

Abstract
Background:
Hyperlipidemia is a well-documented risk factor for coronary heart disease and a great wealth of clinical trials have shown that early detection of hyperlipidemia and prescribing drugs that lower elevated lipid levels reduce serious cardiovascular events, such as myocardial infarction, heart failure and stroke. Fordyce granules (FGs) are sebaceous glands without hair follicles, most often located under the epithelium of the cheek and the vermilion border of lip. The incidence of FGs is typically high and their presence is usually regarded as a normal variation of the oral mucosa. The aim of this study was to investigate the pattern of anatomical distribution and density of FGs and also to explore any potential relationship between the detection of FGs and the state of hyperlipidemia.
Materials and Methods:
A cross-sectional, prospective study was designed. The participants were divided into two groups; first group consisted of individuals with FGs and the second group included those with no FGs detected. All participants were fasting 9-12 h before they were subjected to a comprehensive oral examination and their blood was sampled and tested for complete lipid profile. The presence of FGs was scored based on the number of the granules and their anatomical distribution. Chi-square test was used and P < 0.05 was considered as significant.
Results:
A total of 350 patients were recruited for this study, nearly 90% (n = 314) elicit detectable FGs. The FGs were mainly located on the buccal mucosa with or without labial involvement and their density tend to reduce with age and also with smoking. Individuals with elevated lipid profile tend to have the highest score of the FGs.
Conclusion:
According to this report, the presence of high numbers of FGs in people with high risk factors for cardiovascular disease should not be neglected.
Keywords: Blood lipid profile, cardiovascular disease, ectopic, Fordyce's granules, Fordyce's spots, hyperlipidemia, sebaceous glands, smoking
INTRODUCTION
Sebaceous glands are normal adnexal structures of the skin, but may also be found within the mouth, where they are referred to as Fordyce's granules (FGs) or heterotopic/ectopic sebaceous glands.[1] The granules were initially described by Kölliker in 1861, but are named after Fordyce who reported on the same problem in 1896.[2] Although Fordyce felt that the presence of the phenomena was a sign of a disease, most of the clinicians today consider them as a normal variation made up by collections of sebaceous glands covered with intact mucosa.[3,4,5]
According to the English literature, there are many studies reporting the incidence of FGs in the general population. However, there are no serious attempt to investigate the significance of this phenomenon and any relationship between the appearance of FGs and general health.
The Chemical composition of Fordyce's spots was found to be identical to that of sebaceous glands on the skin and about 50% of sebum composition is triglycerides.[6,7] As far as there is a possibility of fat deposition in an ectopic place with hyperlipidemic patients (such as xantholesma) and due to the importance of early detection and prevention of hyperlipidemia, there was a demand to investigate the presence of these ectopic fatty granules in relation to hyperlipidemia in view of comparability of their chemical composition to other lipid-containing glands or lesions.
The aim of this study was to investigate the pattern of distribution of FGs in adults in relation to anatomical location and density of granules using a practical scoring system. The study also relates the distribution of the granules to the age of participants and their smoking status. Finally and more importantly we explored any potential relationship between the detection of FGs with hyperlipidemia to find out if the presence of FGs with specific density and distribution pattern may serve as a marker for hyperlipidemia in these individuals or not.
MATERIALS AND METHODS
The participants of this cross-sectional study were randomly selected with age 20 years and above. Then all consented individuals were tested for hyperlipidemia and subjected to clinical examination of the mouth for the presence and density of the FGs into two main groups; Group I individuals with detectable FGs and Group II individuals with no FGs detected on their labial and oral mucosae.
All recruited participant were issued a written information sheets about the study and those agreed to take part in the study were requested to fast for approximately 9-12 h after which their blood lipid profile test were performed by an ambulatory device (CardioCheck PA Analyzer, Polymer Technology Systems, Inc., Indianapolis, USA).
The blood lipid profile test was carried out through testing total cholesterol (TC), high density lipoprotein (HDL) and calculated low density lipoprotein (LDL). Hyperlipidemia was defined when TC above 200 mg/dL, HDL below 50 mg/dL for females and below 40 mg/dL for males, LDL above 130 mg/dL and TC/HDL cholesterol ratio above 2 was observed.
During the same visit, each participant's mouth was examined by one of the two investigators for the presence and scoring of the FGs [Figure 1]. The later were classified into six groups according to their location:[5] G1-no spots, G2-vermillion border of the lips, G3-buccal unilateral, G4-buccal bilateral, G5-buccal bilateral and vermillion border of the lips, G6-buccal unilateral and vermillion border of the lips.
Figure 1.

