

Abstract
Objective
The purpose of this study was to evaluate publicly available information of chiropractic technique systems that advocate radiography for subluxation detection to identify links between chiropractic technique systems and to describe claims made of the health effects of the osseous misalignment component of the chiropractic subluxation and radiographic paradigms.
Methods
The Internet and publicly available documents were searched for information representing chiropractic technique systems that advocate radiography for subluxation detection. Key phrases including chiropractic, x-ray, radiography, and technique were identified from a Google search between April 2013 and March 2014. Phrases in Web sites and public documents were examined for any information about origins and potential links between these techniques, including the type of connection to BJ Palmer, who was the first chiropractor to advocate radiography for subluxation detection. Quotes were gathered to identify claims of health effects from osseous misalignment (subluxation) and paradigms of radiography. Techniques were grouped by region of the spine and how they could be traced back to B.J Palmer. A genealogy model and summary table of information on each technique were created. Patterns in year of origination and radiographic paradigms were noted, and percentages were calculated on elements of the techniques’ characteristics in comparison to the entire group.
Results
Twenty-three techniques were identified on the Internet: 6 full spine, 17 upper cervical, and 2 techniques generating other lineage. Most of the upper cervical techniques (14/16) traced their origins to a time when the Palmer School was teaching upper cervical technique, and all the full spine techniques (6/6) originated before or after this phase. All the technique systems’ documents attributed broad health effects to their methods. Many (21/23) of the techniques used spinal realignment on radiographs as one of their outcome measures.
Conclusion
Chiropractic technique systems in this study (ie, those that advocate for radiography for subluxation misalignment detection) seem to be closely related by descent, their claims of a variety of health effects associated with chiropractic subluxation, and their radiographic paradigms.
Key indexing terms: History, 20th century, Chiropractic, Radiography, Spine
Introduction
In 1910, BJ Palmer was President of the Palmer School and Infirmary of Chiropractic in Davenport, IA, which his father, DD Palmer had founded. During this time, he adopted the relatively new technology of radiographic assessment using x-rays to visualize the spine. He began to promote radiography in his effort to visualize the misalignment component of chiropractic subluxations. In 1919, BJ Palmer reflected on the use of radiography, “The original Chiropractic purpose was not to use the X-Ray for therapeutic purposes, to ascertain normal or abnormal tissues, the character of a fracture or whether there was renal calculi [sic] or a bullet in the body. We had already settled how a cure occurred; we did not care much about pathological plates… the advent of the X-Ray into Chiropractic was to prove that vertebral subluxations did actually exist.…” [emphasis original]1 Thus, in the early years, according to BJ Palmer, the main goal in using radiographs was to detect the visible misalignment component of vertebral subluxations. Later on, BJ Palmer adopted additional tools for identifying the neurological component of the subluxation complex, such as the neurocalometer.2
Of the adoption of radiography, it is claimed that BJ Palmer shifted the focus of chiropractic analysis from the nervous system to the osseous system with the introduction of x-ray technology for detecting minute spinal misalignments.3 This may have been an overstatement because the neurological aspect of subluxation was retained; however, it does reflect the importance gained by his quest to visualize spinal misalignments. In essence, the “misaligned bone” represented the visible component of the “cause of disease,” otherwise known as the chiropractic subluxation.1,4–6 It was theorized that, without the misaligned bone, nerve dysfunction would not exist and thus disease would not manifest. This paradigm held supremacy in the early years of chiropractic in the battle against disease, “dis-ease,” and in regaining health; and it was claimed that the radiograph was the key to finding these misalignments. In the introduction to Chiropractic Spinography (1919), BJ Palmer wrote, “the sunnum bonum of all life and death, health or disease issues pivoted around a study of the correct or incorrect position of vertebrae.”7 Although there was some initial backlash to including technology in a profession that focused on manual therapy,3 techniques subsequently developed and adopted this concept.
BJ Palmer called the practice of spinal radiography spinography; and in 1919, he wrote that the radiograph had given the ultimate vindication for his approach to health care.1 This approach was in contrast to other health care paradigms, the closest to chiropractic at that time being traditional osteopathy. There was some early exploration of the use of radiography in the search for osteopathic lesions.8 However, unlike chiropractic, osteopathy never embraced radiography with the same vigor as chiropractic. A search of early to mid-20th century osteopathic texts revealed passing references to the use of x-ray and then often only as a therapeutic measure.9–15
Prior to the advent of radiography as a clinical tool, manual palpation of the vertebrae had been the primary method of finding chiropractic subluxations.16 Upon introduction, radiography was then seen as more important for at least 14 years that followed, until the advent of the Neurocalometer. Thompson wrote, “Today spinography is used to interpret spines which have not been palpated; to correct the interpretations made by palpation; to learn of the reasons why our palpation may have been at fault, in living people, that absolute readings may be determined beyond a shadow of doubt, upon which adjustments can be given with a perfect degree of assurance of being properly adjusted in which all hitherto elements of doubt are entirely obliterated.”7 This change to radiography as the primary method had important consequences. Radiographic measurements of spinal misalignments became a central feature of many chiropractic practices.17 As various new technique systems were developed through the 20th century, some required radiography for the detection or quantification of subluxations, with patients being radiographed as part of the initial analysis.18–24 Some of these radiographically oriented techniques used additional methods to detect nerve vertebral subluxation, such as static palpation, motion palpation, and paraspinal temperature measurements.25
Up to this time, Palmer had advocated the Meric System, in which each vertebral level of the entire spine was responsible for a different set of organs.4 After focusing on the full spine for subluxation detection, BJ Palmer changed his approach. In this next phase, he claimed that only the 2 upper cervical vertebrae, known as the atlas and axis, along with the base of the occiput, were of significance. This heralded his “Upper Cervical” phase.26 In 1935, Palmer announced, “In the spring of 1930 we proclaimed the principle of Hole-in-One, that there could be only one place in the spinal column that a subluxation could exist, and that was at the occipito-atlanto-axial region; that there could be a subluxation at no other place in the spinal column; that there never had been a subluxation below the inferior of Axis; that we have never adjusted a subluxation below the inferior of Axis. You have never got a sick person well by anything you ever did below the inferior of Axis.”27 Although BJ Palmer promoted the concept of upper cervical techniques, it has been suggested that the concept originated with a chiropractor named Aleck August Wernsing.28 The change to a limited spinal region was a radical idea. BJ Palmer adhered to the upper cervical focus, using it as the curriculum at his school until 1950. The Palmer School changed the curriculum under pressure from the reports of students failing state board examinations because they had only been taught upper cervical technique.29 Over the decades and various techniques espoused by the Palmer School, a number of technique systems were developed based on both the upper cervical and the full spine.
