable intraoral appliance was fabricated in acrylic resin for each volunteer's upper jaw.[23] Two holes (5 mm × 5 mm × 2.5 mm) were made in the right and the left sides of the mid-palatal part. The enamel slabs were placed in these holes using dental wax [Figure 1d and e].
Study protocols
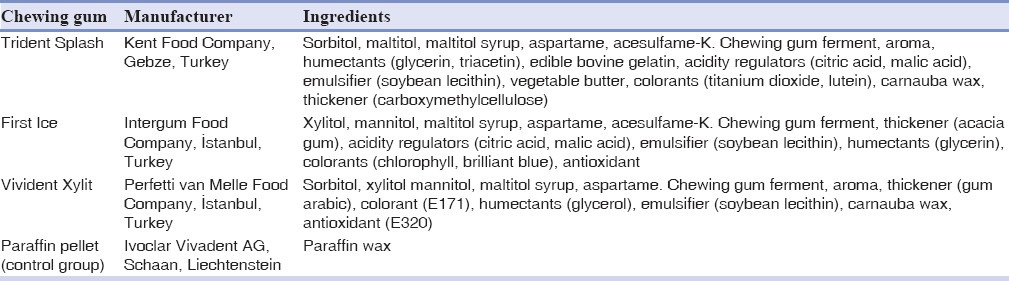
Three different types of chewing gum were used for the study, with paraffin pellets used for the control group. The chewing gums tested in the present study contained sorbitol (Trident Splash), xylitol (First Ice) and a mixture of sorbitol and xylitol (Vivident Xylit). The ingredients of the chewing gums are shown in Table 1.
Table 1.
Chewing gums used in the study
All subjects participated in four experimental periods in randomized order, each lasting 21 days. For each period, all subjects crossed over to each assigned treatment with 1 week between treatments as a washout period. The participants did not know which gum they were chewing during that study period. Chewing gums were given to them in a plastic box. All subjects chewed the gums and paraffin at their natural chewing frequency for 20 min 4 times a day. The appliances were worn for 20 min of gum chewing and for 20 min following removal of the chewing gum from the mouth. They chewed the gum at the following times: 10:00 a.m., 2:00 p.m., 6:00 p.m. and 9:00 p.m. At all other times, the appliances were kept in a moist paper tissue and stored in a box at room temperature. The subjects were instructed not to eat, drink, or smoke while wearing the appliance and they cleaned the appliance with a soft toothbrush (Oral-B expert complete 7, P & G, GmbH, Schwalbach, Germany) without using any dentifrice. They were instructed to avoid brushing directly on the enamel slabs. They were also instructed to brush their teeth twice per day with a standardized fluoride-containing dentifrice (Ipana 7 full prevention, P & G GmbH, Schwalbach, Germany). The subjects were asked to continue their normal dietary intake. They were told not to use any remineralizing agents. At the end of each experimental period, the appliances were collected and the enamel slabs were removed. During a 1-week washout phase, the appliances were kept at room temperature in a humidifier. The subjects were instructed not to chew gum during the washout period. On the 7th day, the appliances were refilled with a new set of enamel slabs.
EDS analysis
Ca (Calcium) and P (Phosphorus) concentrations were analyzed by EDS, using a Bruker-Axs XFlash 3001 silicon drift detector EDS device (Carl Zeiss SMT Ltd, Cambridge, UK) integrated into a scanning electron microscope (Carl Zeiss EVO-50). The EDS spectrometer is an instrument that quantitatively determines the elements within a sample by irradiating the sample with X-rays and then analyzing the re-emitted fluorescent X-rays.[24] The acquisition time of the EDS spectrum was 45 s at an accelerating voltage of 25 kV and with a beam current of 8 nA and focus distance of 10 mm.
Demineralized enamel slabs were analyzed before being inset into the intraoral appliance and after the experimental period by an examiner who did not know, which chewing gum group was analyzing. The slabs were analyzed at five different points and the averages of the results were calculated.
Surface microhardness measurement
The demineralized enamel slabs were divided in half. One of the halves was retained for baseline measurements and stored in a humidified environment. The other half of enamel slab of the pair was inset into an intraoral appliance. At the end of the experimental period, the enamel slab was removed from the appliance [Figure 1f]. For surface enamel hardness measurement, both enamel slabs was embedded in a composite mold with the upper surface of the slabs at the top. Three indentations were made in different regions of the sample using a Vickers indenter with a 50 g load for 10 s (HMV-2; Shimadzu Corporation, Tokyo, Japan).
