

Abstract
[Purpose] The aim of this study was to estimate the stability of the axillary pad in the axilla during single-crutch walking through kinematic analysis of the crutch position in the horizontal plane. [Subjects] The subjects were 19 healthy young males. [Methods] The subjects were instructed to walk 5 m in a straight line while using a single crutch. This was repeated 10 times. Repeated-measures analysis of variance and Tukey’s honest significance test were used to compare crutch angles across three time points during crutch stance (crutch contact, mid stance and crutch off) for each subject. [Results] A statistically significant effect of time was found in 17 of the 19 subjects. Sixteen of these 17 subjects rotated the crutch externally from crutch contact to crutch off. [Conclusion] External rotation of the crutch throughout the stance phase is important to enable the axillary pad to be held tightly against the chest wall. These results may lead to alterations of the instructions for crutch use and the prevention of falls.
Key words: Crutch walking, Crutch position, Stability of the axillary pad
INTRODUCTION
The axillary crutch is an assistive device used by individuals with gait disturbance due to lower-limb impairments such as fractures or surgery of the hip or knee joint. During crutch walking, users have to hold the axillary pad firmly against their chest wall with their arm and maintain their wrist in a dorsiflexed position on the handgrip to support their weight1, 2). However, if the axillary pad is not held firmly to the chest wall, it can separate from the axilla and this may lead to a fall. In the clinical experience of the first and second authors, the axillary pad often deviates from the axilla during the crutch stance phase crutch training. Sasaki et al.3) reported that crutch use was dangerous when the shoulder joint was placed in an internally rotated position (IRP), because the axillary pad is not fixed to the chest wall and could easily slide backward from the axilla. They suggested that a horizontally positioned shoulder joint was important to ensure that the axillary pad was securely positioned against the chest wall.
The position of shoulder joint in the horizontal plane determines the position of the crutch in the horizontal plane during crutch walking. Though supination or pronation of the forearm and radial or ulnar deviation of the wrist influence the position of the crutch, the position of the shoulder joint has the greatest influence3, 4). Therefore, we hypothesized that the position in the horizontal plane of the axillary pad could be used to estimate the stability of the axillary pad during crutch walking.
The aim of this study was to estimate the stability of the axillary pad in the axilla during single-crutch walking using kinematic analysis of the crutch position in the horizontal plane.
SUBJECTS AND METHODS
The subjects were 19 healthy young males (mean age, 22.2 ± 0.4 years; mean height, 171.4 ± 5.5 cm; mean weight; 67.4 ± 8.2 kg). This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of Kyushu University of Nursing and Social Welfare. All subjects received a description of this study and provided their written informed consent before participating in the study. Before measurements were made, all subjects were provided with a crutch of an appropriate length and practiced using the crutch. The appropriate crutch length was determined using the standard method described by Rusk and Lowman5, 6). Single-crutch walking was performed with a pseudo-affected left leg and an unaffected right leg. Subjects were instructed to put 30% of their body weight on the crutch7,8,9,10), which substituted for the left leg, and performed two-point gait by swinging the unaffected side out in front of the crutch.
The experimental set-up consisted of a Vicon MX13 three-dimensional motion capture system (Vicon Peak, UK), comprising eight infrared cameras, six force plates (AMTI, USA) and a digital video camera (Victor, JVC, Japan). The sampling rates of the motion capture system and the force plates were 100 Hz. Two infrared reflective markers were placed on an extension that was attached to the axillary pad so that a straight line connecting the two markers indicated the long axis of the axillary pad. Subjects were instructed to walk 5 m in a straight line using the single crutch, and this was repeated 10 times. Walking speed and step length were determined by the subject.
The position of the crutch in the horizontal plane was defined as the angle between the sagittal (Y-Z) plane and the long axis of the axillary pad, and it was calculated using data collected by the motion capture system. The value of the angle was negative when the crutch turned toward the body (internal rotation) and positive when the crutch turned away from the body (external rotation; Fig. 1). The stance phase of the crutch during walking was identified from the ground reaction force data. Crutch contact was defined as the point at which the crutch tip was grounded on the floor, mid stance was defined as the point at which the anterior-posterior ground reaction force had a value of zero, and crutch off was defined as the point at which the crutch tip was taken off the floor.
