

Abstract
Within dysphoria, rumination has been identified as a particularly maladaptive emotion regulation strategy linked to prolonged negative affect and the onset of depressive episodes. Until now, the majority of research assessing naturally occurring rumination has utilized trait rumination measures; however, additional information may be obtained by assessing state rumination. The current study examined the association between state rumination and participants’ emotional recovery from stress. In addition, biased attention toward emotional information was investigated as a mechanism that might underlie state rumination. Participants completed the exogenous cuing task to assess attentional engagement and disengagement from emotional facial expressions followed by a psychosocial stressor. State rumination and self-reported sadness were measured during the recovery period. As expected, state rumination was associated with less recovery in sadness scores, even after controlling for trait rumination and depressive symptoms. Moreover, within the high dysphoria group, participants who had more difficulty disengaging from emotional expressions reported higher levels of rumination in response to the stressor. Results highlight an important association between state rumination and individuals’ recovery from stress, and suggest that difficulty disengaging attention from emotional expressions might be one mechanism underlying state rumination in dysphoria.
Keywords: dysphoria, attention bias, state rumination, stress
Introduction
Diathesis-stress models of depression propose that stress plays an important role in triggering the onset of a depressive episode (e.g., Hammen, 2005; Monroe & Simons, 1991). Increasing evidence suggests that people at risk for depression differ from their non-vulnerable counterparts in their recovery from negative affect (e.g., Teasdale, 1988). It is therefore critical to understand factors that hinder recovery from stress. Individual differences in the tendency to respond to negative events and negative affect with rumination has been proposed as an important mechanism that interferes with recovery, and may thereby increase risk for the onset of depression (e.g., Nolen-Hoksema, Wisco, & Lyubomirsky, 2008).
Rumination is a maladaptive response strategy defined by repetitively and passively thinking about one’s negative emotions and the events that caused them (e.g., Nolen-Hoeksema et al., 2008). In the context of either naturally occurring or experimentally induced negative mood, rumination is associated with prolonged distress and sadness, a hallmark symptom of depression (see Nolen-Hoeksema et al., 2008, for a review). The tendency to ruminate in response to distressing events has also been linked to numerous maladaptive outcomes, including higher risk for the onset of a major depressive episode (e.g., Nolen-Hoeksema, 2000; Nolen-Hoeksema et al., 2008).
Rumination is typically examined in one of two ways. Individual differences in trait rumination can be assessed with the Ruminative Responses Scale (RRS; Nolen-Hoeksema, Larson, & Grayson, 1999). Participants are asked to rate what they generally do when they feel sad or depressed on a four-point Likert scale ranging from 1 (almost never) to 4 (almost always). Items assess what people typically think about or do during times of sadness. It does not, however, assess the amount an individual is ruminating at the current moment or in response to an acute stressor, and is therefore subject to biases often associated with retrospective report (Stone et al., 1998). The second way that rumination has been examined is via Nolen-Hoeksema and Morrow’s (1993) response styles manipulation, during which rumination is induced in the laboratory. Participants in the rumination induction are asked to read statements for 8 minutes that encourage them to focus on the meanings and causes of their current negative emotions. This is typically contrasted with a distraction induction, in which participants are asked to read statements for 8 minutes that encourage them to focus on ideas and images not personally relevant. Although the response styles manipulation has been critical in determining short- and long-term consequences of rumination (e.g., see Nolen-Hoeksema et al., 2008, for a review), it does not allow us to examine the amount people naturally ruminate in response to an acute stressor, referred to as state rumination. Recent studies have therefore started to focus on assessing state rumination, and results suggest meaningful differences between state and trait rumination. Moberly and Watkins (2008), for example, examined how state and trait rumination influenced negative affect. State rumination, which was assessed by asking participants the extent they were focused on feelings and problems at the current moment, predicted subsequent negative affect independent of the effects of trait rumination. Moreover, studies have documented inconsistent stability of trait rumination over time. Although test-retest correlations of the RRS are typically greater than .60 (Nolen-Hoeksema, 2000; Nolen-Hoeksema, Parker, & Larson, 1994), correlations below .40 have been found within depressed samples (e.g., Kasch, Klein, & Lara, 2001). This suggests that rumination is not a static construct but rather one that can change over time, underscoring the importance of assessing state rumination.
Given the substantial consequences of rumination, it is important to identify mechanisms that might underlie ruminative tendencies in depression. It has been proposed that individual differences in the way people process information might contribute to rumination (e.g., De Raedt & Koster, 2010; Joormann & D’Avanzato, 2010; Koster, De Lissnyder, Derakhshan, & De Raedt, 2011). For example, Joormann and Gotlib (2010) found an association between rumination and difficulty inhibiting the processing of negative information, which was specific to the group of depressed patients. Similarly, Donaldson and colleagues examined the link between rumination and biased attention toward negative information and found that this association held within the depressed group (e.g., Donaldson, Lam, & Mathews, 2007). Until now, however, work in this area has focused on the association between attention biases and trait rumination – rather than naturally occurring state rumination in response to an acute stressor.
When studying attention, increasing evidence suggests that it is not a unitary construct. Rather, it can be separated into people’s initial engagement with a stimulus from people’s subsequent disengagement from it. This distinction is important when thinking about risk for depression. Models of depression suggest depression and dysphoria are characterized not by biases in the initial engagement but rather by biases in the subsequent disengagement from negative stimuli. In support of this model, depressed and dysphoric people showed attention biases for negative information when stimuli were presented for longer durations (e.g., Gotlib, Krasnoperova, Yue, & Joormann, 2004; Joormann & Gotlib, 2006) but not when stimuli were presented only briefly (e.g., Mogg & Bradley, 2005). More specific support for this model comes from work using attention task that directly assesses initial attentional engagement and the subsequent attentional disengagement (e.g., Koster, De Raedt, Goeleven, Franck, & Crombez, 2005). Results suggest that attention biases in dysphoria are specific to difficulty disengaging from negative stimuli. It is possible that, in dysphoria, difficulty disengaging attention from negative material is associated with difficulty disengaging thoughts from negative material (a.k.a., rumination). In fact, findings in dysphoria indicate difficulty disengaging attention from negative stimuli is associated with higher trait rumination (e.g., see Joormannn & D’Avanzato, 2010, for a review), and it is important to see if a similar connection exists with state rumination in response to an acute stressor.