Statistical analysis
The data were subjected to analysis of variance for repeated measures and processed with statistical package for the social sciences (SPSS) (version 15; SPSS Inc., Chicago, IL, USA). A P < 0.05 was considered statistically significant. One-way ANOVA was used to test the differences between the groups for the baseline and experimental periods’ data.
RESULTS
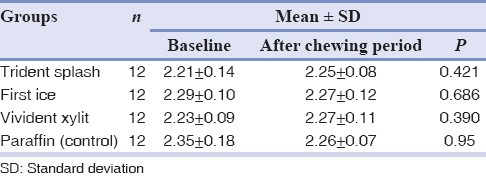
The EDS results regarding Ca/P ratio are shown in Table 2. Mineral analysis revealed no significant difference between baseline and after chewing periods for all groups (P > 0.05). No significant difference was found among the four groups either for the baseline measurements or after chewing periods (P > 0.05).
Table 2.
Ca/P ratio
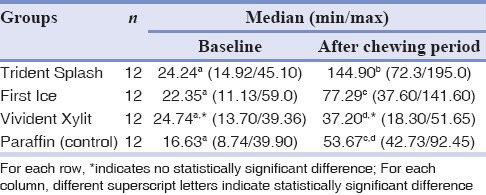
Microhardness data (min, max, median) are shown in Table 3. All groups showed significantly higher microhardness values after the chewing periods than the baseline microhardness values (P < 0.05) except for the Vivident Xylit group (P = 0.074). No significant differences were found between the groups regarding the baseline measurements (P > 0.05). When the microhardness values after the chewing periods were compared, the Trident Splash group was seen to have higher values than the other groups (P < 0.05). While the Vivident Xylit group showed significantly lower hardness values than the other chewing gum groups, the paraffin group showed hardness values similar to those of all groups except for the Trident Splash group.
Table 3.
Vickers hardness number
DISCUSSION
In the present study, an in situ model was applied to verify the effect of different types of chewing gum and paraffin on hardness and mineral content of demineralized enamel using EDS and microhardness test. In situ studies are important because they gather more clinical variables that mimic clinical situations. However, the main disadvantage of these kinds of studies is the dependency solely on the volunteer's compliance, which can be challenging.[25] As salivary flow, buffer capacity and mutans streptococci level could affect the results, these examinations need to be evaluated before the study is carried out.[25] Enrollment of low-risk subjects may increase the controllability of the experiment.[26,27,28]
Bovine enamel is widely used instead of human enamel in the production of initial carious lesions, under the same conditions and with the same demineralization system. As the human enamel is harder and less porous than bovine enamel and less rapidly demineralized, the use of bovine enamel is an advantage for reducing the length of demineralization.[29] That was why bovine teeth were used in the present study.
Indentation hardness testing with either a Knoop or Vickers indenter has been used for the measurement of initial enamel hardness, enamel softening and enamel hardening after remineralization.[30] In the present study, the surface hardness values of the demineralized enamel surface and the enamel surface after chewing the gums and paraffin were examined with a Vickers indenter. In the literature, there are conflicting results regarding the effectiveness of chewing gums on reduction of demineralization. It is not fully understood whether polyols’ effect or mastication causes remineralization. Machiulskiene et al.[4] found that the caries preventive effect of chewing sugar-free gum was related to the chewing process itself rather than the additives, such as polyols and carbamide. In another study, no difference was reported between the remineralization effect of sucrose-containing and sorbitol-containing chewing gums.[12] Supporting these results, both sorbitol-containing chewing gum and paraffin resulted in significantly higher plaque pH values.[31] On the other hand, it has been reported that gums with higher dose of xylitol showed higher caries reduction than gums with both xylitol and sorbitol, only sorbitol, only sucrose and no gum. The sucrose gum group showed the worst results.[32] In the present study, enamel surfaces had harder surfaces after gums and paraffin was chewed than the baseline measurements. Based on our results, it might be speculated that mastication affects the hardness rather than the polyols in the chewing gums as hardness increased in the paraffin group.
