

Abstract
We describe the case of an 81-year-old woman with large bowel-obstruction caused by an impacted gallstone. An 81-year-old, Caucasian, fully independent woman without significant comorbidities presented with absolute constipation, faecal vomiting and abdominal pain. Abdominal radiography revealed dilated small bowel, and a subsequent contrast CT demonstrated a 2.5 cm gallstone in the sigmoid colon. This is believed to have entered the transverse colon via a cholecyst-colonic fistula, and then migrated to a section of sigmoid colon affected by diverticular disease, where it became impacted. Two sigmoidoscopic removals were attempted but were unsuccessful as the gallstone's size prevented removal with an endoscopic basket. A laparotomy was performed and the stone extracted via a sigmoid enterotomy. No covering stoma was formed, and following 48 h on intensive trauma unit and a short ward-based stay for rehabilitation, the patient was discharged home and is currently doing well.
Background
The most common causes of large bowel obstruction are colorectal adenocarcinoma, diverticular disease, volvulus and inflammatory bowel disease.1 Gallstones are known to cause small bowel obstruction in approximately 1–3% of cases,2 but have only very rarely been described as a cause of large bowel obstruction.3–7 Previously documented cases have almost universally been managed with at least one of either a colonic resection or stoma formation, and have tended to result in death or significant postoperative morbidity. We wished to demonstrate how with attentive physiological optimisation, and prompt diagnosis and surgical intervention, patients with large bowel obstruction secondary to gallstones can be managed with enterotomy alone, sparing them the morbidity of colonic resection and stoma formation.
Case presentation
An 81-year-old woman with a background of osteoarthritis and previous acute kidney injury presented with a 4-day history of absolute constipation and recurrent episodes of faeculant vomiting. She described colicky epigastric pain which over the period of constipation had migrated and become localised to the left iliac fossa. She had no intestinal or extraintestinal symptoms to suggest colonic malignancy, nor had she previously undergone any intra-abdominal surgery. Several months earlier she had presented to A and E with symptoms of biliary colic that resolved with simple analgesia. At that time, her liver function tests were normal and she was discharged home without imaging of the gallbladder.
On examination, she was haemodynamically stable, with a heart rate of 89 bpm, blood pressure of 127/61, respiratory rate of 12 breaths per minute and oxygen saturations of 92% on room air. Abdominal examination revealed mild distension with a tender palpable loop of bowel in the left iliac fossa. Bowel sounds were present and normal, and no herniae were identified. Digital rectal examination revealed soft brown stool with no evidence of malaena. She was not peritonitic.
Investigations
Blood tests on admission revealed a raised C reactive protein of 31.8 and mildly deranged renal function (urea 17.1 and creatinine 113), but a normal full blood count, bilirubin, alkaline phosphatase and alanine transaminase.
An initial abdominal radiograph (figure 1) revealed dilated loops of small bowel in the right lower quadrant with very little gas in the large bowel, consistent with distal small bowel obstruction. Erect chest radiography revealed a massive diaphragmatic hernia, but no evidence of free intra-abdominal air. Abdominal CT with contrast demonstrated a 2.5 cm gallstone within the mid-sigmoid colon (figures 2 and 3), impacted in an area affected by diverticular disease. It was unclear from the CT scan whether a stricture was present in this area of sigmoid colon. A second gallstone was demonstrated within the gallbladder along with both intrahepatic and extrahepatic pneumobilia. The transverse colon was identified lying in close proximity to the gallbladder, and although not positively identified on CT scanning, it was felt likely that a fistula existed between gallbladder and transverse colon, providing the entry point for the gallstone into the colon without it having to first traverse the ileocaecal valve.
Figure 1.

Abdominal radiograph showing dilated loops of small bowel with an opacity within the pelvis.
Figure 2.