The current study had two primary goals. We first sought to establish the association between state rumination and participants’ emotional recovery from a laboratory stressor. Even after controlling for depressive symptoms and trait rumination, we predicted that higher state rumination is associated with prolonged sadness in response to the stressor, evidenced by less recovery in sadness ratings. Particular focus was given to examining sad mood in response to the emotional stressor given evidence of increased risk for depression – a hallmark symptom of which is sad mood – following stressful life events (e.g., Monroe & Hidjiyannakis, 2002), chronic stress (e.g., Brown & Harris, 1986), and daily hassles (e.g., Lazarus & Folkman, 1984). Moreover, authors have suggested that it is reasonable to expect increased sadness in response to stress and indicated that this might be examined in future research (e.g., Moons, Eisenberger, & Taylor, 2010). The second goal of the current study was to identify mechanisms that are associated with greater state rumination in individuals scoring high versus low on a dysphoria measure. Given initial evidence that the association between cognitive biases and rumination is specific to depressed and dysphoric participants (e.g., Donaldson et al., 2007; Joormann & Gotlib, 2010), a positive correlation between difficulty disengaging attention from negative stimuli and state rumination was expected only in the high dysphoria group. Attentional engagement was not expected to be correlated with state rumination in either group.
Method
Participants
Undergraduate students at the University of Miami were recruited from Introduction to Psychology courses. Eighty-three participants, 42 females and 37 males, completed the study in partial fulfillment of their course requirement. Mean age was 19.48 years (SD = 3.06).1 The sample consisted of diverse ethnic groups: 45.8% were Non-Hispanic White, 24.1% were Hispanic, 12.0% were Asian, 8.4% were Black, and 9.7% reported ‘other’ ethnicity.
Exogenous Cuing Task (ECT)
Stimuli
Photographs of emotional (happy, sad, and angry) and neutral facial expressions were selected from the MacBrain Face Stimulus Set (http://www.macbrain.org/resources.htm), which was developed by the Research Network on Early Experience and Brain Development. The current study utilized 12 male and 12 female faces, each displaying all four expressions. Eight of the models were Black and sixteen were White. Photographs of eight additional models were used during the practice trials. Photographs were presented in color and were cropped at the hair line, below the chin, and past each ear.
Design
Participants completed an emotional modification of the ECT (Posner, 1980; Koster et al., 2005) as a measure of attentional biases. Stimuli were presented against a black background. Each trial began with two white frames (each consuming 40% of the width of the screen and 53% of the height of the screen) presented side-by-side for 499ms (see Figure 1). Next, a photograph of a facial expression appeared in one of the two frames for 200ms, and it was immediately masked by a 50 ms presentation of the two white frames. Finally, an “E” or an “F” appeared on the left or right side of the screen and remained until participants indicated the letter that was shown. Participants were asked to respond as quickly and accurately as possible by pressing one of two keys on a standard keyboard. The subsequent trial began immediately after a response was received.
Figure 1.
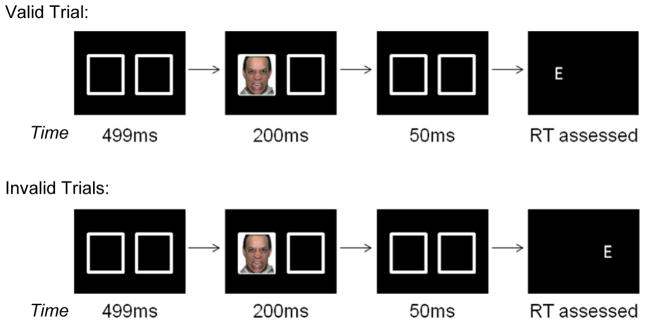
Stimulus presentation on valid and invalid trials
Unbeknownst to participants, two different trial types are utilized in the ECT. Valid trials are those where the photograph and letter appear on the same side of the screen; the photograph is therefore a valid indicator of where the letter will appear. Invalid trials are those where the photograph and letter appear on opposite sides of the screen; the photograph is therefore an invalid indicator of where the letter will appear. For each expression type, participants viewed 24 valid and 24 invalid trials. Photographs were displayed equally often on the left as on the right side of the screen. Trial order was randomized across expression type (happy, sad, angry, vs. neutral), trial type (valid vs. invalid), and location of photograph (right vs. left). Practice trials differed from the main experimental trials in that participants received feedback regarding the accuracy of their responses.
Psychosocial Stressor
Participants completed a psychosocial stressor that began with a 10-minute calming nature video, during which the experimenter left the room. Following, participants completed a three-part psychosocial stressor in the presence of the experimenter. Stress tasks with both social evaluation and uncontrollability were selected given that this combination is especially effective in eliciting distress (see meta-analysis by Dickerson & Kemeny, 2004). Participants were told that they would complete several tasks to “evaluate different aspects of their intelligence,” which would be judged by the experimenter and videotaped so that it could also be evaluated by a panel of their peers. The first two tasks were adapted from the Trier Social Stress Test (Kirschbaum, Pirke, & Hellhammer, 1993), a well-validated stressor. The first was a speech task. Participants were given two minute to prepare and five minute to present an argument for or against global warming. During the speech, the experimenter maintained a neutral expression and appeared to make notes on an evaluation sheet. If participants finished early, the experimenter said the amount of time remaining and recommended that participants use this time to add to their argument. Immediately following the speech, participants were given five minutes to count backwards from 2,083 to zero in 13-step sequences. When an error was made, the experimenter would respond with “error; 2,083,” thereby prompting the participant to start again at the beginning. Finally, participants completed a computer-based anagram test. Participants were given five minutes to solve as many anagrams as possible but allowed only 30 seconds to solve each anagram. Approximately 30% of the anagrams were unsolvable. The task was adapted from MacLeod, Rutherford, Campbell, Ebsworthy, & Holker (2002) and has been shown to induce stress in participants (e.g., Bushman, Bonacci, Pedersen, Vasquez, & Miller, 2005; MacLeod et al., 2002; Salemink, van den Hout, & Kindt, 2009). During the recovery period, participants watched another calming nature video for 30 minutes.