Clinical appearance for buccal Fordyce granules
The number of FGs is scored as FG1-0 spots, FG2-up to 6 spots, FG3-6 to 30 spots, FG4-30 to 100 spots and FG5-more than 100 spots.
The age of participants ranged from 20 to 72 years. The individuals were also questioned about all potential risk factors for cardiovascular disorders including history of high cholesterol, smoking, heart disease and hypertension. The participants who revealed a history of elevated cholesterol that is controlled by medication were grouped with those who we discovered there were elevated lipid profile.
The data were tabulated and statistically analyzed using SPSS© edition 19 software (SPSS Inc., Chicago, USA) using the Chi-square test. The significance was set at 0.05. The study was approved by the Ethical Committee at the college of dentistry and a written informed consent was obtained from all participants.
RESULTS
The age of the studied population ranged from 20 to 72 years with no statistical dominance for any specific age group. Men composed about two-thirds of the participants (63.4%). The medical history analysis for the participants revealed that one-third were smokers (n = 113) while the other two-thirds did not report any history of present or past smoking. This relatively low incidence of smoking in the investigated group was reflected in low incidence of hypertension (14.6%) and other heart diseases (7.1%). Both investigators were able to detect the presence of FGs in the majority of the participant (89.7%) with only 36 individuals did not show any signs of the granules on their oral and labial mucosa. The least presentation of the FGs was their detection on only solitary cheek mucosa (5%). The density of the granules varied from undetectable in 36 participants (10.3%) to more than 100 granules/individual in 28 participants (8%). The highest score of density between 30 and 100 granules/individual was reported in 161 participants (46%). The score of density of FGs has shown a noticeable reduction as the age advances [Table 1]. The density of the FGs reaches its peak between age of 30 and 50 years of age. The FGs were reported more often in man and also at a higher density when compared to those noted in women. There was no statistical difference reported between smokers and non-smokers in detection of FGs (93.8% vs. 87.7%). However, more FGs were scored among the non-smokers [Table 2]. The results of this report showed a clear direct proportional relationship between the density of FGs and the level of serum lipids [Table 3]. This statistically significant association reaches the peak when the FGs count is ≥100 granules/individual. Lastly, the individuals with elevated lipid profile tend to display high FGs count located on both cheeks as well as on their vermilion border of the lip. On the other hand, according to the current study, individuals with few granules on one side of buccal mucosa or those with isolated labial spots are unlikely to show an elevated serum lipid. The hyperlipidemia was also tested for the individual age groups and statistical significance between the groups (P = 0.003) reached above 50 years of age which correspond to high density of the FGs.
Table 1.
The age distribution and the score for FGs
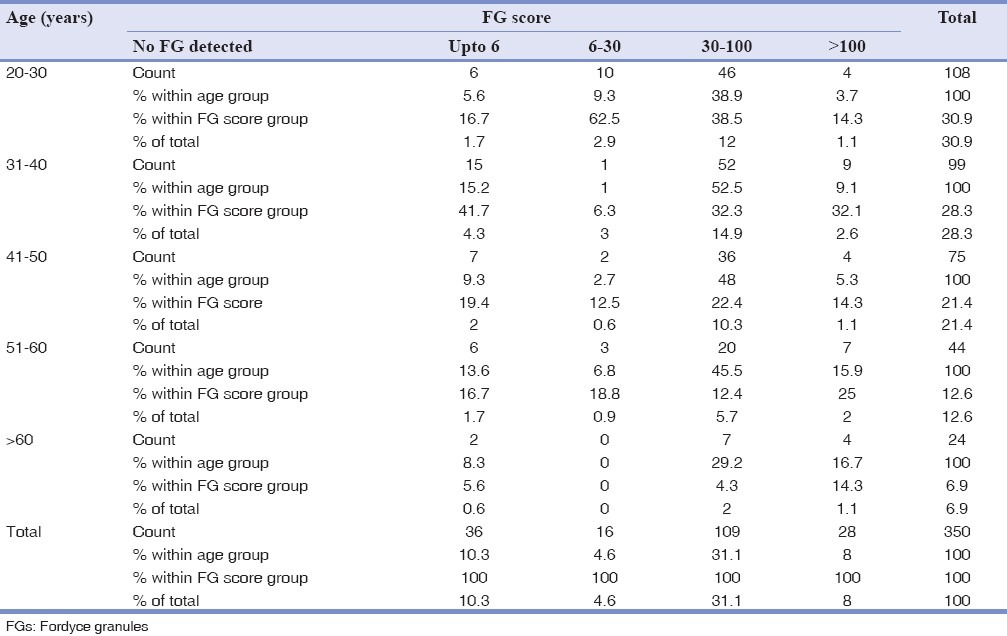
Table 2.