Fig. 1.
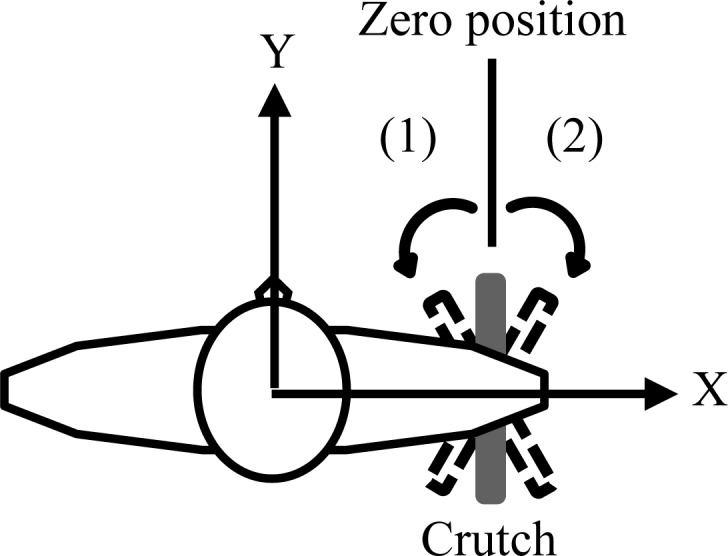
Definition of crutch angle. (1) Indicates internal rotation and (2) indicates external rotation.
Repeated-measures analysis of variance and the Tukey’s honest significance test were used to compare the crutch position across the three phases of stance for each subject. All data were analyzed using standard statistics software (IBM SPSS Statistics ver. 19.0). p values of less than 0.05 were considered significant.
RESULTS
Table 1 shows the crutch angle in each phase of crutch stance for each subject. The crutch angle was significantly different across the crutch stance phases for 17 of the 19 subjects. Posthoc comparisons indicated statistically significant differences (Tukey’s honest significance test) for 15 out of the 17 subjects in the following three comparisons: (1) crutch contact vs. mid stance, (2) crutch contact vs. crutch off, and (3) mid stance vs. crutch off. As for the remaining two subjects, one subject showed statistically significant differences for: (1) crutch contact vs. mid stance, and (2) crutch contact vs. crutch off; and the other subject showed a statistically significant difference for: (3) mid stance vs. crutch off.
Table 1. Crutch angle in each phase of stance for each subject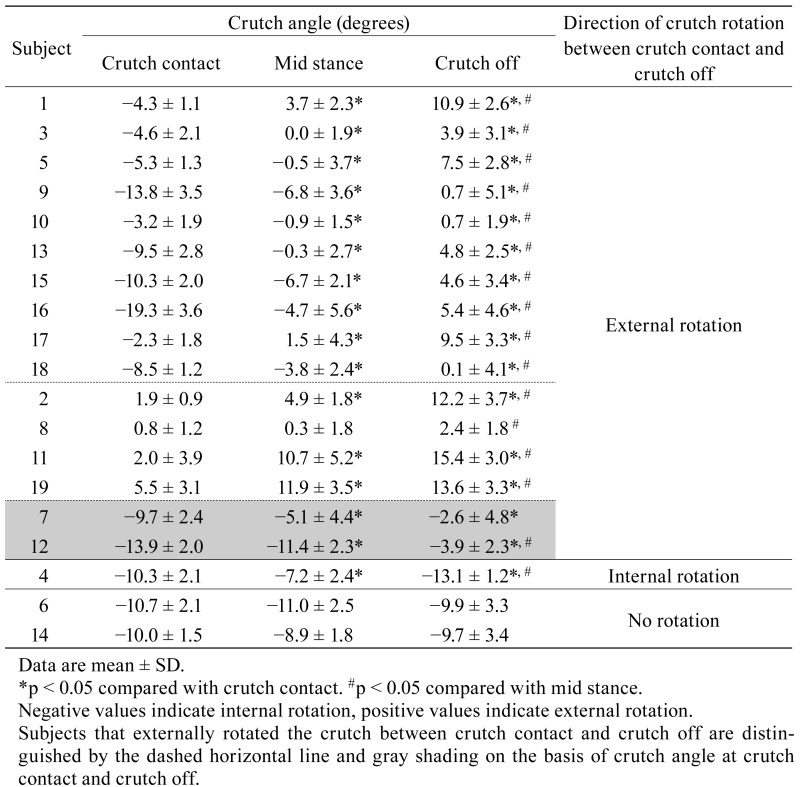 .
