

Abstract
Traffic congestion increases vehicle emissions and degrades ambient air quality, and recent studies have shown excess morbidity and mortality for drivers, commuters and individuals living near major roadways. Presently, our understanding of the air pollution impacts from congestion on roads is very limited. This study demonstrates an approach to characterize risks of traffic for on- and near-road populations. Simulation modeling was used to estimate on- and near-road NO2 concentrations and health risks for freeway and arterial scenarios attributable to traffic for different traffic volumes during rush hour periods. The modeling used emission factors from two different models (Comprehensive Modal Emissions Model and Motor Vehicle Emissions Factor Model version 6.2), an empirical traffic speed–volume relationship, the California Line Source Dispersion Model, an empirical NO2–NOx relationship, estimated travel time changes during congestion, and concentration–response relationships from the literature, which give emergency doctor visits, hospital admissions and mortality attributed to NO2 exposure. An incremental analysis, which expresses the change in health risks for small increases in traffic volume, showed non-linear effects. For a freeway, “U” shaped trends of incremental risks were predicted for on-road populations, and incremental risks are flat at low traffic volumes for near-road populations. For an arterial road, incremental risks increased sharply for both on- and near-road populations as traffic increased. These patterns result from changes in emission factors, the NO2–NOx relationship, the travel delay for the on-road population, and the extended duration of rush hour for the near-road population. This study suggests that health risks from congestion are potentially significant, and that additional traffic can significantly increase risks, depending on the type of road and other factors. Further, evaluations of risk associated with congestion must consider travel time, the duration of rush-hour, congestion-specific emission estimates, and uncertainties.
Keywords: Congestion, Morbidity, Mortality, NO2, Risk assessment, Traffic-related air pollution
1. Introduction
Traffic on roads has significantly increased in the U.S. and elsewhere over the past 20 years (Schrank and Lomax, 2007). In many areas, vehicle emissions have become the dominant source of air pollutants, including carbon monoxide (CO), carbon dioxide (CO2), volatile organic compounds (VOCs) or hydrocarbons (HCs), nitrogen oxides (NOx), and particulate matter (PM) (Transportation Research Board (TRB), 2002). The increasing severity and duration of traffic congestion have the potential to greatly increase pollutant emissions and to degrade air quality, particularly near large roadways. These emissions contribute to risks of morbidity and mortality for drivers, commuters and individuals living near roadways, as shown by epidemiological studies, evaluations of proposed vehicle emission standards, and environmental impact assessments for specific road projects (World Health Organization (WHO), 2005; Health Effects Institute (HEI), 2010).
It is useful to separate traffic-associated pollutant impacts and risks into two categories. First, “congestion-free” impacts refer to impacts of traffic at volumes below the level that produces significant congestion. In this case, each additional vehicle added to the road does not substantially alter traffic patterns, e.g., the speed and travel time of other vehicles are unaffected, and thus vehicle emission factors do not depend on traffic volume. As a result, the marginal impact of an additional vehicle is equal to the average impact of the vehicle fleet. This is not necessarily true during congestion, the second category considered. While there are many definitions, congestion is often defined as periods when traffic volume exceeds road capacity. (Other definitions use a speed threshold, a percentage of free-flow speed of a roadway, or other indicator.) The present study focuses on what might be called “recurring congestion,” specifically, congestion caused by high traffic volumes during weekday peak “rush hour” periods. However, traffic volume is treated as a continuous variable, and strict definitions of congestion are not needed.
In the present analysis, “congestion-related” impacts incorporate multiple interactions that occur with congestion. First, congestion lowers the average speed, which increases travel time and exposure on a per vehicle basis. This effect can be considerable, e.g., the average annual travel delay for a traveler making rush hour trips in the U.S. was 38 h in 2005, based on 437 urban areas (Schrank and Lomax, 2007). Second, congestion diminishes dispersion of vehicle-related pollutants since vehicle-induced turbulence depends on vehicle speed (Benson, 1989). Thus, lower vehicle speeds can increase pollutant concentrations from roadway sources. Third, congestion can change driving patterns, resulting in an increased number of speedups, slowdowns, stops and starts, which increase emissions compared to “cruise” conditions, especially with high power acceleration. For example, Sjodin et al. (1998) showed up to 4-, 3- and 2-fold increases in CO, HC and NOx emissions, respectively, with congestion (average speed of 13 miles per hour, mph; 1 mph=1.61 km per hour) compared to uncongested conditions (average speed, 38–44 mph). Thus, it is important to separate congestion-free and congestion-related impacts since emissions, impacts and risks can differ greatly, and because such analyses can better inform decisions related to traffic and air quality management, as well as impact and risk assessments.
Few evaluations of congestion-related impacts have been undertaken, and available studies have essentially combined congestion and non-congestion related impacts. Tonne et al. (2008) predicted that the congestion charging zone in London, where drivers must pay fees when their vehicles enter this area, would gain 183 years-of-life per 100,000 population in the congestion charging zone itself and a total of 1,888 years-of-life in the greater London area. Eliasson et al. (2009) estimated that a similar zone in Stockholm would avoid 20–25 deaths annually due to traffic-related air pollution in the inner city, and 25–30 deaths annually in the metropolitan area, which contains 1.4 million inhabitants. Both studies indicate that congestion pricing is beneficial in reducing traffic-related health impacts, but congestion-free and congestion-related impacts were not separated. These European studies focused on congestion charging zones, which are uncommon in the U.S., and the vehicle mix and fleet emission characteristics may differ substantially from those in the U.S. Using a different approach that examined shifts in time activity patterns (TAPs: the amount of time spent at various locations and related activities) due to travel delays along with literature values of exposure concentrations in relevant microenvironments, we estimated that a 30 min day−1 travel delay accounted for 21±12% of the exposure to benzene and 14±8% of PM2.5 for a typical working adult on weekdays (Zhang and Batterman, 2009). Levy et al. (2010) estimated that the estimated public health cost of mortality attributable to congestion in 83 U.S. cities in 2000 was $31 billion (2007 dollars). This study used a macro-level approach to estimate traffic volume, which was then linked to the Motor Vehicle Emissions Factor Model 6.2 (MOBILE6.2) (EPA, 2003), thus providing a snapshot of congestion. However, congestion is dynamic and varies with time, space, weather and other factors (Downs, 2004). Overall, these studies suggest that congestion represents a substantial share of exposure to drivers and commuters, with potentially significant risks and impacts on health.