Measures
Sadness ratings
Participants reported the amount of sadness they felt at seven points. Responses were made on an 11-point Likert scale ranging from 0 (not at all) to 10 (very much). Sadness ratings were made before the first nature video (Baseline1), immediately after the first nature video (Baseline2), in the middle of the stressor (Stress), and at the start and minutes 10, 20, and 30 of the second nature video (Recovery1, Recovery2, Recovery3, and Recovery4 respectively).
Anxiety ratings
Anxiety ratings were provided as a check of whether participants experienced an increase in stress in response to the stressor. Ratings were also made on an 11-point Likert scale ranging from 0 (not at all) to 10 (very much) at the following time points: before the first nature video (Baseline1), immediately after it (Baseline2), in the middle of the stressor (Stress), and at the start of the second nature video (Recovery1).
The State Rumination Questionnaire (SRQ)
Participants completed a 10-item measure assessing the extent of state rumination in response to the stressor. Questions from the SRQ were adapted based on both the definition of rumination put forth by the response styles theory (Nolen-Hoeksema et al., 2008) as well as the Ruminative Responses Scale of the Response Style Questionnaire (Nolen-Hoeksema & Morrow, 1991). Seven questions assessed people’s thoughts about the stressor. For example, “In the time since you completed the intelligence tasks…To what extent did you think about how sad or upset you felt?” Responses were provided on a 5-point Likert scale that ranged from 1 (Not at all) to 5 (A lot). In addition, 3 questions clarified the valence of their thoughts on a 5-point Likert scale, which was anchored at 1 (Negative), 3 (Neutral), and 5 (Positive) and reverse scored. These questions were added to assess the extent to which participants’ thoughts focused on symptoms of distress, an integral part of the rumination definition (e.g., Nolen-Hoeksema et al., 2008). Table 1 presents all questions included in the SRQ. Internal consistency was α = .70.
Table 1.
State Rumination Questionnaire
| Questions |
|---|
| To what extent did you think about your performance on the intelligence tasks in the time since you completed them? |
| Were your thoughts about your performance Negative, Neutral, or Positive? |
| To what extent did you criticize yourself about your performance? |
| How much did you think about other past performance on school related or intelligence tasks? |
| Were your thoughts about past performances Negative, Neutral, or Positive? |
| To what extent did you think about the anxiety you felt during the interaction? |
| To what extent did you avoid thinking about your performance on the intelligence tasks in the time since you completed them? |
| How much did you think about how sad or upset you felt? |
| To what extent did you reply parts of what happened in your mind? |
| Were these replayed thoughts Negative, Neutral, or Positive? |
Response Styles Questionnaire (Nolen-Hoeksema & Morrow, 1991)
The 22-item ruminative responses scale (RRS) of the Response Styles Questionnaire (Nolen-Hoeksema & Morrow, 1991) was used to assess trait rumination. Participants were asked to indicate what they generally do when they feel down, sad, or depressed on a 4-point Likert scale ranging from 1 (Almost Never) to 4 (Almost Always).
Center for Epidemiological Studies-Depression Scale (CESD; Radloff, 1977)
The CESD was used to assess depressive symptoms within the past two months. Participants used a 4-point Likert scale that ranged from 0 (Rarely) to 3 (Most of the time) to indicate how often they experienced 20 symptoms related to depression.
Procedure
Participants met individually with an experimenter who oriented them to the ECT and read the instructions aloud. Following the practice trials, the experimenter left the room. When participants completed the ECT, they met a second experimenter, who wore a white laboratory coat, maintained a neutral expression, and provided terse responses if asked any questions. Experimenter 2 brought participants to a new laboratory room located within the same building. Experimenter 2 then turned on the first nature video and left the room.
At the end of the nature video, Experimenter 2 returned and informed participants that they were to complete several tests designed to assess different aspects of their intelligence. Participants then completed the speech and arithmetic tasks while being videotaped. The video camera was turned off following the arithmetic task, and participants were seated at the computer in order to complete the anagram task.
During the recovery period, Experimenter 2 left the room and participants watched a second calming nature video. Lastly, participants were asked to complete several questionnaires, first the SRQ, followed by the RRS and the CESD. Before leaving, participants were debriefed and given course credit.
Results
Manipulation Check
As a check of the effectiveness of the stressor, we examined participants’ anxiety ratings from Baseline1 through Recovery1 (Baseline1, Baseline2, Stress, Recovery1). The repeated-measures analysis of variance (ANOVA) demonstrated a significant main effect of time, F(3, 237) = 21.75, p < .001, η2 = .22. Follow-up paired-samples t-tests demonstrated a significant decrease from Baseline1 (M = 1.18, SD = 1.47) to Baseline2 (M = 0.64, SD = 1.31), t(79) = 5.19, p < .01, followed by a significant increase from Baseline2 to Stress (M = 2.20, SD = 2.20), t(81) = 6.93, p < .01, suggesting the stressor effectively induced anxiety. Participants’ anxiety ratings then significantly decreased from Stress to Recovery1 (M = 1.74, SD = 2.18), t(81) = 2.14, p < .05, suggesting recovery after stressor offset.2
State Rumination and Sadness
Next we investigated whether state rumination was associated with less recovery in sadness ratings. A paired-sample t-test indicated a significant increase in sadness from Baseline2 to Stress in response to the psychosocial stressor, t(79) = 2.72, p < .01. Given that variability between initial scores can be problematic in repeated measures analyses, residualized scores were calculated. This approach is increasingly preferred in repeated-measures analyses to statistically control for variability in earlier scores (e.g., baseline scores when examining reactivity; e.g., Segal et al., 2006) given that the variability among residuals is considered independent from the earlier score (Cohen, Cohen, West, & Aiken, 1983). Residualized scores were first calculated for stress reactivity. Using a linear regression, sad scores at Baseline2 were used to predict sad scores at Stress, and the standardized residual (Zres-Reactivity) was derived. Similarly, when focused on the recovery period, linear regressions were used to predict sad scores during Recovery1 to Recovery4 by sad scores at Stress. Standardized residuals (Zres-Recovery1, Zres-Recovery2, Zres-Recovery3, and Zres-Recovery4) were saved from each regression. The following analyses were therefore conducted using the residualized scores.