.
DISCUSSION
Many diverse studies of crutch walking have been performed by researchers. For example, the study of appropriate crutch length6, 11, 12), the study of energy cost13), the study of crutch palsy or fracture14, 15), and the kinematic or kinetic study of the upper and lower extremities16,17,18,19,20,21,22). However, we were not able to find a study on the stability of the axillary pad in the axilla. We hypothesized that the stability of the axillary pad in the axilla is one of the main issues for safe crutch walking. Our study is the first attempt using kinematic analysis of the crutch position to examine the stability of the axillary pad during crutch walking.
We found that although there was inter-subject variation in the value of the angle, the crutch externally rotated in the horizontal plane during the crutch stance phase for 16 subjects. For the remaining three subjects, the crutch rotated internally or did not rotate during the crutch stance phase.
The external rotation of the crutch that was observed for 16 subjects, likely occurred because of the shape of the chest wall, the position of the shoulder joint, and the fact that the axillary pad was held firmly against the chest wall. Normally, the axillary pad is held to the chest wall by the shoulder adductor muscles1). If the shape of the chest wall is assumed to be a plane (Fig. 2a), the shoulder joint needs to move in flexion and extension in addition to adduction during crutch walking to hold the axillary pad stably against the chest wall. If this were the case, the shoulder joint and the axillary pad would not rotate. However, because the chest wall has a rounded shape, the axillary pad moves along the chest wall, and the shoulder joint and the axillary pad rotate to hold the axillary pad stably against the chest wall. That is to say, internal rotation occurs when the shoulder joint flexes and external rotation occurs when shoulder joint extends (Fig. 2b). We propose that the rotation of the shoulder joint and the axillary pad is very important for holding the axillary pad firmly to the chest wall.
Fig. 2.
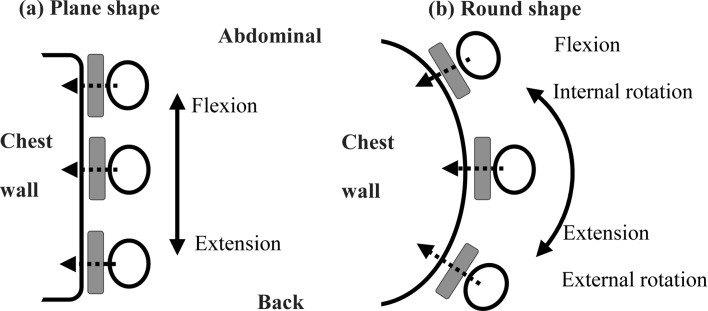
Relation between the shape of the chest wall and the position of the shoulder joint in the horizontal plane Grey rectangles indicate the crutch, open circles indicate the arm, dotted arrows indicate the direction of the force of shoulder adductors, and black arrows indicate the position of the shoulder joint.
Figure 3 shows a conceptual illustration of this idea. At crutch contact, the shoulder joint is in a position of flexion, adduction and internal rotation because the crutch is grounded in front of the body. Therefore the crutch is located in an IRP. From crutch contact to mid stance, the body is moving forward. Throughout this period the shoulder joint extends; then, both the shoulder joint and the crutch rotate from the IRP toward an externally rotated position (ERP). Around mid stance, the crutch is located by the side of the body. From mid stance to crutch off, the body continues to move forward and the crutch is positioned to the rear of the body. Throughout this period the shoulder joint extends, adducts and externally rotates and the crutch continues to externally rotate. Accordingly, we showed that the crutch was grounded in an IRP, and then rotated externally throughout the crutch stance phase and was taken off the floor in an ERP.