This study investigates the magnitude of air pollution impacts and health risks to on- and near-road populations that might occur due to recurring congestion, such as Monday through Friday rush hour traffic. Recurring congestion can result in repeated and chronic exposures, and an increase in long term health risks. “Incident congestion,” such as that caused by an accident or disabled vehicle, is not addressed, although such events may also be important for certain acute health outcomes, e.g., asthma exacerbation. This study utilizes predictive risk assessment techniques, namely, simulation models for traffic, emissions, pollutant dispersion and risk, and an incremental analysis that evaluates congestion-free and congestion-related impacts. After describing the approach, two case studies are used to analyze air pollution impacts and risks. A limited sensitivity analysis is conducted to examine impacts of key parameters on the estimated incremental risk. The merits of the various approaches that might be used to estimate congestion impacts conclude the analysis.
2. Methods
2.1. Approach
Risk assessment methods, depicted in Fig. 1, are used to estimate health risks due to traffic for two scenarios. In brief, vehicle emissions are used as an input to a dispersion model to estimate concentrations, which are then multiplied by exposure time and a risk factor representing the concentration–response relationship. While some exposure and risk assessments utilize time activity patterns (TAPs) or human activity patterns, for simplicity we consider only exposure durations in traffic micro-environments, which include the delays due to traffic congestion. An incremental analysis is used to estimate the marginal impacts of increases in traffic volume. Such analyses are widely used in economic models to examine effects of small changes of an input on outcomes of interest; they also represent one of the classical “sensitivity analysis” techniques used to identify key variables in modeling systems (Trueman, 2007). One difference here, however, is that a wide range of traffic flows is examined over which relationships are expected to vary considerably.
Fig. 1.
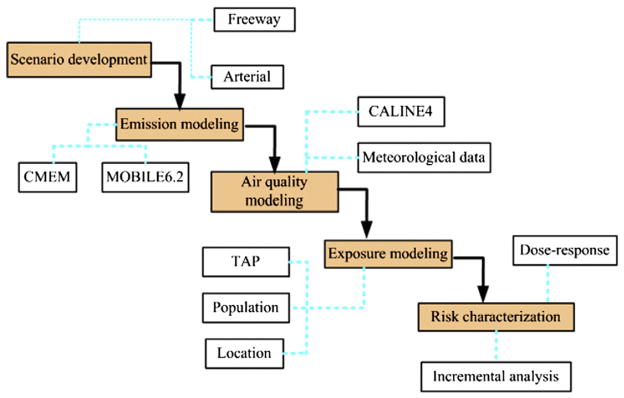
Diagram for modeling health risks due to traffic and congestion (CALINE4, the California Line Source Dispersion Model version 4 CMEM, the Comprehensive Modal Emissions Model; MOBILE6.2, the Motor Vehicle Emissions Factor Model version 6.2; TAP, time activity pattern).
2.2. Case studies
Two case studies or scenarios were developed to examine associations between traffic volume, exposures and health risks. The first, a freeway scenario, models an 8 km long segment of interstate I-94 in Ann Arbor, MI (Fig. S1), which was selected for a field study in which instantaneous emission rates were modeled. This segment had a permanent traffic recorder (PTR) operated by the Michigan Department of Transportation (MDOT). The portion of the segment west of US-23 had two lanes in each direction; the segment to the east had three lanes in each direction. The annual average daily traffic (AADT) volumes for these segments were 78,300 and 91,300 vehicles day−1 in west and east directions, respectively (MDOT, 2008). During the field study described in Zhang et al. (2011), traffic volumes were 3099 and 4040 vehicles per hour (vph) in morning and afternoon rush hour periods, respectively. The vehicle mix (8% heavy duty trucks and 92% light duty vehicles) during rush hour was based on PTR records from October, 2007 (Southeast Michigan Council of Governments (SEMCOG), 2006), and was assumed to be constant. The southeast Michigan vehicle age distribution was assumed to represent the fleet. The traffic volume in the incremental analysis was allowed to vary from 1000 to 10,000 vph. Given that design capacity is 2000 vehicles h−1 lane−1 for a freeway (SEMCOG, 2004), the upper volume represents about 120% of road capacity. In addition to the freeway scenario with an incremental analysis, a scenario using observed volumes on I-94 during rush hour was modeled to demonstrate the spatial and temporal patterns of predicted pollutant levels.
An arterial scenario was also modeled. This used a segment along Grand River Boulevard (M-5) in Detroit, which is 8.5 km long and includes two lanes per direction and a central turning lane (Fig. S2). The AADT volumes for the segment west of M-39 and east of M-39 were 23,800 and 19,200 vehicles day−1, respectively (MDOT, 2009). The regional vehicle mix and age distribution described above were used. Traffic volumes ranged from 1000 to 4000 vph (about 120% of road capacity; design capacity is 825 vehicles h−1 lane−1 for an arterial road; SEMCOG, 2004).
Exposures of drivers and commuters were estimated using several assumptions about their behavior, traffic, and in-vehicle concentrations. A driver or commuter was assumed to travel on the segments under a constant traffic volume in both morning and afternoon rush hours every weekday throughout the year. The in-vehicle concentration was assumed to be equal to predicted on-road concentrations.
Exposures of near-road residents were derived as follows. A uniform population density along both sides of the road was assumed. The (non-commuting) residents were assumed to stay at home, which was assumed to be located 100 m from the road, during rush hour every weekday. Obviously, time activity patterns and actual distances can vary considerably, although an estimated 11% of the US households are located within 100 m of a four lane highway (Brugge et al., 2007). The average concentrations at upwind and downwind receptors (each at 100 m distance) were used, given the assumption of a uniform population density. Since indoor NO2 concentrations (in homes without indoor sources) are about 50% of outdoor concentrations (HEI, 2010), the indoor exposure concentration was assumed to be half that of predicted outdoor concentrations at the 100 m receptors.
2.3. Emission modeling
Emission factors for a vehicle fleet traveling at different speeds were estimated using the Comprehensive Modal Emissions Model (CMEM) and MOBILE6.2. In this study, emissions were estimated for NOx since traffic is its major source, and both models can predict NOx while adjusting for speed effects. There are other important traffic-related pollutants, e.g., PM2.5; however, CMEM does not estimate PM2.5, and MOBILE6.2 does not account for vehicle speed effects on PM2.5.
CMEM is a power-demand instantaneous model that can predict fuel consumption and emissions of CO, HC, NOx and CO2 on a fine time scale, e.g., a second-by-second basis (Scora and Barth, 2006; Zhang and Batterman, 2011). CMEM was used only in the freeway scenario because driving patterns were collected at this frequency only for this freeway segment. The CMEM estimates from Zhang and Batterman (2011), which were based on the east-bound I-94 segment, were assumed to apply to both directions.