To determine whether participants’ initial increase in sadness was associated with their state rumination, we ran a simple linear regression predicting Zres-Reactivity from SRQ. CESD and RRS scores were also included in the model to control for depressive symptoms and trait rumination. This model did not predict a significant portion of variance in reactivity scores (see Table 2). To test our hypothesis that state rumination would affect participants’ subsequent recovery from stress, we ran linear regressions with SRQ predicting Zres-Recovery1 through Zres-Recovery4. CESD and RRS scores were also included in the model to control for depressive symptoms and trait rumination. Each regression model predicted a significant portion of variance in the recovery scores (see Table 2). SRQ scores, but not CESD or RRS scores, predicted a significant portion of variance in sadness recovery in all regressions. More specifically, at all time points, higher SRQ scores were associated with less recovery in sad mood.
Table 2.
Sadness Ratings and Regression Analyses: State Rumination, Trait Rumination, and Mood Predict Sadness Residuals
| Time Points | Sadness Ratings M (SD) |
β
|
R2 | F | ||
|---|---|---|---|---|---|---|
| CESD | RRS | SRQ | ||||
| Stress | 0.47 (1.20) | −0.11 | 0.16 | 0.03 | 0.02 | 0.44 |
| Recovery1 | 0.85 (1.94) | −0.05 | 0.08 | 0.59** | 0.35 | 13.64** |
| Recovery2 | 0.45 (1.49) | −0.00 | −0.14 | 0.48** | 0.23 | 7.66** |
| Recovery3 | 0.41 (1.45) | −0.03 | −0.11 | 0.42** | 0.18 | 5.50* |
| Recovery4 | 0.16 (0.62) | −0.06 | −0.17 | 0.38* | 0.15 | 4.40* |
Note: Regressions calculated using residualized scores. Higher residualized scores at Stress indicate greater reactivity to the stressor. Higher residualized scores at Recovery indicate less recovery from the stressor. CESD = Center for Epidemiological Studies-Depression Scale; RRS = Ruminative Responses Scale; SRQ = State Rumination Questionnaire
p < .01,
p < .001
State Rumination and Attentional Biases
Data preparation
To test our hypothesis that the relation between rumination and attentional biases would differ based on participants’ depressive symptoms, the CESD was used to divide participants into low versus high dysphoria groups using a median split. The median of the CESD in this sample was 13 (M = 14.10, SD = 6.99), which is similar to median splits used in other studies (e.g., Joormann, 2004). This yielded 39 participants in the low dysphoria group and 44 in the high dysphoria group. CESD scores in the low dysphoria group ranged from 3 to 12 (M = 8.51, SD = 2.36); CESD scores in the high dysphoria group ranged from 13 to 40 (M = 19.05, SD = 5.92). Demographic characteristics of the low and high dysphoria groups are presented in Table 3. Age did not significantly differ between groups, t(77) < 1, p > .05. The groups did not significantly differ in gender composition, χ2(1) = 2.68, p > .05, or proportion Caucasian, χ2(1) < 1, p > .05. Although the groups did not significantly differ in their scores on the SRQ, t(81) = 1.34, p > .05, the low dysphoria group had significantly lower scores on the RRS than the high dysphoria group, t(81) = 4.45, p < .001.
Table 3.
Participant Characteristics
| Variable | Low Dysphoria (n = 39) | High Dysphoria (n = 44) |
|---|---|---|
| Age (SD) | 19.49 (2.63) | 19.48 (3.42) |
| Sex (female:male) | 15:20 | 27:17 |
| % Caucasian | 51.28 | 43.18 |
| SRQ (SD) | 16.51 (5.44) | 18.09 (5.29) |
| RRS (SD) | 31.82 (11.33) | 43.75 (13.11) |
Note. SRQ = State Rumination Questionnaire; RRS = Ruminative Responses Scale of the Response Style Questionnaire
Next, two attentional bias scores were calculated: attentional engagement and attentional disengagement. When calculating attentional bias scores, only response latencies from correct responses were examined, and RTs < 200 ms and RTs > 750 ms were considered outliers. This is in line with analytic approaches typically used with the ECT (e.g., Koster et al., 2005). Reaction times are presented in Table 4. Separate indices were calculated for attentional engagement and disengagement using the following formulas (cf. Koster et al., 2005):
Table 4.
Exogenous Cuing Task Reaction Times
| Variable | Low Dysphoria (n = 39) | High Dysphoria (n = 44) |
|---|---|---|
| Valid | ||
| Angry | 593.14 (41.17) | 569.88 (51.64) |
| Happy | 590.70 (36.88) | 576.49 (49.81) |
| Sad | 586.93 (41.80) | 575.17 (56.48) |
| Neutral | 593.25 (35.66) | 572.26 (53.31) |
| Invalid | ||
| Angry | 592.79 (37.04) | 579.67 (46.26) |
| Happy | 595.25 (39.08) | 586.64 (48.00) |
| Sad | 594.72 (45.33) | 577.42 (51.36) |
| Neutral | 599.71 (36.13) | 577.47 (50.04) |
Positive attentional engagement scores indicate that participants were faster to attend to the emotional versus neutral expressions. Positive scores on difficulties in attentional disengagement indicate that participants were slower to disengage from emotional versus neutral expressions.