Historically, this raises several questions. How are chiropractic techniques related to each other? Did techniques that use radiography develop from variations to BJ Palmer’s teaching, or were there other sources of influence? What are the possible lines of descent and relationships to each other in terms of a radiographic paradigm? To the author’s knowledge, these questions have not yet been answered from the perspective of their use of plain film radiography. Therefore, the purpose of this study was to evaluate publicly available information from Web sites of chiropractic technique systems that advocate radiography for subluxation detection to identify links between chiropractic technique systems and to describe any claims made of the health effects osseous misalignment attributed to chiropractic subluxation and radiographic paradigms.
Methods
Definition of Terms
Line of descent was used in the genealogical sense, meaning that if the Web site or public source document stated that the technique was derived from another, the second technique was considered the “child,” descended from the earlier “parent” technique. Degree of separation for this study was used to mean closeness of relation (ie, mother and son have 1 degree of separation; a father and granddaughter have 2 degrees of separation). In this study, degree of separation was determined from the reference point of BJ Palmer who is used as the anchor, or originator of the systems that use radiography for subluxation detection. One degree of separation was indicated by having been taught by BJ Palmer (eg, attending the Palmer School while BJ was still alive) or from statements referencing BJ Palmer’s work as the basis for the radiographic methods of the technique. Two degrees of separation were determined if it was taught by one of BJ Palmer’s students (eg, Kale developed his technique based on work with Lyle Sherman, who was taught by BJ Palmer). The generic term treatment, rather than adjustment, was used because not all the techniques used high-velocity, low-amplitude osseous adjustments as their sole treatment method and the exploration of the different types of adjustments and other treatment methods is beyond the scope of this article. Paradigm of radiography means the broad approach to the value of diagnostic imaging, not the specifics of patient positioning, subluxation marking systems, or tools used to assist with obtaining images. For example, one paradigm may be that radiography should only be used in the presence of clinical “red flags.” Another may be that the primary use of radiography is to find biomechanical changes. In this study, part of the radiographic paradigm was within the inclusion criteria, that is, a technique must have stated that it advocated radiography for the detection or quantification of chiropractic subluxations. However, other elements of the paradigm or variations of the paradigm were considered likely to emerge upon collection of the data. An additional inclusion criterion was that a technique system had to be a named technique. All available techniques were considered, and techniques were not excluded if they no longer existed at the time of data collection. However, practices involving modifications or incomplete versions of a technique were excluded. Because of inconsistency in the writings on the use of the terms misaligment and subluxation, the term subluxation was used to refer to the misaligned bone; and subluxation complex was reserved for the misaligned bone along with nerve interference and organ dysfunction.
Data Collection and Analysis
To establish a list of techniques, the key phrases chiropractic x-ray, chiropractic radiography, chiropractic x-ray line drawing, and chiropractic subluxation were searched on Google between April 2013 and March 2014. PubMed was searched with the terms chiropractic and technique and x-ray. Cooperstein and Gleberzon’s Technique Systems in Chiropractic25 was also used as a source, and experts in the fields of chiropractic history and technique systems were consulted for sources. The writings of BJ Palmer on his radiographic paradigm were used as sources of information for his techniques, specifically, The Subluxation Specific The Adjustment Specific,26 Answers,5 Chiropractic Clinical Controlled Research,6 The Science of Chiropractic,4 and BJ Palmer’s Introduction to EA Thompson’s Chiropractic Spinography,1 as well as quotes from historically scholarly secondary sources such as Keating’s B.J. of Davenport,3 Dye’s The Evolution of Chiropractic,27 Wardwell’s Chiropractic: History and Evolution of a New Profession,30 and Moore’s Chiropractic in America.31
The official Web site, textbook, and/or papers or magazine articles for each technique, as well as the book Who’s Who in Chiropractic International,32 were searched for information on the history of the origin of the technique and the paradigm for the use of radiography. Only publicly available documents were used for this study because they represent chiropractic to the world. It is unknown how many chiropractors practice each technique. However, the importance of the technique lay not in numbers of adherents but rather in the availability of the information.
Lists of quotes were gathered from each of the Web sites and sources to identify lineage and demonstrate the techniques’ claims of broad health effects from chiropractic subluxation and paradigms of radiography. A brief historical vignette of each technique’s origin was written to synopsize descent and radiographic paradigm. Techniques were grouped by spinal region and line of descent. The full spine techniques were those that demonstrated evidence of operating on the principle that all the vertebrae in the spine had the potential to become subluxated. The upper cervical techniques regarded only the articulations of the skull and the top 2 vertebrae as the areas of subluxation development. The degrees of separation from BJ Palmer were noted, where appropriate, to create a genealogy model and summary table of information on each technique. Lineages were determined by finding acknowledgement of a mentor or reference to a technique that was used as a basis for a newer technique. If this information was not found, it was assumed from the originator’s school of graduation. For instance, if an originator graduated from the Palmer School during the time that BJ Palmer was alive, Palmer was assumed to be the main influence for the descendent technique, unless information to the contrary was discovered. The year of technique development was compared with BJ Palmer’s teachings as they changed over time, that is, the times he was advocating full spine technique and the period in which he changed to upper cervical. Patterns in year of origination and radiographic paradigms were noted, and percentages were calculated on elements of the techniques’ characteristics in comparison to the entire group.
Specifics of adjustment procedures and radiographic protocols are not the subject of this study and may be found elsewhere.25
Results
Twenty-three technique systems using radiography for subluxation detection were identified and divided into 2 main lines of descent: full spine and upper cervical. Some techniques were developed directly from BJ Palmer’s teachings, some through 1 or more subsequent generations of techniques, and some seemingly independently.
The full spine line of radiographic techniques was comprised of Chiropractic BioPhysics (CBP), Gonstead, Logan Basic, Pierce/Stillwagon, and Spinal Stressology. Applied Spinal Biomechanical Engineering (ASBE) was a full spine technique but acknowledged no particular forerunner. Chiropractic BioPhysics also credited upper cervical practitioner Pettibon with influence.33 BJ Palmer’s own full spine technique was not included here because it is essentially the forerunner to all the others and was discussed as such.