MOBILE6.2 is a widely used regulatory emission model (Pierce et al., 2008) that estimates emissions of HC, CO, NOx, PM and air toxics like benzene on the basis of chassis dynamometer measurements and driving cycles designed for four road types: freeway, arterial, ramp and local road (Environmental Protection Agency (EPA), 2003; Pierce et al., 2008). Emission factors in summer and winter were estimated using MOBILE6.2 and the fleet mix, vehicle age distribution, and typical daily temperatures for different vehicle speeds. Annual average emission factors were approximated as the average of summer and winter predictions.
For both emission models, emission factors are a function of fleet speed, and speed is a function of traffic volume. Speeds corresponding to given traffic volumes were derived using the Bureau of Public Road (BPR) formula (Dowling, 1997):
| (1) |
where s=predicted mean speed; sf =free-flow speed; v= volume per hour; c=practical capacity, estimated locally as 2000 vehicles h−1 lane−1 for freeways, and 825 vehicles h−1 lane−1 for urban arterials (SEMCOG, 2004); a=scalar coefficient ranging from 0.05 to 1; and b=power coefficient ranging from 4 to 11. The latter two coefficients were obtained from a Detroit case study, which estimated a=0.1226 for the freeway, a=1.00 for the arterial, and b=4.688 (Batterman et al., 2010). The posted speed limits are 70 and 35 mph for freeway and arterial segments, respectively, in the two case studies.
2.4. Dispersion modeling
Dispersion model predictions of NOx concentrations attributable to traffic emissions were given by the California Line Source Dispersion Model version 4 (CALINE4). This model uses a Gaussian-plume model for a line source of finite length, and a mixing zone to characterize thermal and mechanical turbulence (e.g., vehicle wake effects), which is defined as the region over the roadway (traffic lanes, not shoulders) plus 3 m on each side (Benson, 1989). Both emissions and turbulence in the mixing zone are assumed to be uniformly distributed, while the decay of concentrations at more distant locations follows an empirical Gaussian line source equation (Benson, 1989). Because CALINE4 was not designed to process hourly data for a full year, a simplified modeling approach was used (Zhang and Batterman, 2010). In brief, the annual average concentration at a receptor was estimated as the sum of CALINE predictions for 16 wind sectors (each spanning 22.5°) and 15 wind speed classes (1 m s−1 for each bin, e.g., 0.5 to 1.5, 1.5 to 2.5, …), weighted by the joint probability of each wind sector/wind speed category during morning and afternoon rush hour periods, based on (hourly) meteorology from 2005. Model inputs included emission factors, traffic flows, receptor locations, and surface meteorological data for morning and afternoon rush hours (7–9 am and 4–6 pm) in 2005, measured at Detroit Metropolitan Airport (located 24 and 18 km from the freeway and arterial segments, respectively). Receptors were placed 0, 25, 50, 75, 100 and 150 m from both sides of a transect perpendicular to the center of the studied road segments.
Predicted NOx concentrations were converted into NO2 levels in order to utilize NO2-based concentration–health response relationships. Nitric oxide (NO) emissions, which usually account for 90–95% of NOx emissions in traffic (WHO, 2005), are rapidly converted into NO2 by reaction with ozone and OH− radicals. Ambient concentrations of NO and NO2 vary with distance from traffic and other factors, e.g., background ozone and NO2 concentrations, sunlight and dispersion conditions (HEI, 2010). In this study, NO2 concentrations were predicted using an empirical model recommended by the UK Department for Environment, Food and Rural Affairs (2003):
| (2) |
where NO2(road) =annual mean NO2 concentration attributable to the road; NOx(road) =annual mean NOx concentration attributable to the road; and NOx(background) =annual mean background NOx concentration. Eq. (2) gives NO2:NOx ratios from 0.25 at low NOx levels to 0.12 at high NOx concentrations. Although developed for long-term NO2:NOx ratios, Eq. (2) was assumed to hold for short term relationships. The NOx(road) concentration was taken from CALINE4 predictions, and the NOx(background) concentration was set to 28.7 μg m−3, the 2004 average background level at a Detroit area monitor (East 7 Mile, northeast Detroit) (Brown et al., 2007).
2.5. Exposure assessment
Daily and annual NO2 exposures of on-road population were calculated as follows
| (3) |
| (4) |
where Ed =adjusted daily exposures to NO2 (μg m−3 day−1); Ea = adjusted annual exposures to NO2 (μg m−3 year−1); Con–road = predicted on-road concentrations (μg m−3); T=travel time (h), calculated by dividing the segment length over vehicle speed; 1/24=daily adjusted coefficient (h−1 day−1), a reciprocal of 24 h per day, which distributes in-vehicle exposures during travel over the day in order to be compatible with daily-average-based concentration–response relationships; and 255/365=annual adjusted coefficient given 255=weekdays per year and 365=days per year, thus distributing short-term exposures over a year, again to be comparable with the concentration–response relationships.
Exposures for near-road population were derived similarly to that just described, but with the following changes. In Eqs. (3) and (4), on-road concentrations were replaced by one half of the near-road concentrations, and travel time was replaced by the rush hour duration, defined in Eq. (5):
| (5) |
where Trush–hour =actual duration of rush hour; Tfree–flow =baseline duration of free-flow conditions (0.5 h); 0.5=a scale factor, which is used to account for some of road network dynamics (e.g., vehicles enter and leave a network at anytime during a rush hour); sf =free-flow speed (70 and 35 mph for freeway and arterial road, respectively); s= speed (mph). The rush hour duration is extended due to increased traffic volume. Residents were assumed to be at home during rush hours every weekday.
2.6. Risk characterization
Health risks were calculated by linking estimated exposures to the relevant concentration–response relationships from the literature. These relationships were assumed to hold for traffic-related air pollutants as indicated by NO2, and for both congestion and congestion-free conditions, which can be justified if the pollutant mixtures associated with these conditions are similar. Health outcomes of interest and available in the literature include short term morbidity, which represents emergency doctor visits and hospital admissions (EDA), and long term mortality. Both short- and long-term endpoints were selected, based on the strongest concentrations–response relationships in the literature as given by US Environmental Projection Agency (EPA) (2008). Specifically, risks were estimated using exposures and the concentration–response intervals of 0.5–5.3% and 0–14.8% per 10 μg m−3 NO2 concentration increase for EDA and all-cause mortality, respectively. These intervals represent the ranges of the mean estimates from different studies, and not statistical confidence intervals from a meta-analysis. EPA (2008) states that confidence intervals cannot be established since the underlying studies used different models, e.g., single and multi-pollutant models, different covariates, different cohorts, some studies only consider one age group, and other differences.