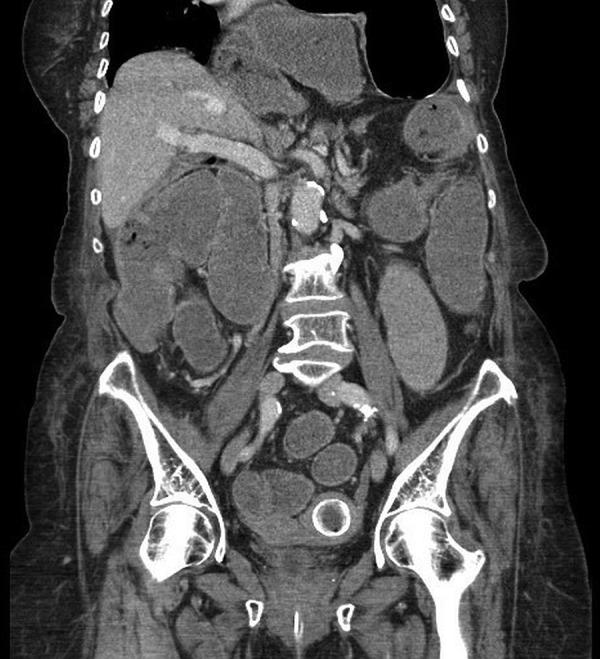
Coronal CT slice showing 2.5 cm gallstone in the sigmoid colon.
Figure 3.

Axial CT imaging revealing 2.5 cm gallstone in the sigmoid colon.
Retrospective analysis of the abdominal film taken on admission demonstrates an opacification in the pelvis, felt likely to be the offending gallstone.
Differential diagnosis
Prior to CT imaging, the differential diagnoses are as below.
Large bowel obstruction secondary to:
Malignancy.
Complications of diverticular disease.
CT of the abdomen and pelvis confirmed the diagnosis of large bowel obstruction secondary to gallstones.
Treatment
In order to attempt to spare the patient the morbidity of a general anaesthetic and laparotomy, sigmoidoscopic removal of the stone was attempted twice prior to surgical intervention. The initial attempt identified an impacted gallstone within inflamed diverticular tissue at around 40 cm proximal to the anal verge. The stone was successfully disimpacted, but complete endoscopic removal was not possible as inadequate bowel preparation led to poor visualisation of the stone. Following the first unsuccessful sigmoidoscopy, bowel preparation was given with phosphate enemas and repeat sigmoidoscopy was performed. The gallstone was visualised, but was too large for extraction with an endoscopic basket. The procedure was abandoned when the patient experienced abdominal pain, presumably due to excessive insufflation of the proximal colon and at this point it was decided to proceed to surgical extraction.
At laparotomy, grossly distended caecum and small bowel were identified, along with moderately significant diverticular disease. There was no evidence of intestinal ischaemia or perforation. The gallstone was identified impacted in the sigmoid colon.
Unfortunately the colon could not be adequately decompressed preoperatively, as it was not possible to pass a scope proximal to the offending stone to enter the area of distended colon. Suction-decompression of the proximal colon and small bowel was therefore performed via an appendiceal enterotomy, before an appendicectomy was performed. The gallstone (figure 4) was extracted via a 2.5 cm sigmoid enterotomy that was closed primarily using 3/0 PDS interrupted sutures. Digital examination of the colonic lumen distal to the enterotomy revealed a benign feeling stricture, which though narrowed, would allow passage of a digit, and therefore resection was deemed unnecessary. A 30F Robinson's drain was placed adjacent to the repair, but due to the fact that there had been no intra-abdominal contamination, and the sigmoid enterotomy had been made within macroscopically healthy tissue, the decision was taken not to form a covering stoma. The cholecyst-enteric fistula was not positively identified intraoperatively, as the decision had been made during preoperative planning not to attempt any resection of the fistulous tract or to perform a cholecystectomy.
Figure 4.
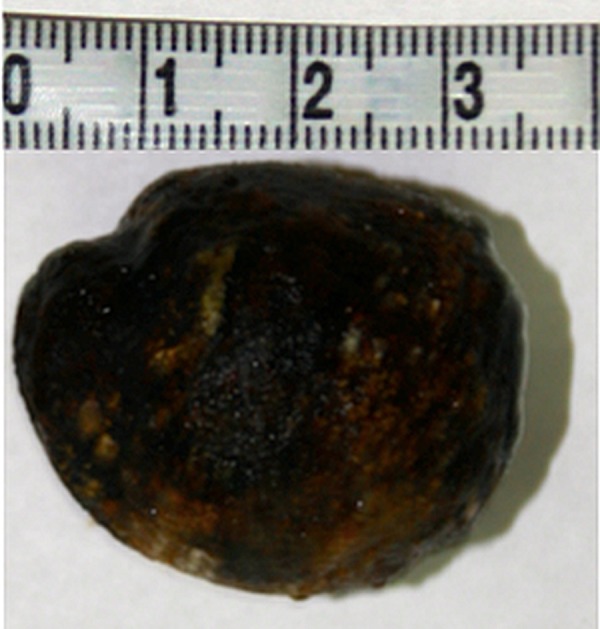
The offending gallstone after removal via sigmoid enterolithotomy.