The relationship between smoking and FGs score
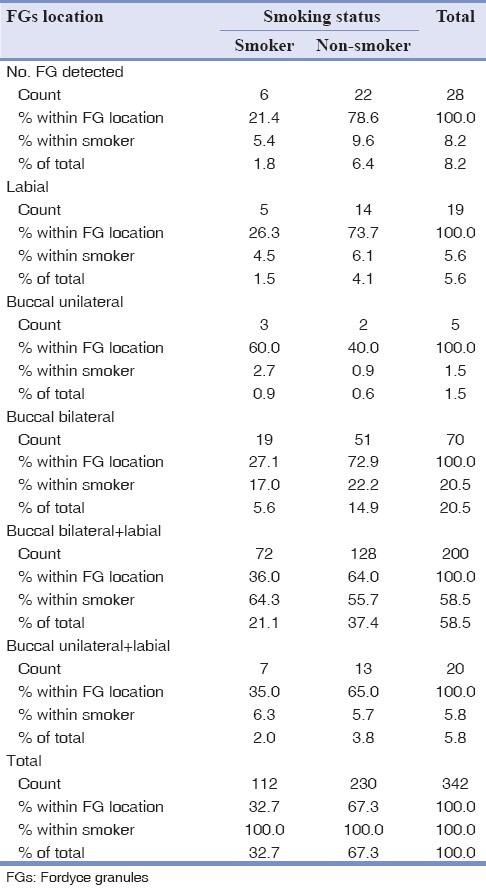
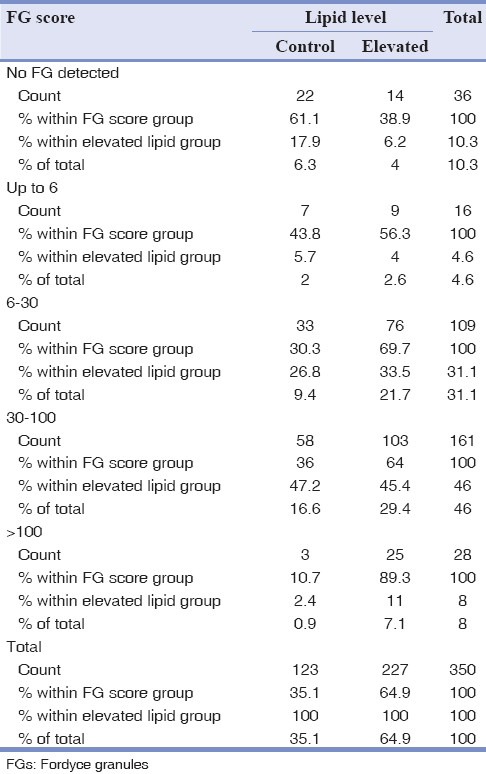
Table 3.
The relationship between the FGs score and the level of lipid
DISCUSSION
The presence of FGs is largely considered as a normal variation of the oral mucosal phenotypes[2] and lots of studies have investigated their incidence in relation to the age, puberty and sex.[5,6,7,8,9,10] The majority of the studies do not consider the relation of these spots with systemic diseases although there are few studies about the pathogenesis of the spots and autoimmune disease.[11] The lipid composition of FGs had been studied and it was reported to be the same lipid composition seen on skin's sebaceous glands.[6]
Cardiovascular disease is the most common cause of death in industrialized countries and hyperlipidemia can lead to accelerated atherosclerosis and premature death from ischemic heart disease.[12,13] The risk of developing atherosclerosis is directly related to the plasma LDL cholesterol and inversely related to the HDL cholesterol level.[12,13,14,15,16,17] In 2003, a national survey was done by American Heart Association, which demonstrated that public awareness of cholesterol education and management was suboptimal and health care providers have a unique role on public education to improve the management of this health issue.[18]
In the present study, the FGs were detected in the vast majority of the participants. This was in accordance with many previous reports.[5,7,19,20] However, there were some studies which reported much lower prevalence of the FGs.[8,9,10] This can be explained by the inconsistency of the examination criteria in defining the appearance of these granules, variability of expertise, and meticulousness of the examination of the oral mucosa.
In contrast to previous studies which claimed that the number and density of granules will increase with advance of age,[21,22] statistical values showed that the number of these spots was reduced with advance of age.[23]
Smoking which is recognized as a major risk factor for the development of ischemic heart disease may play a role in obscuring the presence of the FGs in the mouth. This phenomenon may be explained by the increased thickness of the oral epithelia and increased epithelial melanin production in chronic smokers.