The upper cervical techniques developed from 3 basic lines: one from Palmer Upper Cervical Specific/“Hole-in-One” (HIO)/Toggle Recoil and others from 2 of his followers: John F Grosic and Ralph Gregory. From Palmer came Applied Upper Cervical Biomechanics (AUCB), Blair, Duff, Grostic, Kale, Knee Chest Upper Cervical Specific (KCUCS), Mears, Sutter, and Zimmerman. Grostic’s ideas were modified for Atlas Orthogonality, Cowin Upper Cervical Orthogonal, (Society for Chiropractic) Orthospinology, and Pettibon. Pettibon began as upper cervical but transitioned to full spine.34 The upper cervical aspect seemed to retain prominence, at least radiographically34; and for the percentages calculated in this article, it was put in the Upper Cervical category. Ralph Gregory, a collaborator of Grostic, founded the National Upper Cervical Chiropractic Association (NUCCA), which, in turn, inspired Spinal Orthopaedic Neurological Advancement and Research (SONAR). Advanced Orthogonal acknowledges the input of both Grostic and Gregory. See Figure 1 for a family tree and Table 1 for a summary of techniques, their originators, the dates of origin, outcome measure (posttreatment radiographs), and degrees of separation from BJ Palmer.
Figure 1.
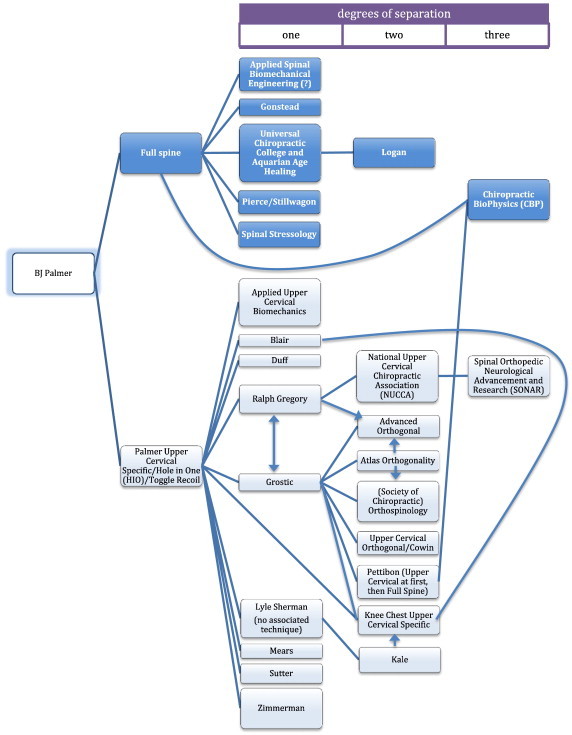
Family tree of technique systems that use radiography for chiropractic subluxation analysis. Note: “?” indicates uncertain lineage. (Color version of figure is available online.)
Table 1.
Summary of Technique Systems That Use Radiography for Chiropractic Subluxation Analysis
| Technique Name | Originator(s) | Year of Origination | Family Line | Posttreatment Radiographs? | DoS |
|---|---|---|---|---|---|
| Advanced Orthogonal | G Stanford Pierce Sr and Jr | 2001 | UC—Grostic and Gregory | Yes | 2 |
| ASBE | Ronald J Aragona | Mid-1970s | Full spine | Yes | 1 or N/A? |
| AUCB | International Upper Cervical Chiropractic Association | 1993 | UC—Palmer | No—thermography | 1 |
| Atlas Orthogonality | Roy Sweat | 1981 | UC—Grostic | Yes | 2 |
| Blair | William G Blair | 1961 | UC—Grostic | No—thermography | 1 |
| CBP | Don and Glenn Harrison | 1985 | Full spine and UC—Grostic | Yes | 3 |
| Duff Method of Analysis | Stephen A Duff | 1970s | UC—Palmer | Implied | 1 |
| Gonstead | Clarence Gonstead | Late 1920s | Full spine | Yes | 1 |
| Grostic | John F Grostic | Late 1930s | UC—Palmer | Yes | 1 |
| Kale | Michael U Kale | 1950-1980 | UC—Palmer via Sherman | No—thermography | 2 |
| KCUCS | Robert Kessinger | 2001 | UC—Palmer and Grostic via Kale and Blair | Yes | 1/2/3 |
| Logan Basic | Hugh B Logan | Early 1930s | Full spine | No | 2 |
| Mears | Donald B Mears | 1930s | UC—Palmer | Yes | 1 |
| NUCCA | Ralph Gregory | 1966 | UC—Grostic and Palmer | Yes | 2/1 |
| Society of Chiropractic Orthospinology | Roy Sweat and others | 1977 | UC—Grostic | Yes | 2 |
| Palmer Upper Cervical Specific (HIO/Toggle Recoil) | BJ Palmer | 1930 | UC—Palmer | No | 0 |
| Pettibon | Burl Pettibon | Late 1960s | UC—Grostic | Yes | 2 |
| Pierce/Stillwagon | Walter “Vern” Pierce and Glenn Stillwagon | 1970s | Full spine | Yes | 1 |
| SONAR | Thomas R Elliott | 1970s | UC—Gregory | Yes | 3 |
| Spinal Stressology | Lowell Ward | 1960s | Full spine | Implied | 1 |
| Sutter Specific Atlas Correction | Max Sutter | 1941 | UC—Palmer | Yes | 1 |
| Upper Cervical Orthogonal (Cowin) | Robert Cowin and Kathleen Bras | 1970s | UC—Grostic | Yes | 3 |
| Zimmerman | Arden D Zimmerman | 1943 | UC—Palmer | Implied | 1 |
DoS, degree of generational separation from BJ Palmer; UC, upper cervical technique.
Only 2 (33%) of 6 full spine technique originators attended the Palmer School, whereas 10 (63%) of 16 (not including BJ Palmer’s own technique) of the upper cervical techniques’ originators attended the Palmer School. Whether or not their originators attended the Palmer School, 14 (88%) of 16 of the upper cervical techniques traced their origin to a time when the Palmer School was teaching this method (1934-1950); and all the full spine techniques (6/6) originated before or after this phase. Eight (35%) of 23 of the technique originators credited chiropractic with restoring their health, citing these events as professionally inspirational.