Today, in most chewing gums polyols such as sorbitol and xylitol are used as sugar substitutes. In the present study gums with sorbitol, xylitol and both were used. When comparing chewing gums with different polyols and paraffin, the sorbitol-gum, Trident Splash, showed higher microhardness values than the other chewing gums and paraffin. It can be speculated that the flavor of Trident Splash and the syrup in this chewing gum stimulated the saliva more effectively than the others. Moreover, the harder texture of this gum might have accounted for the increased saliva stimulation, which resulted in harder surfaces. It has been reported that the intensity of the masticatory stimulus falls due to softening of the gum.[33] However, our findings are not in agreement with a study by Manning et al.,[15] who reported that the differences in the properties of sorbitol and xylitol in the chewing gums did not affect their ability to enhance remineralization due to salivary stimulation. Another study by Wennerholm et al.[34] showed that the mineral loss of enamel were the same and independent of whether the participants had chewed a gum containing xylitol, sorbitol or a mixture of the two. A comparison of other clinical studies also found similar remineralization effects for gums containing xylitol, sorbitol, or a mixture of the two.[12,15,35]
In the present study, the Vickers hardness number (VHN) of demineralized enamel was between 15 and 25 VHN. After the chewing periods, this value increased to 53-145 VHN. It was observed that all chewing gums and paraffin used in this study increased the surface hardness values of the demineralized enamel, but these increased values were lower than the hardness values of sound enamel reported in the literature.[36]
Calcium and phosphate ions are building blocks for the remineralization process.[30] For this reason, we examined Ca and P percentages of the demineralized enamel surface before and after using chewing gums. In EDS measurements, we were unable to detect any significant changes in the Ca/P ratio of demineralized enamel. It might have been expected that Ca/P ratio would be higher than baseline values as the hardness values were increased. In a study conducted by Mäkinen et al.,[37] the Ca/P ratio of dentin was determined after using chewing gums for 2 years. Contrary to our findings, samples showed higher Ca/P ratios than baseline measurements. That study was a long-term one and those researchers examined dentin samples instead of enamel. Our study was a short-lasting in situ experiment and that might have been the reason why we found no difference in Ca/P ratios. Wennerholm et al.[34] found no significant difference between four chewing gum groups (70% xylitol, 35% xylitol + 35% sorbitol, 17.5% xylitol + 52.5% sorbitol, 70% sorbitol) in their study and they also attributed this result to the fact that the study had a short-lasting protocol (25 days). Therefore, long-term clinical studies are required to confirm our results.
CONCLUSION
Based on the limitations of the present study, it might be concluded that the use of sugar-free chewing gum had no effect on the Ca/P ratio of demineralized enamel surfaces. The hardening of the demineralized enamel surfaces may vary according to the type of chewing gum.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Hildebrandt GH, Sparks BS. Maintaining mutans streptococci suppression with xylitol chewing gum. J Am Dent Assoc. 2000;131:909–16. doi: 10.14219/jada.archive.2000.0309. [DOI] [PubMed] [Google Scholar]
- 2.Beiswanger BB, Boneta AE, Mau MS, Katz BP, Proskin HM, Stookey GK. The effect of chewing sugar-free gum after meals on clinical caries incidence. J Am Dent Assoc. 1998;129:1623–6. doi: 10.14219/jada.archive.1998.0113. [DOI] [PubMed] [Google Scholar]
- 3.Edgar WM. Sugar substitutes, chewing gum and dental caries - A review. Br Dent J. 1998;184:29–32. doi: 10.1038/sj.bdj.4809535. [DOI] [PubMed] [Google Scholar]