Data analysis
To examine the relation between rumination and attentional biases in the high and low dysphoria groups, bivariate correlations were calculated between state rumination and attentional bias scores, controlling for trait rumination. These correlations are presented in Table 5. There were no significant correlations between state rumination and attentional scores in the low dysphoria group, all ps > .05. In the high dysphoria group, there were no significant correlations between state rumination and attentional engagement; however, there was a significant positive correlation between state rumination and difficulty disengaging from angry and sad expressions, ps < .05. There was also a positive correlation between state rumination and difficulty disengaging from happy expressions at the trend level, p = .06. Thus, within the high dysphoria group, even after controlling for RRS scores, individuals who had more difficulty disengaging from emotional expressions – particularly negative expressions – reported greater rumination in response to the stressor3. To understand the amount of state rumination that was explained by trait rumination and difficulty disengaging from negative expressions in the high dysphoria group, a hierarchical linear regression was run. RRS scores were entered in Step 1 and difficulty disengaging attention from negative expressions was entered in Step 2 predicting SRQ. RRS scores did not explain a significant proportion of variance in SRQ scores, F(1, 42) = 1.42, p > .05. However, difficulty disengaging from negative expressions explained 13% of the variance in SRQ scores, Fchange(1, 41) = 6.24, p < .02. In total, the model predicted 16% of the variance in SRQ scores, F(2, 41) = 3. 92, p < .05.
Table 5.
Correlation Between SRQ and Attention Scores in the CTL and DYS Groups, Controlling for RRS Scores
| Engagement | Disengagement | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| Angry | Happy | Sad | Angry | Happy | Sad | |
| Low Dysphoria | ||||||
| SRQ | −.08 | .19 | −.24 | .02 | .09 | .09 |
| High Dysphoria | ||||||
| SRQ | .15 | .03 | .13 | 0.30** | 0.29* | 0.33** |
Note. SRQ = State Rumination Questionnaire
p < .05,
p = .06
Discussion
Despite substantial research on rumination, few studies assess individual differences in the extent to which people are ruminating in response to an acute stressor (i.e., state rumination). Thus, the current study had two primary goals. We first investigated whether state rumination was uniquely related to prolonged sadness in response to an acute psychosocial stressor, controlling for trait rumination. Next, we examined cognitive processes that might underlie elevated state rumination in dysphoria. Given previous work on attention biases in depression (e.g., Joormann & Gotlib, 2006), we were particularly interested in focusing on attentional disengagement. Our results demonstrated the importance of state rumination by showing that state rumination was associated with less recovery from stress even after controlling for individual differences in depressive symptoms and trait rumination. In addition, state rumination in the high dysphoria group was correlated with difficulty disengaging attention from negative stimuli. In fact, in the high dysphoria group, difficulty disengaging attention from negative stimuli predicted 13% of the variance in state rumination.
Past research on rumination and recovery from stress has focused on people’s general tendency to ruminate when distressed (i.e., trait rumination), which is often used as a marker of the amount they are actually ruminating in response to a stressor. Although studies suggest that trait rumination prolongs people’s response to stress (e.g., Nolen-Hoeksema & Morrow, 1991), evidence from the current study suggests that we can improve upon our understanding of psychological recovery from a specific stressor by assessing state rumination. When trait rumination, state rumination, and depressive symptoms were all entered in the model, only state rumination explained a significant proportion of variance in the high dysphoria group’s recovery from stress. Previous studies also have documented the importance of assessing state rumination. For example, studies have found that state rumination predicted variance in people’s daily ratings of negative affect independent of trait rumination scores (e.g., Moberly & Watkins, 2008). Additionally, state rumination influenced the association between trait rumination and physiological recovery from stress (Key, Campbell, Bacon, & Gerin, 2008; Zoccola, Quas, & Yim, 2010) as well as the relation between trait rumination and anger following provocation (e.g., Denson, Pedersen, Friese, Hahm, & Roberts, 2011). Thus, growing evidence suggests that it is important to assess the amount that people are currently ruminating in response to stress when examining the relation between rumination and stress recovery.
The current study also examined possible mechanisms that may underlie state rumination. Results indicated that state rumination was not associated with individual differences in trait rumination. The lack of association between state and trait rumination further emphasizes the importance of assessing state rumination as there is not necessarily a direct correspondence between an individual’s tendency to ruminate and the amount they are ruminating in response to a specific stressor. Similar findings have been demonstrated by Puterman and colleagues (Puterman, Delongis, & Pomaki, 2010). They examined the association between state and trait rumination and found the relation between trait and state rumination was attenuated in people with higher social support. Results suggest that there are mechanisms other than trait rumination that affect the amount someone is ruminating at any given moment.
In the current study, more difficulty disengaging from sad and angry expressions was significantly associated with higher state rumination in the high dysphoria group. It is important to acknowledge, however, that dysphoric group did not significantly moderate the association between attentional bias scores and state rumination. These results, therefore, must be interpreted with caution and additional research is needed with a larger sample size to ensure sufficient power to detect higher order interactions. With this limitation in mind, the current study offers tentative evidence that the association between cognitive biases and rumination might hold true specifically within a dysphoric or depressed population. This possibility is in line with suggestions that dysphoric individuals who have difficulty disengaging attention from emotional material might also have difficulty disengaging their thoughts from a recent stressor, resulting in higher state rumination (e.g., Joormann & D’Avanzato, 2010; Koster et al., 2011). As expected, the association between state rumination and attentional biases was found in the high dysphoria and not the low dysphoria group. Other studies have also found that associations between cognitive biases and rumination were specific to the dysphoric or depressed group (e.g., Donaldson et al., 2007; Joormann & Gotlib, 2010; Phillipot & Brutoux, 2008). One reason that we might have found significant correlations in only the high dysphoria group is that the maladaptive effects of rumination require a combination of depressed mood and ruminative thought (e.g., Smallwood et al., 2003). In the current study, participants completed the exogenous cuing task (ECT) prior to the stress induction. Thus, whereas the high dysphoria group was in a negative mood state during both the ECT and stress recovery period, the low dysphoria group was in a neutral mood state during the ECT. In line with this possibility, Phillipot and Brutoux randomly assigned dysphoric and nondysphoric students to ruminate or distract and measured the subsequent impact on executive functioning. Importantly, no mood induction was used. Results indicated that the rumination induction decreased inhibition capabilities in only the dysphoric group, the group that had a combination of both rumination and sad mood.