The techniques did not always modify the radiographic portion of their predecessors; Mears, (the Society of Chiropractic) Orthospinology, SONAR, and Zimmerman all adopted existing subluxation detection methods, changing only their treatment techniques. Ten (43%) of the 23 systems made statements that their diagnostic/analytic and treatment methods were unchanged over time, or they deferred to the methods of previous practitioners. These systems include the 4 just mentioned as well as Gonstead, AUCB, Kale, KCUCS, Sutter, and Grostic.
Publicly available information from all the 23 techniques contained assertions of broad health effects from their methods. For example, Advanced Orthogonal: “By God’s design, the balanced function of the brain and nervous system is essential to the integrity of health. Our focus is on identifying and correcting the structural causes of this dysfunction, to restore and maintain the health and well-being of all those whom we serve.”35 Atlas Orthogonality: “When the atlas bone is properly aligned… the rest of the spinal vertebra [sic] come into better alignment allowing the body to heal itself.”18 (Society of Chiropractic) Orthospinology: “When a Vertebral Misalignment causes the nervous system to initiate imbalances of the body systems, it is known as a Vertebral Subluxation Complex. Once… corrected and the “static” removed, the body can return to a state of balance.’36 See Appendix 1 for examples from all the techniques sampled for this article.
Some techniques separated the vertebral misalignment from the subluxation complex, as BJ Palmer did when he introduced the neurocalometer in 1924 specifically to detect the nerve interference created by the misaligned bone.2 Gonstead reportedly claimed to be “one of the most advanced and scientific methods [of correcting] spinal misalignments, joint dysfunctions and subluxation complexes.”20 Other techniques called the misalignment a subluxation, which caused changes to neurological function, as seen with ASBE: “A chiropractic doctor detects and corrects these spinal misalignments (vertebral subluxation causing nerve interference).…”37 Sutter: “The exact variation of the atlas subluxation in relation to its surrounding structures peculiar to the individual case must be accurately determined. This can only be done through a specialized X-ray technique and analysis.”23 Still other techniques interchangeably used the terms misalignment and subluxation. Grostic: “When the vertebrae become misaligned (subluxated) a decrease of innate vital energy between the brain and the body occurs.”38 Kale: “The ‘Specific Chiropractor’ (‘Brain Stem Specialist’) is trained to locate and remove this subluxation (misalignment) and restore the vertebrae to its normal position.”39 National Upper Cervical Chiropractic Association: “[had] been quietly and accurately measuring and correcting upper cervical misalignments (subluxations) for more than sixty years.”40 Even BJ Palmer’s treatment of the concept sometimes referred to the visible misalignment as equating the subluxation: “The advent of the X-Ray into Chiropractic was to prove that vertebral subluxations did actually exist and could be so proven with the aid of the X-Ray make this visible to the eye.”7
A majority, 15 (65%) of 23 of the technique systems, not only relied on radiography to determine the presence and severity of subluxations are in the spine but also used radiography as the sole outcome measure by which they determine the success of their methods. Three techniques did not explicitly state the use of posttreatment radiographs but implied such by their emphasis on subluxation as the chief factor in health and mentioned no other outcome measure. Three additional techniques used thermography as evidence of reduced subluxation. In total, 21 (91%) of 23 techniques used spinal alignment/apparent corrected subluxation as the sole or main outcome measure. The 2 that were found to use the health of the patient rather than subluxation reduction as the main outcome measure were Logan and Palmer.
The Techniques
The following are the techniques that were found. They are divided into full spine and upper cervical lines and then subdivided down lineages: Palmer, then Grostic, then Gregory, or independent/other. Uncertain lineages are labeled with a question mark. Within each category, the techniques from Figure 1 are presented alphabetically.
Full Spine Line
ASBE-Full Spine Line/Independent?
Ronald J Aragona, DC, PhD, started the Aragona Spinal Biomechanical Engineering Research Laboratories, Inc, in the mid-1970s after attending New York Chiropractic College.41 This work led Aragona to found the technique ASBE.41 The ASBE seminars later fell under the purview of Karen M Borges, DC, and David Borges, DC, at a private chiropractic clinic, Borges Chiropractic. The ASBE Web site contained a link referring viewers to the Borges site; the ASBE Web site had limited information of 3 pages of text with a logo.41 Although no direct references to the teachings of BJ Palmer were found, the ASBE approach to research of “validating the necessity for chiropractic spinal adjustments”41 was similar to Palmer’s stated use for radiography.7 Patients of this technique were reported to receive the same extensive series of radiographs, including posttreatment images to demonstrate the reduction of vertebral subluxations.41 Based upon the available information, it was uncertain as to whether or not this system was an entire technique; the Web site noted that “ASBE works in addition to all current adjusting protocols.”41 This technique was included in this study because it claimed a unique system of analysis of subluxations on radiographs and used reduction of subluxations as the patient outcome measure.
CBP-Full Spine Line and Grostic Line Via Pettibon
Chiropractic BioPhysics, a full spine system, was influenced by Burl Pettibon. Pettibon reportedly derived his ideas from Grostic, who was a student of BJ Palmer. Born in 1946, Don Harrison graduated from Western States Chiropractic College in Portland, OR, in 1979. He then reported a desire to concentrate on spinal research but decided on an alternative route to this knowledge, earning a Master of Science in Engineering in Mechanical Engineering and then a PhD in Applied Mathematics, both from the University of Alabama.42
Harrison credited his brother Glenn, also a doctor of chiropractic, as a founding member and developer of the technique. Together, they took seminars in Pettibon. Don Harrison found shortcomings with the mechanistic descriptions provided in the seminars but was impressed with the technique nonetheless and told this to the technique’s founder, Burl Pettibon. Pettibon hired him to help develop materials for and to teach the seminars, and to work in his Washington state clinic.33
Harrison developed his own system, reducing the number of radiographs taken. He noted appreciation expressed by his patients for the decreased exposure but still included posttreatment films.33 Harrison, at the suggestion of his brother Glenn, expanded his biomechanical ideas to the thoracic spine; and later, Sang Molyneux, who eventually became his wife, suggested applying it to the pelvis.33 Although based on Pettibon’s upper cervical ideas, CBP became a full spine technique.
Gonstead-Full Spine Line
Clarence Gonstead was said to have developed rheumatoid arthritis in young adulthood, and university doctors were ineffectual in their treatments. His pain was apparently alleviated by a series of chiropractic adjustments, allowing him to walk again.43 He graduated from the Palmer School of Chiropractic in 1923 and moved to Mount Horeb, WI, where he opened his practice.