Fig. 3.

Conceptual illustration of the position of the crutch during the crutch stance phase
In this study, we found that this movement pattern was present for 10 of the 16 subjects that showed a statistically significant difference in crutch angle across the three phases. For four of the 16 subjects the crutch was located in an ERP at crutch contact and for the remaining two subjects the crutch was located in an IRP at crutch off. However, all 16 subjects the crutch externally rotated from crutch contract to toward crutch off, showing a similar pattern to that illustrated in Fig. 3. We propose that these 16 subjects were able to hold the axillary pad stably against the chest wall because of the relative positions of the crutch and the chest wall. For two of the remaining three subjects the crutch maintained a similar angle throughout the crutch stance phase, and for one subject the crutch internally rotated throughout the crutch stance phase. We propose that these three subjects had an unstable connection between the axillary pad and the chest wall because of the relative positions of the crutch and the chest wall. Therefore, we conclude that external rotation of both the shoulder joint and the crutch was important for holding the axillary pad against the chest wall.
Maximum weight-bearing by the crutch usually occurs around mid stance. If the crutch externally rotates around the time of mid stance, it will be held stably to the chest wall at this time. As a result, the axillary pad will not easily separate from the axilla, even if a large movement in the anterior-posterior direction is exerted on the crutch. In contrast, the axillary pad would easily separate from the axilla if it were not sufficiently fixed to the chest wall due to internal rotation or lack of rotation. Sasaki et al. suggested that a horizontally positioned shoulder joint was important to ensure that the crutch axillary pad is securely positioned against the chest wall. Additionally, the results of our study suggest that external rotation of both the shoulder joint and the crutch is important for holding the axillary pad against the chest wall during the crutch stance phase. Therefore, not only the position but also appropriate rotation of the crutch is necessary for a stable connection between the axillary pad and the chest wall.
In conventional instructions for crutch use, users are asked to put the axillary pad tightly under their arm. However, we think this instruction is not sufficient, and that crutch users should be instructed to externally rotate the crutch during the crutch stance in order to decrease the likelihood of the axillary pad separating from the axilla, thereby reducing the risk of a fall.
In conclusion, we are confident that our study reproduced the 30% partial weight bearing crutch walking from the ground reaction force data. Accordingly, we think that the subjects successfully imitated the crutch walking of patients in our experiment. However, because the subjects were healthy, their physical ability to support the affected side was different from that of patients. Therefore, we think our findings are not sufficient to recommend their application in clinical settings. Further studies of kinetic analysis of the crutch, comparison of the crutch walking pattern, and selection of the subjects are needed to confirm our findings.
Acknowledgments
Part of this work was supported by JSPS KAKENHI Grant Number 25560273 and Grants-in-Aid for Research and Development Projects of Small and Medium-sized Enterprises of the industry-academia-government collaboration of the Kitakyushu Foundation for the Advancement of Industry, Science and Technology (FAIS).