The incremental risks of increases in traffic volume were derived by dividing the differences of the risks corresponding to nearby traffic volumes by the differences of these traffic volumes. They represent the change (e.g., increase) in risk for an individual per each additional vehicle at a specific traffic volume. Thus, the incremental risk is the marginal risk for an individual given changes in traffic volume. The analysis addressed risks for individuals in traffic-related microenvironments, e.g., in vehicles and near major roads. Incremental risks might also change for populations in other environments due to emissions of primary pollutants, e.g., carbon monoxide and NO2, as well as the formation of secondary pollutants, e.g., ozone promoted by NO2 emissions.
2.7. Sensitivity analysis
A limited sensitivity analysis examined impacts of key factors on predicted incremental risk, including speed, emission factors, and the NO2/NOx ratio. This analysis predicted incremental mortality risks for the on-road population during the morning rush hour using the freeway scenario under different conditions, speeds of 50, 55, 60, 65 and 70 mph with the constant emission factor (2.7 g mi−1) and NO2/NOx ratio (0.16), emission rates of 1.9, 2.1, 2.3, 2.5 and 2.7 g mi−1 at constant speed (70 mph) and NO2/NOx ratio (0.16), and NO2/NOx ratios of 0.12, 0.15, 0.18, 0.22 and 0.25 at constant emission factor (2.7 g mi−1) and speed (70 mph). Emission estimates were derived from MOBILE6.2.
3. Results
3.1. Spatial–temporal patterns of predicted NO2 levels
Fig. S3 shows how quickly predicted NO2 levels decrease with distance from the highway, consistent with previous studies (WHO, 2005). Although the afternoon rush hour traffic volume was 30% higher than that in the morning, morning and afternoon concentrations were similar, mainly due to poorer dispersion conditions in morning, specifically more frequent occurrences of low speed winds.
3.2. Air pollution impacts
Fig. 2 shows associations between traffic volume, speed and NOx emission factors for the freeway and arterial scenarios. For the freeway, speeds were constant up to volume of approximately 4400 vph, at which point speeds began to decrease. Emission factors from both CMEM and MOBILE6.2 were also constant at low volumes. At high volumes, CMEM’s predictions slightly increased while MOBILE6.2’s slightly decreased. For the arterial case, speed was constant at low traffic volumes, and dropped quickly after around 2000 vph (Fig. 2A). Emission factors were nearly constant at low volumes, and increased after 2500 vph when vehicle speeds are low (Fig. 2B).
Fig. 2.
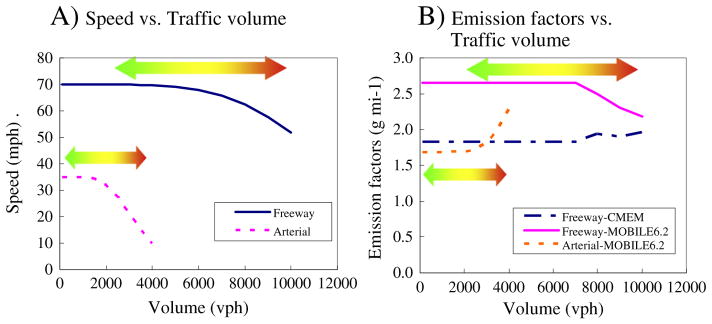
Predicted speed and NOx emission factors versus traffic volumes for the freeway and arterial scenarios (green to red denotes free flow conditions to congestion).
Figs. 3A–B show NO2 concentrations predicted for various emission estimates, traffic volume and rush hour periods in the freeway scenario. Concentrations based on CMEM estimates were nearly linearly associated with traffic volume (Figs. 3A–B); those based on MOBILE6.2 increased exponentially with traffic volume to 7000 vph, and then gradually leveled off (Fig. 3A–B). Figs. 3C–D show predicted NO2 concentrations in the arterial scenario. NO2 levels increased nearly linearly to about 3000 vph, and then increased sharply. These predictions included emissions from the road segment only, i.e., background levels of NO2 attributable to other emissions were not included.
Fig. 3.

Predicted NO2 concentrations versus traffic volume in the freeway and arterial scenarios (green to red, free flow conditions to congestion).
3.3. Health risks
Predicted short- and long-term health risks for the freeway scenario with traffic volumes from 1000 to 10,000 vph using CMEM and MOBILE6.2 emission estimates are shown in Tables 1 and 2, respectively. Predicted total health risks increased with increased traffic volume, regardless of health outcome, road type and emission models. At the same traffic volume, traffic during the morning rush hour increased risks by 20 to 40% compared to afternoon rush hour, mainly due to the poorer dispersion conditions mentioned. Differences between results in Tables 1 and 2 were mainly determined by the differences from two emission estimates and the empirical NO2–NOx relationship.
Table 1.
Predicted short- and long-term health risks for selected receptors in the freeway scenario for different traffic volumes using CMEM emission estimates (EDA, emergency doctor visit or hospital admissions; unit: probability×10−6 day−1 person−1 for EDA and probability×10−6 year−1 person−1 for mortality.).
| Volume | On-road population
|
Near-road populationa
|
||||||
|---|---|---|---|---|---|---|---|---|
| Morning rush hours
|
Afternoon rush hours
|
Morning rush hours
|
Afternoon rush hours
|
|||||
| EDAb | Mortality | EDA | Mortality | EDA | Mortality | EDA | Mortality | |
| 1000 | 6–67 | 0–130 | 5–50 | 0–98 | 10–104 | 0–203 | 7–73 | 0–142 |
| 2000 | 12–123 | 0–241 | 9–95 | 0–184 | 19–203 | 0–397 | 13–143 | 0–279 |
| 3000 | 16–174 | 0–339 | 13–135 | 0–262 | 28–299 | 0–583 | 20–211 | 0–412 |
| 4000 | 21–220 | 0–429 | 16–172 | 0–335 | 37–392 | 0–764 | 26–278 | 0–542 |
| 5000 | 25–264 | 0–515 | 20–208 | 0–405 | 46–483 | 0–942 | 32–344 | 0–672 |
| 6000 | 29–308 | 0–602 | 23–244 | 0–477 | 54–575 | 0–1121 | 39–411 | 0–803 |
| 7000 | 34–357 | 0–696 | 27–284 | 0–554 | 63–670 | 0–1307 | 45–482 | 0–940 |
| 8000 | 41–433 | 0–844 | 33–347 | 0–678 | 77–820 | 0–1599 | 56–592 | 0–1155 |
| 9000 | 47–501 | 0–977 | 38–404 | 0–788 | 88–932 | 0–1818 | 64–675 | 0–1318 |
| 10,000 | 57–609 | 0–1189 | 47–494 | 0–965 | 105–1110 | 0–2165 | 76–807 | 0–1575 |
Near-road population represents individuals living at 100 m to freeways here.