- 4.Machiulskiene V, Nyvad B, Baelum V. Caries preventive effect of sugar-substituted chewing gum. Community Dent Oral Epidemiol. 2001;29:278–88. doi: 10.1034/j.1600-0528.2001.290407.x. [DOI] [PubMed] [Google Scholar]
- 5.Kandelman D, Gagnon G. A 24-month clinical study of the incidence and progression of dental caries in relation to consumption of chewing gum containing xylitol in school preventive programs. J Dent Res. 1990;69:1771–5. doi: 10.1177/00220345900690111201. [DOI] [PubMed] [Google Scholar]
- 6.Edgar WM. Saliva and dental health. Clinical implications of saliva: Report of a consensus meeting. Br Dent J. 1990;169:96–8. doi: 10.1038/sj.bdj.4807284. [DOI] [PubMed] [Google Scholar]
- 7.Dawes C, Kubieniec K. The effects of prolonged gum chewing on salivary flow rate and composition. Arch Oral Biol. 2004;49:665–9. doi: 10.1016/j.archoralbio.2004.02.007. [DOI] [PubMed] [Google Scholar]
- 8.Edgar WM, Geddes DA. Chewing gum and dental health - A review. Br Dent J. 1990;168:173–7. doi: 10.1038/sj.bdj.4807129. [DOI] [PubMed] [Google Scholar]
- 9.Hayes C. The effect of non-cariogenic sweeteners on the prevention of dental caries: A review of the evidence. J Dent Educ. 2001;65:1106–9. [PubMed] [Google Scholar]
- 10.Ly KA, Milgrom P, Rothen M. Xylitol, sweeteners, and dental caries. Pediatr Dent. 2006;28:154–63. [PubMed] [Google Scholar]
- 11.Schirrmeister JF, Seger RK, Altenburger MJ, Lussi A, Hellwig E. Effects of various forms of calcium added to chewing gum on initial enamel carious lesions in situ. Caries Res. 2007;41:108–14. doi: 10.1159/000098043. [DOI] [PubMed] [Google Scholar]
- 12.Creanor SL, Strang R, Gilmour WH, Foye RH, Brown J, Geddes DA, et al. The effect of chewing gum use on in situ enamel lesion remineralization. J Dent Res. 1992;71:1895–900. doi: 10.1177/00220345920710120801. [DOI] [PubMed] [Google Scholar]
- 13.Shen P, Cai F, Nowicki A, Vincent J, Reynolds EC. Remineralization of enamel subsurface lesions by sugar-free chewing gum containing casein phosphopeptide-amorphous calcium phosphate. J Dent Res. 2001;80:2066–70. doi: 10.1177/00220345010800120801. [DOI] [PubMed] [Google Scholar]
- 14.Manton DJ, Walker GD, Cai F, Cochrane NJ, Shen P, Reynolds EC. Remineralization of enamel subsurface lesions in situ by the use of three commercially available sugar-free gums. Int J Paediatr Dent. 2008;18:284–90. doi: 10.1111/j.1365-263X.2008.00920.x. [DOI] [PubMed] [Google Scholar]
- 15.Manning RH, Edgar WM, Agalamanyi EA. Effects of chewing gums sweetened with sorbitol or a sorbitol/xylitol mixture on the remineralisation of human enamel lesions in situ. Caries Res. 1992;26:104–9. doi: 10.1159/000261493. [DOI] [PubMed] [Google Scholar]
- 16.Mäkinen KK, Mäkinen PL, Pape HR, Jr, Allen P, Bennett CA, Isokangas PJ, et al. Stabilisation of rampant caries: Polyol gums and arrest of dentine caries in two long-term cohort studies in young subjects. Int Dent J. 1995;45:93–107. [PubMed] [Google Scholar]
- 17.Lingström P, Holm AK, Mejàre I, Twetman S, Söder B, Norlund A, et al. Dietary factors in the prevention of dental caries: A systematic review. Acta Odontol Scand. 2003;61:331–40. doi: 10.1080/00016350310007798. [DOI] [PubMed] [Google Scholar]
- 18.Alanen P, Isokangas P, Gutmann K. Xylitol candies in caries prevention: Results of a field study in Estonian children. Community Dent Oral Epidemiol. 2000;28:218–24. doi: 10.1034/j.1600-0528.2000.280308.x. [DOI] [PubMed] [Google Scholar]
- 19.Mickenautsch S, Leal SC, Yengopal V, Bezerra AC, Cruvinel V. Sugar-free chewing gum and dental caries: A systematic review. J Appl Oral Sci. 2007;15:83–8. doi: 10.1590/S1678-77572007000200002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cury JA, Francisco SB, Simões GS, Del Bel Cury AA, Tabchoury CP. Effect of a calcium carbonate-based dentifrice on enamel demineralization in situ. Caries Res. 2003;37:194–9. doi: 10.1159/000070444. [DOI] [PubMed] [Google Scholar]
