

Abstract
We describe two patients with cardiac tumors in the left atrium, which by their association and histopathological lineage, are extremely rare. The clinical, echocardiographic and pathological findings were analysed. The first case was asymptomatic, but in the control studies of colon adenocarcinoma, an intracardiac mass was found by chest computed tomography (CT). A transesophageal 3D (TEE 3D) echocardiogram revealed a left atrial mass attached to the interatrial septum. The mass was surgically removed and histopathologic findings showed myxoma. The second had history of chronic intermittent diarrhea. A thoraco-abdominal CT showed a left atrial mass. The TEE 3D echocardiography reported an intracardiac mass attached to the roof of the left atrium. The mass was surgically removed and the histopathogical findings showed a myxoma, with dystrophic ossification and extramedullary hematopoiesis. TEE 3D echocardiography provides an acceptable morphological characterisation of intracardiac masses, with good correlation with surgery.
Background
Atrial myxomas are the most common primary cardiac tumours in adults, accounting for nearly half of primary cardiac tumours.1 Cardiac myxomas develop in any of the cardiac cavities, but up to 90% of them are located in the left atrium, mainly adhered to the atrial septum near the fossa ovalis2; however, some of them have atypical localisation such as the right atrium (18% of cases)3 and, more rarely, the aorta, pulmonary artery, ventricles and vena cava; they are also, though very rarely, found in the roof of the left atrium;4 5 they exhibit a strong preference for women aged 40–60 years.1
There is no established association between cardiac myxomas and colorectal neoplasms.6 Of interest, however, is that regardless of the type of cancer, the incidence of second and third neoplasms in patients with cancer is higher than can be accounted for by chance alone.7 Atrial myxomas are mostly soft and friable without macroscopic ossification signs. Calcification is present in 10–20% of myxomas, but bone formation has been reported only in a 68-year-old woman by Ishikawa et al8 and in a 58-year-old man by Panagiotou et al.9 Echocardiography, especially three dimensional (3D) transesophageal echocardiogram (TEE), is the method of choice to assess the characteristics of echocardiographic morphology of cardiac myxomas.10 11
We describe two rare cases, one with a simultaneous left atrial myxoma and colorectal cancer, and the other with an asymptomatic left atrial myxoma with atypical localisation and areas of extramedullary haematopoiesis and extensive ossification.
Case presentation
Case 1
A 55 year-old asymptomatic woman with a history of colon adenocarcinoma diagnosed in April 2011, was treated with hemicolectomy and given chemotherapy with Capecitabine. In November 2011, a routine chest CT was performed, where an intracardiac mass was found. Cardiac auscultation was unremarkable. Laboratory data showed slight anaemia with haemoglobin of 12.5 mg/dL and haematocrit of 37.4 mg/dL. ECG of 12 derivations was normal. TEE 3D revealed an echogenic 2.25×1.34 cm left atrial mass. It had a smooth surface and was attached to the middle portion of the interatrial septum by a small pedicle (figure 1A, B). The mass was surgically removed and histopathological analysis confirmed the echocardiographic suspicion of a myxoma with a diameter of 2.4×2.1×1.4 cm and weight of 3.6 g (figure 1C). In follow-up 2 years after surgery, the patient is in NYHA functional class I and a cardiac MRI performed a year ago has demonstrated no recurrence of myxoma; also, the latest oncologic report showed remission of the colorectal cancer.
Figure 1.

Three-dimensional transesophageal echocardiography showing an anterior view of the mass attached by a short pedicle to the middle portion of the interatrial septum (A). Posterior aspect of the left atrial mass (B). Macroscopic view of the surgical specimen with areas of hemorragic appearance (C).
Case 2
A 66-year-old woman with a history of systemic arterial hypertension, diabetes mellitus type 2, gastro-oesophageal reflux and diverticular disease, was on follow-up to investigate the aetiology of her chronic intermittent diarrhoea. A thoracoabdominal CT was performed, which showed a left atrial mass. 3D transoesophageal echocardiography reported a 2.7×2.2 cm heterogeneous intracardiac mass with patchy calcification and a smooth surface attached to the roof of the left atrium by a short, thick pedicle, which was better visualised with the administration of an intravenous bolus of Definity contrast agent (figure 2A, B). The physical examination was irrelevant and the laboratory testing was normal, including the calcium level (8.5 mg/dL). A surface ECG was normal. The patient underwent surgical resection of the intracardiac mass and the histopathogical findings showed a 2.8×2.5×2 cm myxoma of 9.1 g (figure 3A, B), with areas of dystrophic ossification and extramedullary haematopoiesis (figures 4A, B); no areas of necrosis, cytological atypia or mitosis were observed.
Figure 2.