Emergency doctor visit or hospital admissions.
Table 2.
Predicted short- and long-term health risks for selected receptors in the freeway scenario using MOBILE6.2 emission estimates (unit: probability×10−6 day−1 person−1 for EDA and probability×10−6 year−1 person−1 for mortality.).
| Volume | On-road population
|
Near-road populationa
|
||||||
|---|---|---|---|---|---|---|---|---|
| Morning rush hours
|
Afternoon rush hours
|
Morning rush hours
|
Afternoon rush hours
|
|||||
| EDAb | Mortality | EDA | Mortality | EDA | Mortality | EDA | Mortality | |
| 1000 | 9–94 | 0–183 | 7–71 | 0–139 | 14–150 | 0–293 | 10–105 | 0–205 |
| 2000 | 16–170 | 0–331 | 12–131 | 0–256 | 28–292 | 0–569 | 19–206 | 0–401 |
| 3000 | 22–235 | 0–459 | 17–184 | 0–360 | 40–425 | 0–830 | 29–302 | 0–590 |
| 4000 | 28–294 | 0–574 | 22–233 | 0–455 | 52–553 | 0–1080 | 37–396 | 0–773 |
| 5000 | 33–350 | 0–682 | 26–279 | 0–545 | 64–678 | 0–1323 | 46–488 | 0–952 |
| 6000 | 38–405 | 0–790 | 31–326 | 0–635 | 76–803 | 0–1566 | 55–581 | 0–1133 |
| 7000 | 44–465 | 0–906 | 35–376 | 0–734 | 88–932 | 0–1819 | 64–677 | 0–1321 |
| 8000 | 48–513 | 0–1001 | 39–416 | 0–813 | 96–1017 | 0–1985 | 70–741 | 0–1445 |
| 9000 | 54–568 | 0–1108 | 44–462 | 0–901 | 103–1095 | 0–2136 | 75–798 | 0–1557 |
| 10,000 | 62–652 | 0–1273 | 50–532 | 0–1038 | 114–1212 | 0–2364 | 83–885 | 0–1726 |
Near-road population represents individuals living at 100 m to freeways here.
Emergency doctor visit or hospital admissions.
Table 3 shows predicted health risks for the arterial scenario. Like the freeway results, the arterial scenario had higher risks during the morning rush hour.
Table 3.
Predicted short- and long-term health risks for selected receptors in the arterial scenario using MOBILE6.2 emission estimates (unit: probability×10−6 day−1 person−1 for EDA and probability×10−6 year−1 person−1 for mortality.).
| Volume | On-road population
|
Near-road populationa
|
||||||
|---|---|---|---|---|---|---|---|---|
| Morning rush hours
|
Afternoon rush hours
|
Morning rush hours
|
Afternoon rush hours
|
|||||
| EDAb | Mortality | EDA | Mortality | EDA | Mortality | EDA | Mortality | |
| 1000 | 9–96 | 0–187 | 7–73 | 0–142 | 6–68 | 0–133 | 3–33 | 0–65 |
| 1500 | 13–143 | 0–278 | 10–109 | 0–212 | 10–102 | 0–200 | 5–51 | 0–99 |
| 2000 | 19–198 | 0–387 | 14–152 | 0–296 | 13–141 | 0–274 | 7–70 | 0–136 |
| 2500 | 27–284 | 0–554 | 21–219 | 0–427 | 18–192 | 0–374 | 9–95 | 0–186 |
| 3000 | 43–451 | 0–880 | 33–350 | 0–682 | 27–281 | 0–548 | 13–140 | 0–274 |
| 3500 | 74–787 | 0–1536 | 58–614 | 0–1198 | 42–448 | 0–874 | 21–225 | 0–439 |
| 4000 | 138–1461 | 0–2851 | 108–1148 | 0–2240 | 73–772 | 0–1507 | 37–391 | 0–763 |
Near-road population represents individuals living at 100 m to freeways here.
Emergency doctor visit or hospital admissions.
3.4. Incremental health risk analysis
Fig. 4 shows incremental risks (increased risk for an individual per an additional vehicle) for the upper bound mortality outcomes in the freeway scenario. (Figs. S4–S5 show incremental risks for EDA using CMEM and MOBILE6.2 emission estimates, which are proportional to the mortality risk.) The incremental risks for the on-road population in the morning rush hour period were 20 to 45% higher than those in the afternoon rush hour.
Fig. 4.

Predicted incremental risks per vehicle versus traffic volume for upper bound mortality in the freeway scenario (CMEM, estimated based on CMEM estimates; MOBILE6.2, estimated based on MOBILE6.2 estimates; near-road representing individuals living at 100 m to a highway; green to red, free flow conditions to congestion).
For the arterial scenario, incremental risks greatly increased at high traffic volumes (Fig. 5). (Fig. S6 shows incremental risks for EDA using MOBILE6.2 emission estimates, and again, incremental risks for EDA and mortality are proportional.) In the arterial scenario, speeds decreased substantially (from 35 to 10 mph) and emission factors increased markedly (from 1.7 to 2.3 g mi−1).
Fig. 5.
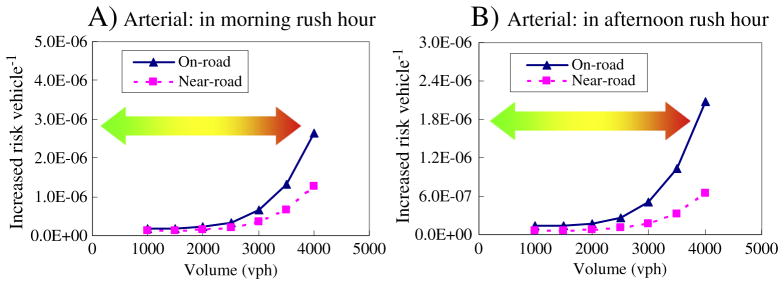
Predicted incremental risks per vehicle versus traffic volume for upper bound mortality in the arterial scenario.