It also is interesting to note that state rumination was associated with difficulty disengaging from not only negative emotions but also positive emotions at the trend level. Past research has reported similar across-valence effects in the association between cognitive processes and rumination – albeit trait rumination – within a dysphoric sample (e.g., De Lissnyder et al., 2012). Moreover, other studies have shown that trait rumination is linked with difficulty inhibiting neutral or non-emotional material (e.g., De Lissnyder, Derakshan, De Raedt, & Koster, 2011). It is therefore possible that the association between rumination and cognitive control deficits may not be specific to negative material but instead may be found across the board. In line with this possibility, the response styles theory emphasizes that although ruminative thought in depression and dysphoria is frequently negative in content, rumination is defined as a cognitive style involving repetitive and passive thought rather than the valence of one’s thought (e.g., Nolen-Hoeksema et al., 2008). It is therefore possible that when positive information enters working memory, such as during the ECT, ruminative thought processes make it difficult to disengage from positive stimuli as well. Future research is needed to replicate these unexpected and only marginally significant findings. In doing so, studies might consider using paradigms that measure attentional processes by means other than reaction times, such as eye tracking.
Several limitations in the current study should be noted. First, this study examined the correlation between rumination and attentional disengagement, and as such we are unable to draw conclusions about the causal relation between them. Although this study provides an important first step in understanding the relation between these two variables, additional research is needed that manipulates attentional disengagement to draw firm conclusions about causation. Second, it is important to acknowledge that the SRQ has not yet been psychometrically evaluated. Further research is needed that examines its psychometric properties. Furthermore, one should note that some items on the SRQ might be confounded with participants’ self-reported sadness ratings (see similar concerns regarding the RRS and depressive symptoms; Conway, Csank, Holm, & Blake, 2000; Segerstrom, Tsao, Alden and Craske, 2000). Researchers must, therefore, continue to work toward developing a measure of depressive rumination that does not overlap with items assessing depressive mood state. In addition, this study focused on a nonclinical sample. A replication with a clinical sample is warranted. Future research might also consider including biological markers of stress such as cortisol, heart rate, or respiratory sinus arrhythmia.
Despite these limitations, the current study has important implications. For one, future research should not rely solely on measures of trait rumination but should also assess the amount individuals are ruminating in response to a specific stressor. Assessing state rumination has the potential to improve our understanding of psychological recovery from stress. In addition, results suggest that there are variables other than the general tendency to ruminate that influences rumination in response to a specific stressor. This possibility suggests that there could be mechanisms that we can target for intervention. Indeed, attention training studies have demonstrated the ability to train participants to attend away from negative or toward positive material, which has been found to improve people’s response to stressful events (e.g., Baert, De Raedt, Schacht, & Koster, 2010; Dandeneau, Baldwin, Baccus, Sakellaropoulo, & Pruessner, 2007; Wells & Beevers, 2010). Future research might examine whether such attention training also serves to reduce state rumination, especially among individuals with heightened risk for depression.
Acknowledgments
This research was supported in part by a grant from the National Institute of Mental Health (F31MH086246) awarded to Joelle LeMoult and the 2011 James W. McLamore Provost Research Award in Social Sciences awarded to Jutta Joormann.
Footnotes
Four participants (in the low dysphoria group) elected to not provide their sex. Four participants (2 low dysphoria, 2 high dysphoria) elected to not provide their age.
Two participants did not provide the first anxiety rating, and one participant did not provide any anxiety ratings.
Regressions examining whether dysphoric group moderated the association between attentional bias and SRQ scores were not significant, Δ R2 < 3.00, ps > .05.
References
- Baert S, De Raedt R, Schact R, Koster EHW. Attentional bias training in depression: Therapeutic effects depend on depression severity. Journal of Behavior Therapy and Experimental Psychiatry. 2010;41:265–274. doi: 10.1016/j.jbtep.2010.02.004. http://dx.doi.org/10.1016/j.jbtep.2010.02.004. [DOI] [PubMed] [Google Scholar]
- Brown GW, Harris TO. Stressor, vulnerability and depression: A question of replication. Psychological Medicine. 1986;16(4):739–744. doi: 10.1017/s0033291700011740. http://dx.doi.org/10.1017/S0033291700011740. [DOI] [PubMed] [Google Scholar]
- Bushman BJ, Bonacci AM, Pedersen WC, Vasquez EA, Miller N. Chewing on it can chew you up: Effects of rumination on triggered displaced aggression. Journal of Personality and Social Psychology. 2005;88:969–983. doi: 10.1037/0022-3514.88.6.969. http://dx.doi.org/10.1037/0022-3514.88.6.969. [DOI] [PubMed] [Google Scholar]
- Cohen J, Cohen P, West SG, Aiken LS. Applied multiple regression/correlation analysis for the behavioral sciences. Erlbaum; Hillsdale, NJ: 1983. [Google Scholar]