REFERENCES
- 1.Hoberman M, Basmajian JV: Crutch and cane exercises and use, Basmajian JV (Ed.), Therapeutic exercise, 4th ed. Baltimore: Williams and Wilkins, 1984, pp 267-284. [Google Scholar]
- 2.Hashimoto T: Tsue•hokouhozyogu no syurui to dousasyougai ni oujita mochiikata no youtenn. Rigaku Ryoho, 2010, 27: 192–207 (in Japanese). [Google Scholar]
- 3.Sasaki S, Nose Y, Shimada S, et al. : The biomechanics of crutches and canes. Rigaku Ryoho, 2000, 17: 814–823 (in Japanese). [Google Scholar]
- 4.Sasaki S, Shimada S, Nakayama Y, et al. : Denkikakudokei niyoru syukansetu no undoukaiseki: tokuni hozyogu wo mochiita idoudousa nituite. Jpn Phys Ther Assoc, 1987, 14: 178.(in Japanese). [Google Scholar]
- 5.Lowman EW, Rusk HA: Self-help devices, crutch prescription: measurement. Postgrad Med, 1962, 31: 303–305. [Google Scholar]
- 6.Bauer DM, Finch DC, McGough KP, et al. : A comparative analysis of several crutch-length-estimation techniques. Phys Ther, 1991, 71: 294–300. [DOI] [PubMed] [Google Scholar]
- 7.Jebsen RH, Jebsen RH: Use and abuse of ambulation aids. JAMA, 1967, 199: 5–10. [PubMed] [Google Scholar]
- 8.Takeuchi T: Kokansetu-sikkan no rigakuryoho. Rinsho Rigaku Ryoho, 1981, 8: 95–113 (in Japanese). [Google Scholar]
- 9.George V: Crutches, canes, and walkers, Redford JB (Ed.), Orthotics etcetera, 3rd ed. Baltimore: Williams and Wilkins, 1986, pp 453-463. [Google Scholar]
- 10.Seki K, Morohashi I, Kamata I, et al. : Gait analysis of axillary crutch gait: the first report. Tohoku Rigaku Ryohogaku, 2003, 15: 13–18 (in Japanese). [Google Scholar]
- 11.Beckwith JM: Analysis of methods of teaching axillary crutch measurement. Phys Ther, 1965, 45: 1060–1065. [DOI] [PubMed] [Google Scholar]
- 12.Crosbie J, Armstrong E, Kempson J: Is walking aid height critical? Aust J Phys Ther, 1992, 38: 261–266. [DOI] [PubMed] [Google Scholar]
- 13.Mullis R, Dent RM: Crutch length: effect on energy cost and activity intensity in non-weight-bearing ambulation. Arch Phys Med Rehabil, 2000, 81: 569–572. [DOI] [PubMed] [Google Scholar]
- 14.Raikin S, Froimson MI: Bilateral brachial plexus compressive neuropathy (crutch palsy). J Orthop Trauma, 1997, 11: 136–138. [DOI] [PubMed] [Google Scholar]
- 15.Garcia Suarez G, Garcia Garcia J, Perez Carro L: Stress fracture of the ulna associated with crutch use. J Orthop Trauma, 2001, 15: 524–525. [DOI] [PubMed] [Google Scholar]
- 16.Wilson JF, Gilbert JA: Dynamic body forces on axillary crutch walkers during swing-through gait. Am J Phys Med, 1982, 61: 85–92. [PubMed] [Google Scholar]
- 17.Reisman M, Burdett RG, Simon SR, et al. : Elbow moment and forces at the hands during swing-through axillary crutch gait. Phys Ther, 1985, 65: 601–605. [DOI] [PubMed] [Google Scholar]
- 18.Shiokawa K: [Dynamic roles of the upper extremity during axillary crutch gait]. Nippon Seikeigeka Gakkai Zasshi, 1993, 67: 1014–1025(in Japanese). [PubMed] [Google Scholar]
- 19.Li S, Armstrong CW, Cipriani D: Three-point gait crutch walking: variability in ground reaction force during weight bearing. Arch Phys Med Rehabil, 2001, 82: 86–92. [DOI] [PubMed] [Google Scholar]
- 20.Soma T, Onishi H, Oyama M, et al. : Electromyography analysis of shoulder joint muscles in standing with three ambulatory aids. J Phys Ther Sci, 2007, 19: 117–123. [Google Scholar]
- 21.Lee JU, Kim MY, Kim JH, et al. : Analysis of plantar foot pressure during the non-crutch, two-point, and four-point crutch gait performed by healthy volunteers. J Phys Ther Sci, 2011, 23: 489–493. [Google Scholar]
- 22.Lee JU, Kim JH, Lee LK, et al. : Posture analysis of various types of crutch gait of healthy volunteers. J Phys Ther Sci, 2013, 25: 453–458. [Google Scholar]