3.5. Sensitivity analysis
Fig. S7 shows effects of speed, emission factors and the NO2/NOx ratio on incremental mortality risks. Generally, incremental risks decreased as speed increased (or traffic volume decreased), and risks increased with higher emission factors and higher NO2/NOx ratios. The NO2/NOx ratio had the largest impact on incremental risks; its relative sensitivity was an order of magnitude higher than that for emission factors, and two orders higher than speed’s.
4. Discussion
This study demonstrates a methodology for analyzing the health risks attributable to traffic, specifically using a marginal analysis that shows the effect of incremental increases in traffic volume. To our knowledge, this appears to be the first study examining health risks attributable to congestion-related air pollution using this approach. Although the methodology employs several models that incorporate simplifying assumptions, the incremental analysis shows the effect of each additional vehicle. It highlights the key factors affecting risks due to congestion, which include traffic volume, speed, road type, emission factor and meteorology.
The key factors determining NO2 concentration predictions include the emission model (MOBILE6.2 vs. CMEM), receptor location (on-road vs. near road), and road type (freeway vs. arterial road). In the freeway scenario, NO2 concentration trends were determined by mainly traffic volume, emission factors and the empirical NO2–NOx relationship. MOBILE6.2 has slightly lower emission factors at lower speeds (high traffic volumes), thus NO2 concentrations increase slowly at high volumes compared to a sharp increase at low volumes. Additionally, with the same traffic volume, concentrations predicted for the morning rush hour are 30 to 50% higher than those in afternoon rush hour period, which is mainly attributable to meteorological factors (more frequent lower winds and poor dispersion conditions). In the arterial road scenario, the predicted NO2 trends can be explained by emission factors that are approximately constant at low volumes and thus traffics volume dominates the trend, while at high volumes, increasing emission factors make NO2 levels rise more sharply (Fig. 2).
The predicted incremental risk per vehicle in the freeway scenario suggests a U-shape pattern for the on-road population, and constant incremental risks at low traffic volume for near-road populations. This indicates that incremental risks may be variable, dependent on driving patterns and parameters that pertain to that specific road segment and population. These patterns can be explained by travel time (for the on-road population), emission estimates, and the empirical NO2–NOx relationship. The incremental risks derived using CMEM are used to explain the interactions of these factors. The on-road risks show U-shaped curves with traffic volume, as depicted in Fig. 4A and B: from 1000 to 4000 vph, trends are determined by the NO2/NOx empirical relationship because speed and emission factors are constant, while the proportion of NO2 to NOx slightly decreases from 0.3 to 0.22 with higher volumes; from 5000 to 7000 vph, emission factors remain constant but speed decreases, resulting in longer travel times, and the NO2 to NOx ratio slightly decreases (from 0.21 to 0.19), which together slightly increase incremental risks; and lastly, for volumes exceeding 8000 vph, incremental risks increase due to longer travel delays, higher emission factors, and slightly decreased NO2/NOx ratio. The near-road risks show smaller changes, but the pattern is similar. The variation in results around 7000 to 10,000 vph, a result of step changes in the underlying models, might be addressed by smoothing.
The dramatic changes in incremental risks in the arterial scenario suggest that congestion could pose risks to commuters on and residents near arterial roads that are greater than congestion risks associated with freeways, possibly because lower speeds might be associated with more acceleration/deceleration events than higher speeds and, to a lesser degree, because low speeds reduce vehicle-induced dispersion (Benson, 1989).
In summary, the case studies indicated that incremental risks depend primarily on emission rates, empirical NO2–NOx relationships, and travel delay (for the on-road population). At the high traffic volumes often associated with congestion, emission rates dominate the factors affecting risk trends. The divergence between the two emission models further suggests the importance of the emission estimates, especially for congested conditions. Many other factors can influence risk results, as described below.
4.1. Relevance of the case studies
The case studies used two simplified and somewhat hypothetical scenarios. The volumes assumed for the study segments may be unrealistic, e.g., the observed freeway traffic volume was only 4040 vph in the afternoon rush hour, less than half of the highest volume (10,000 vph) simulated. The results of incremental risks are expected to vary with roads with different orientations, topography, meteorology, and population density. Further, only NO2 was considered. It would be helpful to examine other traffic-related pollutants, such as diesel exhaust and PM2.5, given its health significance and differences in emission trends from NOx.
4.2. Emission uncertainties
The MOBILE6.2 and CMEM models yield different trends of emission factors against traffic volume, and the former model’s predictions are systematically higher. These models have many differences. CMEM simulates segment-specific driving behaviors using segment-specific second-by-second speed/acceleration profiles, while MOBILE6.2 assumes a generic driving pattern. Differences and uncertainties also occur due to the different approaches used to represent driving patterns, smoothing of speed and acceleration data used by CMEM, vehicle fleet assumptions, and difference in driving cycles and calibration database, among other reasons (Zhang and Batterman, 2011). Smit (2006, 2008) suggests that emission models based on average speeds, such as MOBILE6.2, do not explicitly account for congestion since input parameters representing congestion levels are not incorporated. MOBILE6.2 implicitly accounts for congestion because some urban driving patterns used in the model are associated with congestion. In contrast, driving pattern-based emission models, such as CMEM, predict emissions in congestion using instantaneous speed and acceleration/deceleration profiles as model inputs. However, predictions for congestion periods have not been fully validated (Smit, 2006). Therefore, our scenarios used the default congestion levels in MOBILE6.2’s development and calibration.
There are many other sources of uncertainty in the emission models. For CMEM, key uncertainties result from the speed-profile smoothing and the car-floating technique used to develop these profiles. This approach likely reduced differences between congestion and free-flow predictions since actual acceleration/deceleration is underestimated. Additional uncertainties result from mapping CMEM to vehicle categories, and assuming that CMEM predictions applied to both road directions. For MOBILE6.2, a key uncertainty is whether the embedded driving cycles and speed adjustments reflect the actual driving patterns. As discussed, MOBILE6.2’s ability to predict congestion-related emissions for a specific road is limited. Other uncertainties include the lack of segment-specific vehicle mix and age distributions, and the performance of the BPR model that relates traffic flow and speed. Finally, both CMEM and MOBILE6.2 are deterministic models that do not represent uncertainties in both the structures and parameters of the models.