The patient remained stable throughout the operation, but was admitted to intensive trauma unit for observation for 24 h postoperatively. No inotropic, ventilatory or renal support was required. She remained an inpatient for 12 days postoperatively for physiotherapy input and gradual reintroduction of a full enteral diet before being discharged back to her own home.
Outcome and follow-up
Following discharge, an intensive community-based rehabilitation programme was implemented in order to aid her return to baseline mobility. At telephone follow-up 3 months postdischarge, she was doing well, and had returned to full independent living. No subsequent cholecystectomy has been performed.
Discussion
Gallstone ileus is rare and occurs predominantly in women over the age of 65, many of whom have multiple comorbities.8 9 Owing to the affected population, and an often delayed diagnosis, it is associated with a postoperative mortality of up to 18%.10 Large bowel obstruction secondary to gallstones is even rarer than gallstone ileus, and is suggested to account for between 2% and 8% of all cases of intestinal obstruction resulting from gallstones.11 Given the rarity of large bowel obstruction secondary to gallstones, no consensus has been reached on the optimal management. Options include endoscopic removal, simple enterotomy with or without covering stoma formation, and a Hartmann's procedure. There is also debate as to whether cholecystectomy and correction of the cholecyst-enteric fistula should be performed at the time of gallstone extraction.
A large case-series of gall-stone ileus concluded that a one stage procedure including cholecystectomy and fistula correction was associated with significant excess mortality, and that simple enterolithotomy should be the procedure of choice.10 We have shown this approach to be a successful option for the treatment of large bowel obstruction secondary to gallstones, and one that when combined with prompt diagnosis can be associated with a rapid postoperative recovery and return to premorbid function. It is important to note that because our patient had no on-going symptoms of biliary disease, and because cholecystectomy in a patient of this age with previous laparotomy was likely to be a major operation, it was decided that an interval cholecystectomy should not be performed. To date, she has suffered no adverse events as a result of this decision, although there is obviously the potential for enteric obstruction as a result of movement of the second gallstone that was noted within her gallbladder.
We have also presented a novel technique for decompression of the proximal colon prior to extraction of the impacted stone. Interestingly, a literature review of the management of gallstone ileus has concluded that it is ‘unlikely that a trial of enterolithotomy versus one-stage surgery could be performed’ given the rarity of cases and the high-risk nature of the patients.12 The review concludes it may be a condition in which treatment choice will continue to be based on the clinical judgement of the surgical team.
More recent case reports describe the use of endoscopic lithotripsy as a surgery-sparing treatment for colonic gallstones that are endoscopically accessible,13–15 but not amenable to removal with a retrieval basket. Options include mechanical, electrohydraullic or laser lithotripsy, or a combination thereof. Similar techniques have been described in relation to cases of upper gastrointestinal gallstone ileus,13 15 but only very few have been performed in cases of colonic obstruction.
Impaction of the gallstone in our patient was associated with underlying complicated diverticulosis. Previous case reports have also documented the presence of active diverticulitis in the area of colon in which a gallstone has become impacted.3 We would therefore suggest that areas of active inflammation or stricturing within the colon may predispose to impaction of gallstones that have entered the gastrointestinal tract through a cholecyst-enteric fistula. Our case would also support the belief that it is stones of around 2.5 cm or larger that result in obstruction when there is an underlying pathology present.16
While large bowel obstruction secondary to gallstones is rare, it should not be ignored as a potential cause of large bowel obstruction in patients whose symptoms and medical history do not classically fit the presentation of one of the more common causes. Our case has provided further evidence that this entity appears to occur most commonly in elderly Caucasian women. We would suggest that it is valid to attempt sigmoidoscopic extraction of the impacted stone prior to surgical intervention, though operators should proceed with caution due to the risk of causing caecal distension and subsequent perforation secondary to excessive insufflation. In the absence of any intestinal ischaemia or perforation, simple enterolithotomy without covering stoma appears to be an acceptable definitive surgical intervention. Following this, affected patients can make a rapid return to their premorbid level of functioning.