Within a few years, he theorized a variant of the early chiropractic idea of a bone causing pressure on a nerve. He proposed that the intervertebral disk was the cause of the pressure resulting in nerve interference.43 Gonstead believed that the spinal range from the base of the skull to the fifth cervical vertebra and below the fifth lumbar vertebra governed the parasympathetic nervous system and that the remainder of the spine controlled the sympathetic nervous system.44 The outcome measure he used was realignment of the vertebral body with the disk. To measure this, full spine radiographs were used.44 After practicing for more than 50 years,43,20 Gonstead sold his clinic and seminar company, which claimed to teach the materials “…in their original format.…”43
Logan Basic-Full Spine Line Via Universal Chiropractic College and Aquarian Age Healing
At first, the Logan Basic Technique appeared to have arisen from an independent chiropractic line; but its underlying ideas showed the foundations of Palmer chiropractic theory. It also seemed to draw heavily from Aquarian Age Healing.45 Hugh B Logan (1881-1944) and his son Vinton F Logan (1905-1961) both graduated from Universal Chiropractic College in 1915 and 1926, respectively.32 The Universal Chiropractic College was started by a group of former Palmer faculty who rebelled when BJ Palmer introduced radiography to the curriculum.46
Hugh Logan was reportedly highly opinionated; and his obstinacy made him enemies in California, where he had set up practice in 1927. His license to practice was revoked, so he began teaching Aquarian Age Healing. During this time, he developed his own version of chiropractic but was forced to defend himself against several lawsuits from the founders of Aquarian Age Healing for purportedly stealing their ideas. The treatment methods of the 2 techniques bore strong resemblance to each other, focusing on perceived biomechanical imbalances in the pelvis. However, Logan Basic incorporated radiographic analysis. He and his son traveled the country for several years giving seminars on “Basic Technique.” Eventually, they moved back to the Midwest and founded Logan College of Chiropractic in St Louis, MO, in 1935.45
Warren L Sausser credits Logan’s method as the inspiration behind his development of the 14×36–inch (35×91–cm) upright, full-spine radiograph.47 Although the Logan system used radiography prior to this,48 in 1934, Hugh Logan advocated this particular method of radiography for his system in a speech at the annual convention of the National Chiropractic Association.49
The original Textbook of Logan Basic Methods (1950)50 stated that full-spine radiographs should always be obtained before adjusting a patient and that, although periodic follow-up images were good for convincing the patient of the benefits of chiropractic care, they were not required. Before and after plates of images were provided with text relating cures of such ailments as asthma, constipation, and appendicitis.50 A recent edition of the Textbook (2006) indicated that patients should receive 2 frontally oriented full spine views as well as a lateral full spine view.51
Pierce-Stillwagon-Full Spine Line
No official Web site for this technique could be found, possibly because the Pierce and Stillwagon descendants split. This technique was started by Walter “Vern” Pierce, a 1955 Palmer graduate,52 and Glenn Stillwagon53 a 1956 Palmer graduate.25 Pierce had a desire to help people but disliked the medical model; his uncle was a chiropractor, which helped him decide to become one himself.52 Stillwagon was reported to have entered the profession because “A chiropractor helped me with a health problem.”32
Pierce started his career concentrating on the upper cervical spine. Later, he was influenced by Logan Basic technique and expanded his methods to include the entire spine.52 In the late 1970s and into the 1980s, Pierce and Stillwagon lectured together and founded their system.54 The overall technique was described as being very similar to Thompson but with greater emphasis on radiography.25 They adopted radiographic stress views, videofluoroscopy, palpation methods, and thermography in addition to plain radiographs.25 According to Cooperstein and Gleberzon, recently, the Stillwagon component has altered the system by deemphasizing the radiographic component.25 However, the Web site that they cited for this information (ie, www.stillwagon.com) did not seem to exist. A Web site for the Pierce system was found, and it described itself in traditional chiropractic terms.55 The Web site also asserted that practitioners of the Pierce system save lives and that spines they treat often exhibit rapid and complete “corrections” on radiographs, for which they give thanks to Innate.56
Spinal Stressology-Full Spine Line
Started by Lowell Ward and continued by his son Stephen Ward, Spinal Stressology used radiographic assessment of spinal alignment to determine emotional states of the patient.57 The elder Ward decided to become a chiropractor because of personal experience as a patient, and he graduated from Palmer College in 1960.32
Working with Clint Fulkerson, PhD, who was an aerospace engineer, they developed a method to measure and analyze the progression of spinal distortions.58 Ward incorporated Selye’s theory of stress response (alarm, resistance, and exhaustion) to devise a biomechanical-emotional correlation.58 Stephen Ward specialized in using radiographic methods to determine the postural origins of conditions such as emotional disturbances, including suicidal thoughts,59 neuromuscular diseases, immune compromise, and learning disabilities.58 The radiographic procedure was extensive and included standing and seated front-view and side-view full-spine radiographs58 and also used posttreatment images.59 They reportedly performed these views even on wheelchair-bound children.58
Upper Cervical Systems
Palmer Upper Cervical Specific/HIO/Toggle Recoil
The original upper cervical technique was known as Palmer Upper Cervical Specific but has also been referred to as Toggle Recoil or Hole-in-One.26,60 The term Hole-in-One referred to the “hole” of the Atlas ring holding “one” of the dens of the Axis, and BJ Palmer’s adjusting method during this phase was called Toggle Recoil.26 The names Palmer Upper Cervical Specific and Hole-in-One seemed to be historical for the most part. In the modern iteration at the Palmer School of Chiropractic, the class that taught this system was called Toggle Recoil rather than HIO or Palmer Upper Cervical Specific.61 In Chiropractic Spinography and The Subluxation Specific The Adjustment Specific (1934), it was notable that BJ Palmer did not advocate posttreatment radiographs.1,26 His outcome measure was improved health of the patient, as was reported in his summary of 5000 cases.26 In this monograph, he provided some before-and-after radiographs; but in his description of how to handle a chiropractic case, he did not include postadjustment imaging.26 In The Science of Chiropractic (1920), there was no mention of spinography or x-ray.4
AUCB-Palmer Upper Cervical Line
Applied Upper Cervical Biomechanics falls under the purview of the International Upper Cervical Chiropractic Association, which was founded in 1993.62 The system credits BJ Palmer’s “15 years of unprecedented research” as the basis for its existence and that the radiographic analysis is modified from BJ Palmer’s methods.63 This system states that the technique affects “global body function”62 in patients and that their radiographic subluxation analysis and treatment allow benefits to conditions like cortical blindness, epilepsy, autism, and asthma.62 The main outcome measure is thermographic analysis.64
Duff Method of Analysis-Palmer Upper Cervical Line
Richard A Duff graduated from Palmer College of Chiropractic in 1989 and took over for his father, Stephen A Duff, who invented the system in the 1970s.65,66 The technique stated that it used “specific x-ray views” as well as thermographs and other procedures to evaluate the alignment of the upper cervical vertebrae,66 removing subluxations to prevent disease and correct dysfunction of the body.67 The goal of removing vertebral subluxations implies the use of posttreatment radiographs; however, the published materials from this technique did not include this explicitly.