Roadway emissions can be estimated in other ways. The new EPA Motor Vehicle Emission Simulator (MOVES; EPA, 2009) has been calibrated using a larger database than CMEM, can consider user-specified driving patterns (EPA, 2009), and provides (varying) PM2.5 estimates. Emissions might also be determined using on-board monitoring or near-road emission/concentration measurements. While expensive, onboard monitoring links transient emissions to transient speed, acceleration and deceleration parameters, and thus can capture emissions that typify stop-and-go congestion. Because such relationships can vary dramatically among vehicles, generalizations to the whole fleet may be problematic. Near-road monitoring can be difficult to couple to transient driving parameter given instrumental limitations and changes in meteorological conditions and dispersion, among other reasons, although such measurements might provide the best estimate of congestion’s contribution to pollutant levels.
4.3. Dispersion modeling
The concentration predictions involved several uncertainties and limitations, the largest of which might arise from the use of the empirical NO2–NOx relationship. This relationship was derived from a UK study, whereas the case studies used US-based traffic compositions, vehicle technologies, and emission models. Actual NO2–NOx relationships depend on many factors, e.g., background levels of NO, NO2 and O3, and meteorology (Stedman et al., 2001). The empirical relationship was derived for long-term relationships. Here it was used for short-term concentrations. The background NOx level used might not reflect levels around the studied roads. Meteorological information driving the dispersion model was obtained at an open (unsheltered) (airport) site, while conditions near roads might be affected by buildings, trees and other factors (Greco et al., 2007) that can reduce wind speed and increase turbulence. Because concentrations rapidly decrease at distances exceeding 150 m from the road, only near-road receptors were considered. This does not account for background concentrations that can be attributed to traffic. The dispersion model predictions are deterministic, and do not consider model uncertainty. Other limitations of CALINE4, e.g., its poor performance at low wind speeds, have been discussed elsewhere (Zhang and Batterman, 2010).
4.4. Exposure assessment limitations
The scenarios demonstrate key factors affecting risk trends, which do not necessarily apply to actual commuting populations. For example, commuters usually travel for longer trips than the studied segments: US commuters spent an average of 81 min day−1 in vehicles in 2001 (HEI, 2010). Such trips might include both congestion-free and congestion periods, and both freeway and arterial roads. Exposures for only two populations were examined (in-vehicle cabins for the on-road population, and in-homes for the near-road population). Dynamic adjustments to time activity patterns associated with travel delay were not considered (Zhang and Batterman, 2009). Concentrations in vehicle cabins, which can be affected by opening car windows, the air intake location, air conditioning system operation, and other factors, may differ from on-road concentrations. Similar considerations apply to indoor concentrations for near-road residents.
4.5. Risk characterization
This study provides an analysis of the incremental risks of traffic-related air pollutants in on-road and near-road environments, e.g., in vehicle cabins and locations near roads. There are several related risks or risk trade-offs that fall beyond the scope of our analysis. For example, additional time in traffic will decrease the time spent in other microenvironments, most notably at home, which can represent a risk trade-off as analyzed previously by Zhang and Batterman (2009). Second, changes in the emissions of traffic related air pollutants can promote the formation of secondary air pollutants, e.g., ozone and organic aerosols, that potentially affect a broader population, not just the near-road population. Finally, we did not evaluate risks related to “upstream” or process emissions (e.g., refining), climate change pollutants (e.g., associated with CO2 emissions), or accidents.
Several issues in the risk characterization are worth pointing out. First, congestion-specific concentration–response relationships are unavailable. The literature data may inadequately represent risks related to congestion, which typically involve shorter exposure periods (typically less than several hours) than the daily or annual periods used in most studies. It is unclear how averaging to the annual level in the present study affects true risks. Still, the NO2 concentration–response relationship used can be supported since congestion does not generate new pollutants, but simply changes concentrations of traffic-related pollutants. Also, NO2 was used as a surrogate for congestion impacts, thus representing effects of NO2 as well as other traffic-related pollutants, such as PM2.5. This might be justified given the high correlation between NO2 and several co-pollutants (EPA, 2008; Tonne et al., 2008).
Risks were calculated for individuals that were on-road and at a distance of 100 m, which incompletely accounts for the diversity of population exposures. An improved spatial analysis of traffic-related air pollutants is possible using actual population densities. Other potentially affected persons would include indoor and outdoor workers near roads.
4.6. Other approaches for estimating congestion-related health risks
Health risks from congestion might be estimated using epidemio-logical studies that include indicators for congestion. Such studies might provide tailored dose–response relationships that could be used in risk assessments. For example, congestion indicators such as time spent in congestion might be linked to health outcomes directly. This could help avoid the use of complicated and uncertain models.
4.7. Recommendations
Further research is needed to characterize exposures and risks attributable to traffic congestion. Concentration–response relationships using direct indicators of congestion are needed since previous epidemiological studies used only aggregate (and not congestion) indicators, e.g., daily traffic volume or traffic density within a buffer. Second, there is a need for emission models that directly account for congestion. The application of the new MOVES model would be useful in this context; this also requires the development of representative driving patterns portraying congestion. Third, populations living and working near roads must be known at finer resolution given that pollutant concentrations associated with traffic rapidly decrease with distance.
5. Conclusions
This study used an incremental analysis to estimate pollution impacts and characterize health risks caused by congestion, which appears to be the first of its type in the literature. Congestion can increase risks for individuals driving on freeways and arterial roads, and for individuals living or working near roads. The modeling analysis suggests that incremental risks have a “U” shaped pattern with increased traffic volume for on-road populations in the freeway case study, and a different pattern, dramatic increases at high traffic volumes, for the arterial road. Risk levels depend on many factors, including traffic volume, vehicle mix, road type and meteorology. While risks from congestion can be predicted and are potentially significant, uncertainties are also high, and thus additional information is required to confirm predictions. This study suggests that the marginal risks of additional vehicles vary, and that key risk determinants include emission factors in congestion, the NO2–NOx relationship, travel time changes, road type, and exposure location. Overall, the findings that marginal risks are not constant should be used to inform policy making related to traffic and air quality management.
Supplementary Material
HIGHLIGHTS.
Congestion and additional traffic can significantly increase exposures and risks.
Risks and exposures are not proportional to traffic volumes.
Incremental risks depend on site-specific factors including road type.
Acknowledgments
Portions of this research were funded through the support of the National Science Foundation’s Materials Use: Science, Engineering, and Society Biocomplexity Program Grant (CMS-0329416) and the University of Michigan Risk Science Center through the support of a fellowship.
Appendix A. Supplementary data
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.scitotenv.2013.01.074.