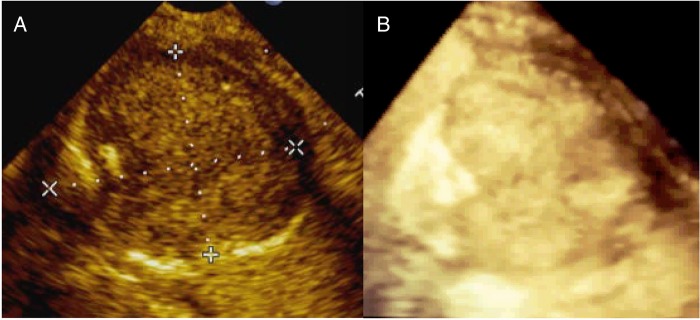
Two-dimensional transesophageal echocardiography of heterogeneous left atrial mass of 2.7×2.2 cm with a patchy calcification and a short pedicle attached to the roof of the left atrium (A), which was better visualised with 3D echo (B).
Figure 3.
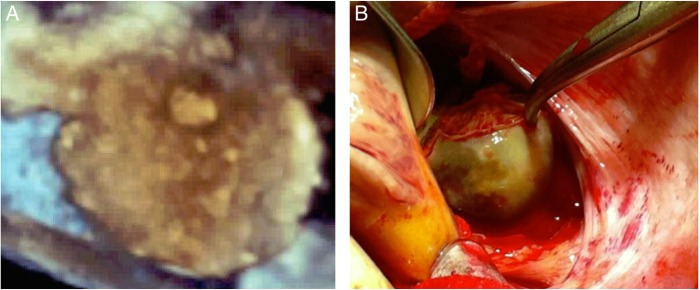
Three-dimensional aspect of the left atrial mass with patchy calcification (A) and its correlation with the surgical view (B).
Figure 4.
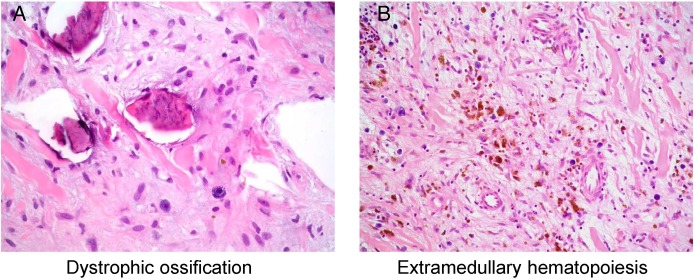
Microscopic appearance of the left atrial myxoma with areas of dystrophic ossification (A) and extramedullary hematopoiesis (B).
The patient’s evolution was satisfactory and in 1 1/2 years of follow-up no recurrence was described; the patient is in New York Heart Association (NYHA) functional class I.
Differential diagnosis
The echocardiographic differential diagnosis was mainly rhabdomyoma or thrombus.
Treatment
Surgery was opted for in both cases; it is the usual treatment of choice.
Outcome and follow-up
In 2 year follow-up, both our cases are in NYHA functional class I, without recurrence in the control transthoracic echocardiography and MRI.
Discussion
Atrial myxomas are benign growing neoplasms. Patients often present with a classic triad of symptoms: heart failure due to obstruction, stroke due to embolism and constitutional, rheumatological symptoms due to tumour secretion of interleukin-6. Embolisation to systemic or pulmonary circulation is a frequent phenomenon and is observed in approximately 30% to 40% of patients.1 12 It is usually associated with atypical symptoms and only 4% of patients remain completely asymptomatic,10 as occurred in one of our patients. All myxomas can be classified as having a smooth surface (ovoid/solid types) and those with an irregular surface (papillary/gelatinous types), according to the microscopic appearance of the tumour surface. Solid type myxomas have a tendency to form vasoforming structures and papillary type myxomas are thought to be related to embolisms.13
The two cases presented can be considered rare and with a smooth surface. In the first case, there was an unusual association of cardiac left atrial myxoma with a mucinous colorectal adenocarcinoma. To the best of our knowledge, there are only three published papers that describe the association of an atrial myxoma with colorectal adenocarcinoma,6 and polyps in the colon14 and small bowel, respectively.15
Until now, there is no established association between cardiac myxomas and colorectal neoplasm. In our patient, the colorectal cancer was surgically resected immediately after diagnosis was established and chemotherapy was given; then, in a 6-month-control CT, a cardiac tumour was found. TTE 3D plays a very important role in the diagnosis and classification, according to surface characteristics, of cardiac myxomas and has a good correlation with surgical and histopathological findings.
Similarly, some types of cardiac myxomas display areas of microscopic calcification and metaplastic bone changes, with massive ossification and extramedullary haematopoiesis, similar to lithomyxoma.16 The combination of ossified atrial myxoma with extramedullary haematopoiesis has been reported in isolation17 and in patients with Carney complex,18 which most often recurs despite adequate surgical resection. Our second case corresponds to a combination of isolated left atrial myxoma and extramedullary haematopoiesis with a very uncommon localisation to the roof of the left atrium. In this case, the diagnosis of calcified left atrial myxoma was suspected by 3D and contrast echocardiography, and histopathological examination showed dystrophic ossification and extramedullary haematopoiesis.