Grostic-Palmer Upper Cervical Line
John Francis Grostic was influential in the subluxation-based, upper cervical spine–focused chiropractic community. Born in 1907, he contracted Hodgkin’s lymphoma at age 22 and was told he had 2 years to live. He visited a chiropractor, who treated him several times and then referred him to BJ Palmer. Grostic traveled from Michigan to Palmer’s school in Davenport for what is reported to be Palmer’s HIO technique, although Palmer taught full spine adjusting until 1934. Grostic appeared to have recovered fully within weeks of receiving care at the Palmer clinic and shortly thereafter decided to enroll in the Palmer School of Chiropractic, graduating in 1933.68
While there, he reportedly “became infatuated with x-ray”; and upon returning to Michigan, he opened a practice and acquired x-ray equipment.68 One day, he was hit in the neck by a heavy x-ray tube, which apparently caused a relapse of his Hodgkin’s symptoms; this time, he was given only 2 weeks to live.68 He again boarded a train to see BJ and was restored after a single adjustment.68 These treatments38 seemed to solidify Grostic’s belief, although he continued to have health issues throughout his life. “He never questioned the principle of chiropractic, only its application.”68
In 1936, Grostic entered a period of more systematic clinical observation, radiographing his patients both before and after each adjustment, noting perceived changes in the films and building some equipment to aid him in these endeavours.68 Although a strong supporter of BJ Palmer,68 Grostic believed that he could improve upon those techniques. By 1939, he was giving seminars on his own methods.68 In the mid-1940s, he commissioned a man named Travis Utterback to develop various devices to standardize the radiography and analysis of patients, including head clamps, a rotating chair, x-ray beam filters, and a “diarticulometer template” for subluxation analysis on the radiographs to aid his efforts.68
Grostic became a fastidious teacher of his own system, requiring practitioners to send in radiographs of their patients, which he would personally scrutinize, before they would be allowed to take an advanced seminar in his methods.68 Eventually, he required a philosophy questionnaire from each prospective seminar attendee; and those that did not stay true to his definition of chiropractic were not allowed to attend.68
From the 1940s through the 1960s, Grostic’s main collaborator was Ralph Gregory, a 1939 graduate of the Palmer School, although there were separations and reconciliations along the way.68 In 1966, Gregory went on to develop the NUCCA.69 Grostic died in 1964; but along the way, he influenced several other subluxation-based practitioners who developed their own radiographic analysis systems. Upon his demise, Grostic followers generally split into 2 groups, one following Grostic’s principles and one following Ralph Gregory’s. Grostic’s group included Roy Sweat (Orthospinology then Atlas Orthogonal), Burl Pettibon (Pettibon), William Blair (Blair), and Don Harrison (CBP).68
The technique prided itself on its constancy, never straying from the ideas developed by the originator: “The x-ray analysis is the real core of the procedure and is the one area that has remained constant over the last 30 years.”21 Seven of 21 chapters of the official textbook for this technique pertained to radiography.68 The clinical outcome measure Grostic used was postadjustment radiographic findings.68 There seemed to be no clear delineation between Orthospinology and the Grostic method according to the public documents; the descriptions of the techniques are blended in the official textbook.
Kale-Palmer Upper Cervical Line Via Sherman
Michael U Kale was a graduate of the Palmer School and credited BJ Palmer’s HIO as the inspiration for his technique, tracing the lineage from BJ, through Lyle Sherman, also a chiropractor. According to Kale’s son BJ Kale, Sherman was the Assistant Director of the BJ Palmer Research Center from 1935 to 1951,70 although another source states the years as 1942-195571; and he was the inspiration for the name of Sherman College of Chiropractic.72 Kale claimed to have been sick for 18 years and, after having seen many doctors, stated that he was finally cured by a chiropractor. Because of this experience, he decided to become a chiropractor.32 After attending Palmer, he interned for Lyle Sherman in the 1960s; the Kale technique’s online promotional materials made many references to this second degree of separation and its importance to the purity of the Kale Method.73 As stated on the Kale Web site, “He did not overstep Dr. Sherman’s words and wisdom. He Trusted!”70
The Knee Chest Upper Cervical Society stated that they had “central influence” from Michael Kale and credited Kale with bringing upper cervical techniques back from the brink of extinction in the 1980s.74 Particularly strong belief was noted in Kale’s methods: “Mild to moderate [spinal] malfunction results in sickness and disease, while extreme malfunction results in DEATH!!” [emphasis original]39 This site also claimed that the technique will benefit or cure conditions like Parkinson disease, AIDS, paralysis, and sight and hearing disorders.75 They noted that because the spinal misalignments that cause these diseases are very slight, on the order of millimeters, they used very precise x-ray equipment.76 According to their sources, they also note inadequacy in standard x-ray machines for this purpose, using a laser-aligned x-ray instrument.77 The outcome measure used was thermographic imaging to ascertain nervous system interference.76
KCUCS-Palmer Upper Cervical Line Via Sherman
Knee Chest Upper Cervical Specific was founded in 2000 by Robert Kessinger, who graduated from Logan College of Chiropractic in 1988.78 The Web site reported that the first official KCUCS Seminar took place on 16 and 17 November 2001 and was led by Kessinger after he hosted a number of unofficial gatherings to discuss the “philosophy, science and art” of chiropractic.74 Kessinger trained under Michael U Kale in January 1991 and then went on foreign missions with Kale and taught Kale seminars.74 He subsequently studied Blair’s method of radiographic analysis and combined these methods with a modified subluxation theory, based on Grostic’s ideas, to form his own technique.79 He was assisted in these endeavors by 2 other Kale practitioners, Henri Dallies and Mike Anderson.74 Radiography demonstrated prime importance in this technique; the KCUCS blog made reference to a 6-week “x-ray bootcamp.”80 A YouTube video showed Kessinger demonstrating radiographic technique, including posttreatment radiographs.81
On its Web site, KCUCS deferred to BJ Palmer’s clinical observations from 1935 to 1954 for the clinical rationale and presented 4 case reports of KCUCS successes, 1 of which was published in a scientific journal.82 Although heavily influenced by Kale and Grostic and Blair, and because of the references to Palmer for the basis of their methods, the technique was considered here as having 1/2/3 degrees of separation from Palmer’s HIO.