References
- Batterman S, Zhang K, Kononowech R. Prediction and analysis of near-road concentrations using a reduced-form emission/dispersion model. Environ Health. 2010;9:29. doi: 10.1186/1476-069X-9-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benson P. FHWA-CA-TL-84-15. Sacramento, CA: California Department of Transportation; 1989. CALINE4 — a dispersion model for prediction air pollutant concentrations near roadways. [Google Scholar]
- Brown SG, Wade KS, Hafner HR. [Accessed April 2, 2010];Summary of recent ambient air quality and accountability analyses in the Detroit area. 2007 http://www.epa.gov/airtrends/specialstudies/2007detroit_summary_report.pdf.
- Brugge D, Durant JL, Rioux C. Near-highway pollutants in motor vehicle exhaust: a review of epidemiologic evidence of cardiac and pulmonary health risks. Environ Health. 2007;6:23. doi: 10.1186/1476-069X-6-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Department for Environment, Food and Rural Affairs. [Accessed April 2, 2010];Part IV of the Environment Act 1995, Local Air Quality Management Technical Guidance. 2003 :6–33. http://www.ni-environment.gov.uk/technical_guidance.pdf.
- Dowling R. National Cooperative Highway Research planning report. Vol. 387. Washington DC: National Research Council; 1997. Planning techniques to estimate speeds and service volumes for planning. [Google Scholar]
- Downs A. Still stuck in traffic: coping with peak-hour traffic congestion. Washington, DC: Brookings Institution Press; 2004. [Google Scholar]
- Eliasson J, Hultkrantz L, Nerhagen L, Rosqvist LS. The Stockholm congestion — charging trial 2006: overview of effects. Transp Res A Policy Pract. 2009;43(3):240–50. [Google Scholar]
- EPA. User’s guide to MOBILE6.1 and MOBILE6.2. 2003. [Google Scholar]
- EPA. [Accessed November 20, 2009];Risk and exposure assessment to support the review of the NO2 primary National Ambient Air Quality Standard. 2008 http://www.epa.gov/ttn/naaqs/standards/nox/data/20081121_NO2_REA_final.pdf.
- EPA. [Accessed February 27, 2010];MOVES2010 policy guidance. 2009 http://www.epa.gov/otaq/models/moves/420b09046.pdf.
- Greco SL, Wilson AM, Hanna SR, Levy JI. Factors influencing mobile source particulate matter emissions-to-exposure relationships in the Boston urban area. Environ Sci Technol. 2007;41:7675–82. doi: 10.1021/es062213f. [DOI] [PubMed] [Google Scholar]
- Health effects institute. [Accessed on March 10, 2009];Traffic-related air pollution: a critical review of the literature on emissions, exposure, and health effects. http://pubs.healtheffects.org/getfile.php?u=5532010.
- Levy JI, Buonocore JJ, von Stackelberg K. Evaluation of the public health impacts of traffic congestion: a health risk assessment. Environ Health. 2010;9:65. doi: 10.1186/1476-069X-9-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michigan Department of Transportation. [Accessed April 28, 2009];Ann Arbor 2008 annual average daily traffic map. 2008 http://www.michigan.gov/documents/annarbor_19544_7.pdf & http://mdotwas1.mdot.state.mi.us/public/maps_adtmaparchive/2007cadt/Ann%20Arbor.pdf.
- Michigan Department of Transportation. [Accessed April 1, 2010];Detroit 2008 annual average daily traffic map. 2009 http://www.michigan.gov/documents/detmetro_19640_7.pdf.
- Pierce T, Isakov V, Haneke B, Paumier J. [Accessed June 26, 2009];Emission and air quality modeling tools for near-roadway applications. 2008 http://www.epa.gov/airscience/pdf/Pierceetal_EPA2008.pdf.
- Schrank D, Lomax T. [Accessed March 22, 2008];The 2007 urban mobility report. 2007 http://financecommission.dot.gov/Documents/Background%20Documents/mobility_report_2007_wappx.pdf.
- Scora G, Barth M. Comprehensive Modal Emission Model (CMEM) Version 3.01 User’s Guide. Riverside, California: University of California; 2006. [Google Scholar]
- Sjodin A, Persson K, Andreasson K, Arlander B, Galle B. On-road emission factors derived from measurements in a traffic tunnel. Int J Veh Des. 1998;20(1–4):147–58. [Google Scholar]
- Smit R. Doctoral dissertation: An examination of congestion in road traffic emission models and their application to urban road networks. Griffith University; Queensland, Australia: 2006. p. 12. [Google Scholar]
- Southeast Michigan Council of Governments (SEMCOG) [Accessed March 29, 2010];Sensitivity analysis of EPA’s new mobile model. 2004 http://library.semcog.org/InmagicGenie/DocumentFolder/SensitivityAnalysisEPAmodel.pdf.
- Southeast Michigan Council of Governments (SEMCOG) Ozone and carbon monoxide conformity analysis for the proposed amendment of the 2030 regional transportation plan for southeast Michigan draft; Detroit, Michigan. 2006. [Google Scholar]
- Stedman JR, Goodwin JWL, King K, Murrells TP, Bush TI. An empirical model for predicting urban roadside nitrogen dioxide concentrations in the UK. Atmos Environ. 2001;35:1451–63. [Google Scholar]
- Tonne C, Beevers S, Armstrong B, Kelly F, Wilkinson P. Air pollution and mortality benefits of the London Congestion Charge: spatial and socioeconomic inequalities. Occup Environ Med 2008. 2008;65(9):620–7. doi: 10.1136/oem.2007.036533. [DOI] [PubMed] [Google Scholar]
- Transportation Research Board. Special Report. Washington, DC: Transportation Research Board, National Research Council; 2002. The Congestion Mitigation and Air Quality Improvement Program, assessing 10 years of experience; pp. 60–4. [Google Scholar]
- Trueman RE. Incremental (marginal) analysis of basic inventory models. Decis Sci. 2007;2(3):341–55. [Google Scholar]
- World Health Organization. Health effects of transport-related air pollution. Copenhagen: WHO Regional Office for Europe; 2005. pp. 125–65. [Google Scholar]
- Zhang K, Batterman S. Time allocation shifts and pollutant exposure due to traffic congestion: an analysis using the national human activity pattern survey. Sci Total Environ. 2009;407:5493–500. doi: 10.1016/j.scitotenv.2009.07.008. [DOI] [PubMed] [Google Scholar]
- Zhang K, Batterman S. Near-road air pollutant concentrations of CO and PM2.5: a comparison of MOBILE6. 2/CALINE4 and generalized additive models. Atmos Environ. 2010;44:1740–8. [Google Scholar]
- Zhang K, Batterman S, Dion F. Vehicle emissions in congestion: comparison of work zone, rush hour and free-flow conditions. Atmos Environ. 2011;45:1929–39. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.