- 21.Rios D, Honório HM, Magalhães AC, Delbem AC, Machado MA, Silva SM, et al. Effect of salivary stimulation on erosion of human and bovine enamel subjected or not to subsequent abrasion: An in situ/ex vivo study. Caries Res. 2006;40:218–23. doi: 10.1159/000092229. [DOI] [PubMed] [Google Scholar]
- 22.ten Cate JM, Dundon KA, Vernon PG, Damato FA, Huntington E, Exterkate RA, et al. Preparation and measurement of artificial enamel lesions, a four-laboratory ring test. Caries Res. 1996;30:400–7. doi: 10.1159/000262351. [DOI] [PubMed] [Google Scholar]
- 23.Suda R, Suzuki T, Takiguchi R, Egawa K, Sano T, Hasegawa K. The effect of adding calcium lactate to xylitol chewing gum on remineralization of enamel lesions. Caries Res. 2006;40:43–6. doi: 10.1159/000088905. [DOI] [PubMed] [Google Scholar]
- 24.Asaka Y, Miyazaki M, Aboshi H, Yoshida T, Takamizawa T, Kurokawa H, et al. EDX fluorescence analysis and SEM observations of resin composites. J Oral Sci. 2004;46:143–8. doi: 10.2334/josnusd.46.143. [DOI] [PubMed] [Google Scholar]
- 25.Higham SM, Pretty IA, Edgar WM, Smith PW. The use of in situ models and QLF for the study of coronal caries. J Dent. 2005;33:235–41. doi: 10.1016/j.jdent.2004.10.016. [DOI] [PubMed] [Google Scholar]
- 26.Hara AT, Queiroz CS, Paes Leme AF, Serra MC, Cury JA. Caries progression and inhibition in human and bovine root dentine in situ. Caries Res. 2003;37:339–44. doi: 10.1159/000072165. [DOI] [PubMed] [Google Scholar]
- 27.Aires CP, Tabchoury CP, Del Bel Cury AA, Koo H, Cury JA. Effect of sucrose concentration on dental biofilm formed in situ and on enamel demineralization. Caries Res. 2006;40:28–32. doi: 10.1159/000088902. [DOI] [PubMed] [Google Scholar]
- 28.Magalhães AC, Rios D, Delbem AC, Buzalaf MA, Machado MA. Influence of fluoride dentifrice on brushing abrasion of eroded human enamel: An in situ/ex vivo study. Caries Res. 2007;41:77–9. doi: 10.1159/000096110. [DOI] [PubMed] [Google Scholar]
- 29.Amaechi BT, Higham SM, Edgar WM. Factors affecting the development of carious lesions in bovine teeth in vitro. Arch Oral Biol. 1998;43:619–28. doi: 10.1016/s0003-9969(98)00043-0. [DOI] [PubMed] [Google Scholar]
- 30.Tantbirojn D, Huang A, Ericson MD, Poolthong S. Change in surface hardness of enamel by a cola drink and a CPP-ACP paste. J Dent. 2008;36:74–9. doi: 10.1016/j.jdent.2007.10.008. [DOI] [PubMed] [Google Scholar]
- 31.Jensen ME. Effects of chewing sorbitol gum and paraffin on human interproximal plaque pH. Caries Res. 1986;20:503–9. doi: 10.1159/000260981. [DOI] [PubMed] [Google Scholar]
- 32.Isokangas P, Alanen P, Tiekso J, Makinen KK. Xylitol chewing gum in caries prevention: A field study in children. J Am Dent Assoc. 1988;117:315–20. doi: 10.1016/s0002-8177(88)72017-6. [DOI] [PubMed] [Google Scholar]
- 33.Rosenhek M, Macpherson LM, Dawes C. The effects of chewing-gum stick size and duration of chewing on salivary flow rate and sucrose and bicarbonate concentrations. Arch Oral Biol. 1993;38:885–91. doi: 10.1016/0003-9969(93)90098-7. [DOI] [PubMed] [Google Scholar]
- 34.Wennerholm K, Arends J, Birkhed D, Ruben J, Emilson CG, Dijkman AG. Effect of xylitol and sorbitol in chewing-gums on mutans streptococci, plaque pH and mineral loss of enamel. Caries Res. 1994;28:48–54. doi: 10.1159/000261620. [DOI] [PubMed] [Google Scholar]
- 35.Leach SA, Lee GT, Edgar WM. Remineralization of artificial caries-like lesions in human enamel in situ by chewing sorbitol gum. J Dent Res. 1989;68:1064–8. doi: 10.1177/00220345890680060201. [DOI] [PubMed] [Google Scholar]
- 36.Pinto CF, Paes Leme AF, Cavalli V, Giannini M. Effect of 10% carbamide peroxide bleaching on sound and artificial enamel carious lesions. Braz Dent J. 2009;20:48–53. doi: 10.1590/s0103-64402009000100008. [DOI] [PubMed] [Google Scholar]
- 37.Mäkinen KK, Chiego DJ, Jr, Allen P, Bennett C, Isotupa KP, Tiekso J, et al. Physical, chemical, and histologic changes in dentin caries lesions of primary teeth induced by regular use of polyol chewing gums. Acta Odontol Scand. 1998;56:148–56. doi: 10.1080/000163598422884. [DOI] [PubMed] [Google Scholar]