In this report, the relationship between the FGs score and elevated lipid profiles was noted. Among the group scoring with 6-30 spots, the number of individuals with elevated lipid profile was double compared to those with normal lipid profile. Furthermore, we noted that when the number of granules increase, the people are more likely to have hyperlipidemia, as in group of people with >100 spots. On the other hand, individuals previously with elevated lipid profile had shown the highest score of granules and more than half of the individuals in the sample presented elevation of lipid profile.
The relationship between the elevated lipid and the increase in the density of FGs has not been reported and may not be easy to explain. However, the literature has described the possible effects of the elevated lipid on the health of skin, but not that for oral mucosa. It was reported that patients with familial hypercholesterolemia may present with xanthoma, which is a yellowish material formed by macrophages with phagocytosed lipid material and collagen fibers. There are different xanthomas based on their clinical and morphological aspects.[24,25] LDL derived from plasma is trapped in the collagen and glycosaminoglycans and oxidized at these sites. The reaction of LDL with macrophages or other cells can explain the modification of LDL into oxLDL, which is taken up mainly by macrophages, thereby promoting the formation of foam cells,[26] which extravasate through the vascular walls and deposit in perivascular connective tissue. On the other hand, it has been reported that hypercholesterolemic patients without clinically manifesting arterial diseases showed an abnormal skin blood flow motion and endothelial dysfunction.[27] None of these findings may directly explain the increased number of FGs in the oral mucosa. The elevated lipid levels may contribute to the appearance of the FGs either by the increase in the fat content of clinical undetectable glands making them easily visible during the oral examination or de novo differentiation of cells leading to more oral FGs. Both assumptions require verification by histological and histochemical studies.
If the finding of this report can be reproduced in a larger study with different population groups and including more age groups like children, it means that dentists as a health-care providers should consider referring patients with high density of FGs for appropriate medical care especially if such individuals show other risk factors for cardiovascular disorders.
CONCLUSION
According to this report, the presence of high numbers of FGs in people with high risk factors for cardiovascular disease should not be neglected.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Neville B, Damn D, Allen C, Bouquet J. 3rd ed. Philadelphia: Saunders Elsevier; 2009. Oral and Maxillofacial Pathology; pp. 7–8. [Google Scholar]
- 2.Bork K, Hoede N, Korting G, Burgdorf WH, Young SK. 2nd ed. Philadelphia: WB Saunders; 1996. Diseases of the Oral Mucosa and the Lips; pp. 240–1. [Google Scholar]
- 3.Neville B, Damm D, White D. 2nd ed. Ontario, Hamilton: BC Decker; 2003. Color Atlas of Clinical Oral Pathology; p. 6. [Google Scholar]
- 4.Antonio N. 6th ed. Missouri: Mosby; 2003. Ten Cate's Oral Histology, Development, Structure and Function; pp. 333–74. [Google Scholar]
- 5.Gorsky M, Buchner A, Fundoianu-Dayan D, Cohen C. Fordyce's granules in the oral mucosa of adult Israeli Jews. Community Dent Oral Epidemiol. 1986;14:231–2. doi: 10.1111/j.1600-0528.1986.tb01541.x. [DOI] [PubMed] [Google Scholar]
- 6.Nordstrom KM, McGinley KJ, Lessin SR, Leyden JJ. Neutral lipid composition of Fordyce's granules. Br J Dermatol. 1989;121:669–70. doi: 10.1111/j.1365-2133.1989.tb08205.x. [DOI] [PubMed] [Google Scholar]
- 7.Halperin V, Kolas S, Jefferis KR, Huddleston SO, Robinson HB. The occurrence of Fordyce spots, benign migratory glossitis, median rhomboid glossitis, and fissured tongue in 2,478 dental patients. Oral Surg Oral Med Oral Pathol. 1953;6:1072–7. doi: 10.1016/0030-4220(53)90220-5. [DOI] [PubMed] [Google Scholar]