Learning points.
While rare, gallstones should not be ignored as a potential cause of large bowel obstruction, particularly in those with underlying colonic pathology and prior symptoms suggestive of gallstone disease.
Sigmoidoscopic removal of the impacted stone may be attempted in patients who are haemodynamically stable, in order to attempt to avoid the morbidity associated with a general anaesthetic and laparotomy. Endoscopic lithotripsy has also been described as a possible treatment for those unfit for surgery. Following on from this case however, we would advocate only a single attempt at sigmoidoscopic removal prior to proceeding to surgical extraction.
Decompression of the proximal colon via the appendix, followed by simple enterolithotomy without covering stoma appears to be an acceptable surgical treatment for large bowel obstruction secondary to gall stones.
Current evidence would appear to suggest it is safer not to perform cholecystectomy at the time of removal of obstructing gallstones. Leaving the gallbladder in situ in our patient does not appear to have caused any long-term morbidity, and until higher levels of evidence are available, we would advocate this approach for future cases of large bowel obstruction secondary to gallstones.
Contrary to what has been seen with the majority of previously published case reports, patients with large bowel obstruction secondary to gallstones have the potential to make a rapid recovery and return to their premorbid condition.
Footnotes
Contributors: KS drafted the initial case report which was edited by BA. KS and BA were involved in writing the discussion (including a literature search) and the learning points. MS and TY provided details about the case and critically edited the report.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Sawai RS. Management of colonic obstruction: a review. Clin Colon Rectal Surg 2012;25:200–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Martinez Ramos D, Daroca Jose JM, Escrig Sos J et al. Gallstone ileus: management options and results on a series of 40 patients. Rev Esp Enferm Dig 2009;101:117–20, 21–4. [DOI] [PubMed] [Google Scholar]
- 3.Ball WR, Elshaieb M, Hershman MJ. Rectosigmoid gallstone coleus: a rare emergency presentation. BMJ Case Rep 2013;2013:pii: bcr2013201136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Athwal TS, Howard N, Belfield J et al. Large bowel obstruction due to impaction of a gallstone. BMJ Case Rep 2012;2012:pii: bcr1120115100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ranga N. Large bowel and small bowel obstruction due to gallstones in the same patient. BMJ Case Rep 2011;2011:pii: bcr0920103372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Van Kerschaver O, Van Maele V, Vereecken L et al. Gallstone impacted in the rectosigmoid junction causing a biliary ileus and a sigmoid perforation. Int Sur 2009;94:63–6. [PubMed] [Google Scholar]
- 7.Vaughan-Shaw PG, Talwar A. Gallstone ileus and fatal gallstone coleus: the importance of the second stone. BMJ Case Rep 2013;2013:pii: bcr2012008008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ayantunde AA, Agrawal A. Gallstone ileus: diagnosis and management. World J Surg 2007;31:1292–7. [DOI] [PubMed] [Google Scholar]
- 9.Brezean I, Aldoescu S, Catrina E et al. Gallstone ileus: analysis of eight cases and review of the literature. Chirurgia (Bucur) 2010;105:355–9. [PubMed] [Google Scholar]
- 10.Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg 1994;60:441–6. [PubMed] [Google Scholar]
- 11.Osman N, Subar D, Loh MY et al. Gallstone ileus of the sigmoid colon: an unusual cause of large-bowel obstruction. HPB Surg 2010;2010:153740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ravikumar R, Williams JG. The operative management of gallstone ileus. Ann R Coll Surg Engl 2010;92:279–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zielinski MD, Ferreira LE, Baron TH. Successful endoscopic treatment of colonic gallstone ileus using electrohydraulic lithotripsy. World J Gastroenterol 2010;16:1533–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Alkhusheh M, Tonsi AF, Reiss S et al. Endoscopic laser lithotripsy for gallstone large bowel obstruction. Int J Case Rep Images 2011;2:11–14. [Google Scholar]
- 15.Reiss G, Gopi R, Ramrakhiani S. Unusual cause of colonic obstruction: gallstone impaction requiring mechanical lithotripsy. Clin Gastroenterol Hepatol 2009;7:A20. [DOI] [PubMed] [Google Scholar]
- 16.Tucker A, Garstin I. A peculiar cause of bowel obstruction. Int J Surg Case Rep 2013;4:473–6. [DOI] [PMC free article] [PubMed] [Google Scholar]