Mears-Palmer Upper Cervical Line
Donald B Mears, Sr, graduated from the Palmer School in 1927, having been drawn to Davenport from his home in Vermont by hearing lectures on chiropractic broadcast on WOC radio.32 A contemporary of William Blair, he searched beyond the teachings of BJ Palmer, having become dissatisfied with the inconsistency of the responses of his patients to his adjustments.83 He changed the focus of his radiographic interpretation slightly and maintained radiographically demonstrated subluxation reduction as the goal.83
Sutter Specific Atlas Correction-Palmer Upper Cervical Line
Max Sutter graduated from the Palmer School in March 1925 and moved to California to practice.23 He had originally been practicing full spine technique but abandoned that in 1936 in favor of concentration on the upper cervical area.23 In 1938, Sutter began to use his clinical observations to embark on the process of developing his own version of the technique.23 In 1940, he named the system Specific Atlas Correction.84 He put his theories forth in his treatise The Master Key to Health, which was praised by BJ in a Foreword to the 20-page pamphlet.84 The radiographic interpretation was described as a combination of standard HIO and elements that Sutter invented.23 There was no reference in these materials related to posttreatment radiography, although Sutter stressed realignment of the atlas vertebra as the goal of a chiropractor.23
Zimmerman-Palmer Upper Cervical Line
Arden D Zimmerman may be best remembered for having invented the first machine to deliver a chiropractic adjustment in application of the principles of BJ Palmer’s HIO system. However, he also invented his own complete technique system by modifying Palmer’s ideas.85 Before becoming a chiropractor, Zimmerman graduated from Stanford University with a degree in engineering in 1931.85 He claimed that after being hit in the back of the head at 9 years of age, he developed Addison disease.85 His mother took him to different medical practitioners, who failed to give long-term results.85 In 1937, he visited the Palmer clinic for care85; and later that year, he was well enough to enroll in the Palmer School.85 He credited the relief of nerve pressure from his upper cervical spine with his return to health and became licensed to practice in California in August 1939. He began studying radiographs of the upper cervical spine in more detail.85 By 1943, Zimmerman had developed his own system for taking radiographs including stereoscopy, using the spinal misalignments he found to guide his treatments.85 He wrote, “All it takes to restore the flow of energy to the sick body is ONE accurate adjustment.” [emphasis original]86 He stated that the purpose of a chiropractor was to set vertebrae back in alignment, not to treat illness.85 This might be implied to mean that he may have used posttreatment radiographs, although no explicit information on this was found. This technique never became widely disseminated; in its pure form, it was apparently only practiced in 14 offices between 1948 and 1996.85 Although criticized by BJ Palmer for his use of a machine to perform spinal adjustments instead of adjustments by hand, Zimmerman remained loyal to Palmer throughout his lifetime; and he bequeathed all his professional materials, devices, and papers to the Palmer College of Chiropractic.85
Grostic Upper Cervical Line
Atlas Orthogonality-Grostic Line
One of the original Grostic descendants, Roy Sweat, was schooled by BJ Palmer and attended his first Grostic seminar in 1952.25 He built his theories on Grostic’s work, emphasizing the importance of the upper cervical spine and its potential subluxations in relation to the cause of disease. He also helped found the Society of Chiropractic Orthospinology.18 In 1981, he founded his own technique, Atlas Orthogonality.87 According to Sweat, Grostic introduced posttreatment radiographs to the profession in 194618; but AA Wernsing advocated them in 1941 in his text,25 and Sweat required them as part of Atlas Orthogonality.18
Blair-Grostic Line
William George Blair claimed to have been cured of bronchial asthma by a chiropractor who practiced an upper cervical technique. This experience inspired him to attend the Palmer School of Chiropractic,88 from which he graduated in 1949.68 He chose the Palmer School because it was the alma mater of Leon Halsted from El Paso, TX, the man who Blair credits with helping him overcome his health difficulties.68 After graduating, he moved from Iowa to Texas, with the idea of changing the upper cervical radiographic analysis he was taught.68 Halsted had been attending Grostic seminars and likely encouraged Blair to study Grostic’s methods, although apparently Blair never formally attended any Grostic classes.68 In 1951, Blair embarked on “Ten long months” to develop the "Blair Principle of Occipital-Alanto Misalignment.”88 The rationale behind this technique included Blair’s perception that anatomical “malformations” were the rule rather than the exception, leading to erroneous subluxation descriptions and therefore incorrect adjustment applications.88 Differentiating the malformations from the subluxations resulted in many radiographic images being necessary for each patient: stereo views, meaning 3 views, each from 2 slightly different angles as well as “the usual flat views.”88 This procedure became considered “the hallmark of the Blair Upper Cervical Technique.”89 Posttreatment radiography was not considered routine, the technique instead opting for thermography as a standard outcome measure.89
(Society of Chiropractic) Orthospinology-Grostic Line
The Society of Chiropractic Orthospinology was founded in 1977, based on the work of John F. Grostic. The first President was Roy Sweat, who later started his own technique, Atlas Orthogonality. Other members of the original Board of Directors came from the group formed to continue disseminating Grostic’s techniques after his death, Grostic Chiropractic Presentations, Inc.68 As noted in the section on Grostic, there was no clear distinction found between Grostic and Orthospinology; the official textbook for both is the one book entitled Orthospinology Procedures: An Evidence-Based Approach to Spinal Care Based on the John F Grostic Model and Procedure.21 The system used Grostic radiographic analysis90 including posttreatment images.21 The outcome measures were not patient wellness or improved function, but rather changes demonstrated by radiographic and postural analysis.36
Pettibon-Grostic Line Later Joining Full Spine
Burl Pettibon graduated in 1956 from Cleveland Chiropractic College after being treated by a chiropractor for sequelae of a fracture of his spine due to a football incident.32 The co-manager of the system, Sharon Freese-Pettibon, attributed changes in her health, including resolution of a bleeding ulcer and recovery from trauma-induced paralysis, to treatment by Burl Pettibon, who later became her husband.91