- 8.Jahanbani J, Sandvik L, Lyberg T, Ahlfors E. Evaluation of oral mucosal lesions in 598 referred Iranian patients. Open Dent J. 2009;3:42–7. doi: 10.2174/1874210600903010042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.dos Santos PJ, Bessa CF, de Aguiar MC, do Carmo MA. Cross-sectional study of oral mucosal conditions among a central Amazonian Indian community, Brazil. J Oral Pathol Med. 2004;33:7–12. doi: 10.1111/j.1600-0714.2004.00003.x. [DOI] [PubMed] [Google Scholar]
- 10.Bessa CF, Santos PJ, Aguiar MC, do Carmo MA. Prevalence of oral mucosal alterations in children from 0 to 12 years old. J Oral Pathol Med. 2004;33:17–22. [PubMed] [Google Scholar]
- 11.Scully C, Flint SR, Porter SR, Moos KF. 3rd ed. London: Tailor and Francis Group; 2004. Oral and Maxillofacial Disease; p. 520. [Google Scholar]
- 12.Immanuel S, Giantini A, Dharma RS, Samino The role of lipid profile as a risk factor indicator for ischemic stroke at Cipto Mangunkusumo Hospital, Jakarta. Acta Med Indones. 2006;38:11–6. [PubMed] [Google Scholar]
- 13.Nash IS, Mosca L, Blumenthal RS, Davidson MH, Smith SC, Jr, Pasternak RC. Contemporary awareness and understanding of cholesterol as a risk factor: Results of an American Heart Association national survey. Arch Intern Med. 2003;163:1597–600. doi: 10.1001/archinte.163.13.1597. [DOI] [PubMed] [Google Scholar]
- 14.Castelli WP, Wilson PW, Levy D, Anderson K. Cardiovascular risk factors in the elderly. Am J Cardiol. 1989;63:12H–9. doi: 10.1016/0002-9149(89)90110-0. [DOI] [PubMed] [Google Scholar]
- 15.Benfante R, Reed D. Is elevated serum cholesterol level a risk factor for coronary heart disease in the elderly? JAMA. 1990;263:393–6. [PubMed] [Google Scholar]
- 16.Weverling-Rijnsburger AW, Jonkers IJ, van Exel E, Gussekloo J, Westendorp RG. High-density vs low-density lipoprotein cholesterol as the risk factor for coronary artery disease and stroke in old age. Arch Intern Med. 2003;163:1549–54. doi: 10.1001/archinte.163.13.1549. [DOI] [PubMed] [Google Scholar]
- 17.Bhatti MS, Akbri MZ, Shakoor M. Lipid profile in obesity. J Ayub Med Coll Abbottabad. 2000;12:31–3. [PubMed] [Google Scholar]
- 18.Ferris A, Robertson RM, Fabunmi R, Mosca L American Heart Association, American Stroke Association. American Heart Association and American Stroke Association national survey of stroke risk awareness among women. Circulation. 2005;111:1321–6. doi: 10.1161/01.CIR.0000157745.46344.A1. [DOI] [PubMed] [Google Scholar]
- 19.Güleç AT, Haberal M. Lip and oral mucosal lesions in 100 renal transplant recipients. J Am Acad Dermatol. 2010;62:96–101. doi: 10.1016/j.jaad.2009.06.022. [DOI] [PubMed] [Google Scholar]
- 20.Olivier JH. Fordyce granules on the prolabial and oral mucous membranes of a selected population. SADJ. 2006;61:072–4. [PubMed] [Google Scholar]
- 21.Cawson R, Odell E. 6th ed. Edinburgh: Churchill Livingstone; 2000. Essentials of Oral Pathology and Oral Medicine; p. 209. [Google Scholar]
- 22.Pindborg JJ. 5th ed. Copenhagen: Munksgaard; 1992. Atlas of the Disease of the Oral Mucosa; p. 294. [Google Scholar]
- 23.Flinck A, Paludan A, Matsson L, Holm AK, Axelsson I. Oral findings in a group of newborn Swedish children. Int J Paediatr Dent. 1994;4:67–73. doi: 10.1111/j.1365-263x.1994.tb00107.x. [DOI] [PubMed] [Google Scholar]
- 24.Pietroleonardo L, Ruzicka T. Skin manifestations in familial heterozygous hypercholesterolemia. Acta Dermatovenerol Alp Panonica Adriat. 2009;18:183–7. [PubMed] [Google Scholar]
- 25.Klemp P, Halland AM, Majoos FL, Steyn K. Musculoskeletal manifestations in hyperlipidaemia: A controlled study. Ann Rheum Dis. 1993;52:44–8. doi: 10.1136/ard.52.1.44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mori M, Itabe H, Higashi Y, Fujimoto Y, Shiomi M, Yoshizumi M, et al. Foam cell formation containing lipid droplets enriched with free cholesterol by hyperlipidemic serum. J Lipid Res. 2001;42:1771–81. [PubMed] [Google Scholar]
- 27.Rossi M, Carpi A, Di Maria C, Franzoni F, Galetta F, Santoro G. Skin blood flowmotion and microvascular reactivity investigation in hypercholesterolemic patients without clinically manifest arterial diseases. Physiol Res. 2009;58:39–47. doi: 10.33549/physiolres.931351. [DOI] [PubMed] [Google Scholar]