- Conway M, Csank PAR, Holm SL, Blake CK. On assessing individual differences in rumination on sadness. Journal of Personality Assessment. 2000;75:404–425. doi: 10.1207/S15327752JPA7503_04. http://dx.doi.org/10.1207/S15327752JPA7503_04. [DOI] [PubMed] [Google Scholar]
- Dandeneau SD, Baldwin MW, Baccus JR, Sakellaropoulo M, Pruessner JC. Cutting stress off at the pass: Reducing vigilance and responsiveness to social threat by manipulating attention. Journal of Personality and Social Psychology. 2007;93:651–666. doi: 10.1037/0022-3514.93.4.651. http://dx.doi.org/10.1037/0022-3514.93.4.651. [DOI] [PubMed] [Google Scholar]
- De Lissnyder E, Derakshan N, De Raedt R, Koster EHW. Depressive symptoms and cognitive control in a mixed antisaccade task: Specific effects of depressive rumination. Cognition & Emotion. 2011;25:886–897. doi: 10.1080/02699931.2010.514711. http://dx.doi.org/10.1080/02699931.2010.514711. [DOI] [PubMed] [Google Scholar]
- De Lissnyder E, Koster EHW, Goubert L, Onraedt T, Vanderhasselt MA, De Raedt R. Cognitive control moderates the association between stress and rumination. Journal of Behavior Therapy and Experimental Psychiatry. 2012;43:519–525. doi: 10.1016/j.jbtep.2011.07.004. http://dx.doi.org/10.1016/j.jbtep.2011.07.004. [DOI] [PubMed] [Google Scholar]
- Denson TF, Pedersen WC, Friese M, Hahm A, Roberts L. Understanding impulsive aggression: Angry rumination and reduced self-control capacity are mechanisms underlying the provocation-aggression relationship. Personality and Social Psychology Bulletin. 2011;37:850–862. doi: 10.1177/0146167211401420. http://dx.doi.org/10.1177/0146167211401420. [DOI] [PubMed] [Google Scholar]
- De Raedt R, Koster EHW. Understanding vulnerability for depression from a cognitive neuroscience perspective: A reappraisal of attentional factors and a new conceptual framework. Cognitive, Affective, & Behavioral Neuroscience. 2010;10:50–70. doi: 10.3758/CABN.10.1.50. http://dx.doi.org/10.3758/CABN.10.1.50. [DOI] [PubMed] [Google Scholar]
- Dickerson SS, Kemeny ME. Acute stressors and cortisol responses: A theoretical integration and synthesis of laboratory research. Psychological Bulletin. 2004;130:355–391. doi: 10.1037/0033-2909.130.3.355. http://dx.doi.org/10.1037/0033-2909.130.3.355. [DOI] [PubMed] [Google Scholar]
- Donaldson C, Lam D, Mathews A. Rumination and attention in major depression. Behaviour Research and Therapy. 2007;45:2664–2678. doi: 10.1016/j.brat.2007.07.002. http://dx.doi.org/10.1016/j.brat.2007.07.002. [DOI] [PubMed] [Google Scholar]
- Gotlib IH, Krasnoperova E, Yue DN, Joormann J. Attentional bias for negative interpersonal stimuli in clinical depression. Journal of Abnormal Psychology. 2004;113:127–133. doi: 10.1037/0021-843X.113.1.121. http://dx.doi.org/10.1037/0021-843X.113.1.121. [DOI] [PubMed] [Google Scholar]
- Hammen C. Stress and Depression. Annual Review of Clinical Psychology. 2005;1:293–319. doi: 10.1146/annurev.clinpsy.1.102803.143938. http://dx.doi.org/10.1146/annurev.clinpsy.1.102803.143938. [DOI] [PubMed] [Google Scholar]
- Joormann J. Attention bias in dysphoria: The role of inhibitory processes. Cognition and Emotion. 2004;18:125–147. http://dx.doi.org/10.1080/02699930244000480. [Google Scholar]
- Joormann J, D’Avanzato C. Emotion regulation in depression: Examining the role of cognitive processes. Cognition and Emotion. 2010;24:913–939. http://dx.doi.org/10.1080/02699931003784939. [Google Scholar]
- Joormann J, Gotlib IH. Is this happiness I see? Biases in the identification of emotional facial expressions in depression and social phobia. Journal of Abnormal Psychology. 2006;115:705–714. doi: 10.1037/0021-843X.115.4.705. http://dx.doi.org/10.1037/0021-843X.115.4.705. [DOI] [PubMed] [Google Scholar]
- Joormann J, Gotlib IH. Emotion regulation in depression: Relation to cognitive inhibition. Cognition and Emotion. 2010;24(2):281–298. doi: 10.1080/02699930903407948. http://dx.doi.org/10.1080/02699930903407948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasch KL, Klein DN, Lara ME. A construct validation study of the Response Styles Questionnaire rumination scale in participants with a recent-onset major depressive disorder. Psychological Assessment. 2001;13:375–383. doi: 10.1037//1040-3590.13.3.375. http://dx.doi.org/10.1037/1040-3590.13.3.375. [DOI] [PubMed] [Google Scholar]
- Key BL, Campbell TS, Bacon SL, Gerin W. The influence of trait and state rumination on cardiovascular recovery from a negative emotional stressor. Journal of Behavioral Medicine. 2008;31:237–248. doi: 10.1007/s10865-008-9152-9. http://dx.doi.org/10.1007/s10865-008-9152-9. [DOI] [PubMed] [Google Scholar]
- Kirschbaum C, Pirke KM, Hellhammer DH. The ‘Trier Social Stress Test’- a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology. 1993;28:76–81. doi: 10.1159/000119004. http://dx.doi.org/10.1159/000119004. [DOI] [PubMed] [Google Scholar]
- Koster EHW, De Lissnyder E, Derakhshan N, De Raedt R. Understanding depressive rumination from a cognitive science perspective: The impaired disengagement hypothesis. Clincial Psychology Review. 2011;31:138–145. doi: 10.1016/j.cpr.2010.08.005. http://dx.doi.org/10.1016/j.cpr.2010.08.005. [DOI] [PubMed] [Google Scholar]
- Koster EHW, De Raedt R, Goeleven E, Franck E, Crombez G. Dysphoria impairs attentional disengagement from negative information. Emotion. 2005;5:446–455. doi: 10.1037/1528-3542.5.4.446. http://dx.doi.org/10.1037/1528-3542.5.4.446. [DOI] [PubMed] [Google Scholar]
- Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York: Springer; 1984. [Google Scholar]
- MacLeod C, Rutherford E, Campbell L, Ebsworthy G, Holker L. Selective attention and emotional vulnerability: Assessing the causal basis of their association through the experimental manipulation of attentional bias. Journal of Abnormal Psychology. 2002;111:107–123. http://dx.doi.org/10.1037/0021-843X.111.1.107. [PubMed] [Google Scholar]