Conclusions
Echocardiography is the primary diagnostic imaging modality in the morphological assessment of intracardiac tumours. 3D Echocardiography provides a better morphological characterisation and classification according to the microscopic appearance of the surface of these intracardiac masses, with a good correlation with surgical and histopathological findings.
CT can accurately identify the components of the tumour and contributes to a proper diagnosis of left cardiac myxoma and its rare associations.
In both of our patients, the diagnosis was timely and accurate, with surgical curative resection of the tumours. In the 2-year follow-up no cardiac recurrence was detected.
Learning points.
Atrial myxomas are the most common primary cardiac tumours in adults.
Echocardiography plays a very important role in the diagnosis and classification, according to surface characteristics, of cardiac myxomas, with good correlation with surgical and histopathological findings.
As soon a diagnosis of myxomas is performed, patients should go to surgery in order to prevent complications.
Non-invasive imaging methods should be used for follow-up of these patients.
Footnotes
Contributors: NE-Z designed and drafted the text and selected photos, JJL-DR reviewed the literature and helped write the text, LC-L and EL-H were involved in editing the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Reynen K. Cardiac myxomas. N Engl J Med 1995;333:1610–17. [DOI] [PubMed] [Google Scholar]
- 2.Gošev I, Paić F, Durić Z et al. Cardiac myxoma the great imitators: comprehensive histopathological and molecular approach. Int J Cardiol 2013; 164:720. [DOI] [PubMed] [Google Scholar]
- 3.Diaz A, Di Salvo C, Lawrence D et al. Left and right ventricular myxoma: an uncommon presentation of a rare tumour. Interact Cardiovasc Thorac Surg 2011;12:622–3. [DOI] [PubMed] [Google Scholar]
- 4.Croti UA, Braile DM, Souza AS et al. Right ventricle and tricuspid valve myxoma [in Portuguese]. Rev Bras Cir Cardiovasc 2008;23:142–4. [DOI] [PubMed] [Google Scholar]
- 5.Nina VJS, Silva NAC, Gaspar SFD et al. Atypical size and location of a right atrial myxoma: a case report. J Med Case Reports 2012;6:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nuño IN, Kang TY, Arroyo H et al. Synchronous cardiac myxoma and colorectal cancer. Heart Inst J 2001;28:215–17. [PMC free article] [PubMed] [Google Scholar]
- 7.Schottenfeld D, Berg JW. Epidemiology of multiple primary cancers. In: Schottenfeld D, ed. Cancer epidemiology and prevention; current concepts. Springfield, IL: Thomas, 1974:416–34. [Google Scholar]
- 8.Ishikawa T, Shimizu Y, Kimura E et al. A surgical case report of ossified left atrial myxomas. Nippon Kyobu Geka Gakkai Zasshi 1996;44:1796–9. [PubMed] [Google Scholar]
- 9.Panagiotou M, Panagopoulos ND, Ravazoula P et al. Large asymptomatic Left Atrial Myxoma with ossification: case report. J Cardiothorac Surg 2008;3:19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Meng Q, Lai H, Lima J et al. Echocardiographic and pathologic characteristics of primary cardiac tumors: a study of 149 cases. Int J Cardiol 2002; 84:69–75. [DOI] [PubMed] [Google Scholar]
- 11.Espinola-Zavaleta N, Delgado-Barriga J, Soto-Abraham MV et al. Cardiac benign tumors: echocardiography and computed tomography findings in two cases with histopathologic correlation. Int Canc Conf J 2013;2:82–8. [Google Scholar]
- 12.Singh SK, Kumar A, Tewarson V et al. Calcified left atrial myxoma with osseous metaplasia. Indian J Chest Dis Allied Sci 2012;54:201–3. [PubMed] [Google Scholar]
- 13.Gao C, Yang M, Wang G et al. Excision of atrial myxoma using robotic technology. J Thorac Cardiovasc Surg 2010;139:1282–5. [DOI] [PubMed] [Google Scholar]
- 14.Jánosi A, Moravcsik E, Faller J et al. Simultaneous occurrence and treatment of right atrial myxoma and extensive colonic polyposis causing recurrent intestinal hemorrhages. Orv Hetil 1996;137:1647–50. [PubMed] [Google Scholar]
- 15.Wang Y, Sharkey FE. Myxoma of the small bowel in a 47-year-old woman with a left atrial myxoma. Arch Pathol Lab Med 2003;127:481–4. [DOI] [PubMed] [Google Scholar]
- 16.Azúa-Romeo J, Moreno E, Gomollón JP. Right atrial lithomyxoma with extramedullary hematopoiesis. Heart 2002;88:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kugai T, Chibana M. Left atrial myxoma with extramedullary hematopoiesis and ossification. Kyobu Geka 2002;55:376–8. [PubMed] [Google Scholar]
- 18.Lozada-Grande EJ, Al-Kassam Martínez D, González-Boillos M. Carney Complex. Endocrinol Nutr 2011;58:308–14. [DOI] [PubMed] [Google Scholar]