- Moberly NJ, Watkins ER. Ruminative self-focus and negative affect: An experience sampling study. Journal of Abnormal Psychology. 2008;117:314–323. doi: 10.1037/0021-843X.117.2.314. http://dx.doi.org/10.1037/0021-843X.117.2.314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mogg K, Bradley BP. Attentional bias in generalized anxiety disorder versus depressive disorder. Cognitive Therapy and Research. 2005;29:29–45. http://dx.doi.org/10.1007/s10608-005-1646-y. [Google Scholar]
- Moons WG, Eisenberger NI, Taylor SE. Anger and fear responses to stress have different biological profiles. Brain, Behavior, and Immunity. 2010;24(2):215–219. doi: 10.1016/j.bbi.2009.08.009. http://dx.doi.org/10.1016/j.bbi.2009.08.009. [DOI] [PubMed] [Google Scholar]
- Monroe SM, Hadjiyannakis K. The social environment and depression: Focusing on severe life stress. In: Gotlib IH, Hammen CL, editors. Handbook of depression. New York: Guilford; 2002. pp. 314–340. [Google Scholar]
- Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research implications for the depressive disorders. Psychological Bulletin. 1991;110:406–425. doi: 10.1037/0033-2909.110.3.406. http://dx.doi.org/10.1037/0033-2909.110.3.406. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S. The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. Journal of Abnormal Psychology. 2000;109:504–511. http://dx.doi.org/10.1037/0021-843X.109.3.504. [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Larson J, Grayson C. Explaining the gender difference in depressive symptoms. Journal of Personality and Social Psychology. 1999;77:1061–1072. doi: 10.1037//0022-3514.77.5.1061. http://dx.doi.org/10.1037/0022-3514.77.5.1061. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Morrow J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology. 1991;61:115–121. doi: 10.1037//0022-3514.61.1.115. http://dx.doi.org/10.1037/0022-3514.61.1.115. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Morrow J. Effects of rumination and distraction on naturally occurring depressed mood. Cognition and Emotion. 1993;7:561–570. http://dx.doi.org/10.1080/02699939308409206. [Google Scholar]
- Nolen-Hoeksema S, Parker LE, Larson J. Ruminative coping with depressed mood following loss. Journal of Personality and Social Psychology. 1994;67:92–104. doi: 10.1037//0022-3514.67.1.92. http://dx.doi.org/10.1037/0022-3514.67.1.92. [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Wisco BE, Lyubomirsky S. Rethinking rumination. Perspectives on Psychological Science. 2008;3:400–424. doi: 10.1111/j.1745-6924.2008.00088.x. http://dx.doi.org/10.1111/j.1745-6924.2008.00088.x. [DOI] [PubMed] [Google Scholar]
- Phillipot P, Brutoux F. Induced rumination dampens executive processes in dysphoric young adults. Journal of Behavior Therapy and Experimental Psychiatry. 2008;39:219–227. doi: 10.1016/j.jbtep.2007.07.001. http://dx.doi.org/10.1016/j.jbtep.2007.07.001. [DOI] [PubMed] [Google Scholar]
- Posner MI. Orientation of attention. Quarterly Journal of Experimental Psychology. 1980;32:3–25. doi: 10.1080/00335558008248231. http://dx.doi.org/10.1080/00335558008248231. [DOI] [PubMed] [Google Scholar]
- Puterman E, Delongis A, Pomaki G. Protecting us from ourselves: Social support as a buffer of trait and state rumination. Journal of Social and Clinical Psychology. 2010;29:797–820. http://dx.doi.org/10.1521/jscp.2010.29.7.797. [Google Scholar]
- Radloff LS. The CESD scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. http://dx.doi.org/10.1177/014662167700100306. [Google Scholar]
- Salemink E, van den Hout M, Kindt M. Effects of positive interpretive bias modification in highly anxious individuals. Journal of Anxiety Disorders. 2009;23:676–683. doi: 10.1016/j.janxdis.2009.02.006. http://dx.doi.org/10.1016/j.janxdis.2009.02.006. [DOI] [PubMed] [Google Scholar]
- Segal ZV, Kennedy S, Gemar M, Hood K, Pedersen R, Buis T. Cognitive reactivity to sad mood provocation and the prediction of depressive relapse. Archives of General Psychiatry. 2006;63:749–755. doi: 10.1001/archpsyc.63.7.749. http://dx.doi.org/10.1001/archpsyc.63.7.749. [DOI] [PubMed] [Google Scholar]
- Segerstrom SC, Tsao JCI, Alden LE, Craske MG. Worry and rumination: Repetitive thought as a concomitant and predictor of negative mood. Cognitive Therapy and Research. 2000;24:671–688. http://dx.doi.org/10.1023/A:1005587311498. [Google Scholar]
- Smallwood J, Obsonsawin M, Baracaia SF, Reid H, O’Connor R, Heim D. THE relationship between rumination, dysphoria, and self-referent thinking: Some preliminary findings. Imagination, Cognition and Personality. 2003;22:317–342. http://dx.doi.org/10.2190/2N80-AVM3-4A23-LEAJ. [Google Scholar]
- Stone AA, Schwarz JE, Neale JM, Shiffman S, Marco CA, Hickcox M, Cruise Laura J. A comparison of coping assessed by ecological momentary assessment and retrospective recall. Journal of Personality and Social Psychology. 1998;74:1670–1680. doi: 10.1037/0022-3514.74.6.1670. http://dx.doi.org/10.1037/0022-3514.74.6.1670. [DOI] [PubMed] [Google Scholar]
- Teasdale JD. Cognitive vulnerability to persistent depression. Cognition and Emotion. 1988;2:247–274. http://dx.doi.org/10.1080/02699938808410927. [Google Scholar]
- Wells TT, Beevers CG. Biased attention and dysphoria: Manipulating selective attention reduces subsequent depressive symptoms. Cognition and Emotion. 2010;24:719–728. http://dx.doi.org/10.1080/02699930802652388. [Google Scholar]
- Zoccola PM, Quas JA, Yim IS. Salivary cortisol responses to a psychosocial laboratory stressor and later verbal recall of the stressor: The role of trait and state rumination. Stress. 2010;13:435–443. doi: 10.3109/10253891003713765. http://dx.doi.org/10.3109/10253891003713765. [DOI] [PubMed] [Google Scholar]