Burl Pettibon took 1 Grostic class in either 195625 or 195968 and eventually developed his own technique. The Orthospinology textbook noted similarity between his cervical x-ray analysis and that of the Grostic procedure.68 Pettibon collaborated with others like Don Harrison and Vern Pierce; built a variety of tools and devices for radiography and radiographic subluxation analysis; and taught at Palmer, Life, Logan, and the Northern California Colleges of Chiropractic.32 This technique advocated 7 or more views of the spine as routine for patients.22 The radiographic analysis included over 41 lines and 23 angles to specifically locate the displaced vertebra.92 Although improvements in health of patients were attributed to the system, this was not the outcome measure, but rather perceived changes on the radiographs.22
Upper Cervical Orthogonal/Cowin-Grostic Line
Developed in Australia by Robert Cowin and Kathleen Bras, this was a variation of upper cervical orthogonal19 and was therefore placed in the Grostic line. This technique claimed extreme precision in radiographic interpretation of the bones of the spine, noting measurements as small as 0.75° or 28 thousandths of an inch or 0.7 mm.19 There is no evidence to support this level of accuracy. The chief outcome measure for this technique is reportedly the perceived change of vertebral position on a second set of radiographs.19
Gregory Upper Cervical Line
Advanced Orthogonal-Grostic and Gregory Lines
This technique was started in 2001 by G Stanford Pierce and his son G Stanford Pierce, Jr, based on the father’s work with other upper cervical techniques earlier in his career.93 This technique reports to focus on finding subluxations using “3-D x-ray analysis.” This seemed to mean analysis based on 3 different views of the upper cervical spine, not 3-dimensional simulated radiographic visualization.93 In the 1960s, the elder Pierce attended Grostic seminars and then worked with Roy Sweat in developing the Atlas Orthogonality technique, eventually teaching seminars in those methods.93 The Advanced Orthogonal Web site also acknowledged the influence of Ralph Gregory, founder of NUCCA and Grostic collaborator, and recognized the lineage of all upper cervical techniques as traceable to BJ Palmer and his HIO technique.93 According to their documents, this technique claimed the ability to measure misalignments as small as 1/100th of a degree.94 The stated goal of the technique was subluxation correction,94 although they claimed effects for this including reversal of degeneration,95 and a wide variety of systemic and neurological conditions.96 Posttreatment radiographs were reportedly required.97
NUCCA-Gregory Line
Ralph R Gregory, a 1939 graduate of the Palmer School,68 met John Francis Grostic in 1941 and formed an alliance dedicated to upper cervical methods.68 Grostic had apparently been suffering from Hodgkin disease and received a restorative treatment from Gregory at this time.69 The Grostic literature criticized Gregory for using full spine adjusting early in his career but acknowledged his transformation into a skilled practitioner and that Grostic allowed Gregory to treat him.68 Gregory’s interest in the upper cervical spine began at Palmer, but he also noted direct influence by AA Wernsing's book The Atlas Specific.69 Gregory and Grostic’s main collaboration was between 1941 and 1946, when they undertook systematic observations of their radiographic methods and outcomes.69
Following Grostic’s death in 1964, Gregory was initially reluctant to continue teaching seminars and wanted to concentrate on modifying his method. However, he eventually relented; the informal organization NUCCA was created in April 1966.69 National Upper Cervical Chiropractic Association hired Harry Long, PhD, to be the first research director.69 In 1971, the group decided to form a subgroup specifically for research, which they called the National Upper Cervical Chiropractic Research Association, disseminating their findings through a newsletter called The Monograph.69 Subsequently, they developed new methods of radiographic analysis that have been incorporated into the system.69,98 The National Upper Cervical Chiropractic Research Association changed its name to the Upper Cervical Research Foundation.98 Their documents asserted that misalignments of less than 0.75° can cause systemic disorders.99,100 National Upper Cervical Chiropractic Association declared its mission as maximizing human health potential by reducing misalignments of the atlas.101 The standard of care document published on NUCCA’s Web site stated that the patient’s progress is monitored with radiographic analysis and that the least accurate outcomes assessment is patient pain or symptoms.102
Spinal Orthopedic Neurological Advancement and Research-Gregory Line
Thomas R Elliott, Jr, president of SONAR Foundation, graduated from Palmer College and began practicing in 1972.103 Elliott claimed to be active in research103; however, there is no record of published research studies authored by him in PubMed. The system reported the supremacy of alignment of the cervical spine, stating that if the top cervical bone is out of place, the brain and body will degenerate and even render medication ineffective.104 Elliott started as an NUCCA practitioner, and SONAR used those procedures for taking and analyzing radiographs.68 Because Elliott attended the Palmer College of Chiropractic after BJ had died, his technique was considered 3 degrees separated from Palmer, with his radiographic methods arising from NUCCA.
Discussion
From the review of publicly available documents, the technique systems that use plain radiography for the detection or quantification of subluxations emphasized their differences, often acknowledging the foundation from a previous technique but incorporating changes to perceived inadequacies. Interestingly, they seem to be much more alike than they are different. These similarities are not only in their use of radiography but particularly if viewed from the broader perspective of diagnostic imaging in health care. BJ Palmer espoused the idea that radiography was to be used for the detection of chiropractic subluxations and nothing else, stating, “The original Chiropractic purpose was not to use the X-Ray for therapeutic purposes, to ascertain normal or abnormal tissues, the character of a fracture or whether there was renal calculi [sic] or a bullet in the body. We had already settled how a cure occurred; we did not care much about pathological plates.”1 This concept seems to have continued down the lineage by many of the subsequent techniques. This is not to say that modern practitioners of any of these systems did not also scrutinize their images for pathology, but little mention of pathology analysis was found while examining their official publications. The vast majority of references to radiographic imaging found on the Web sites and in public documents were in the context of subluxation detection only (Appendix 2). The majority of the techniques also acknowledged a clear lineage in their histories and development. This implies a sort of family and reinforces their similarities. These similarities placed them on a separate branch of the tree from the technique systems and practitioners that did not include radiography for subluxation detection; that did not claim to have broad, systemic effects with their methods105,106; and who advocated radiography and other diagnostic imaging technology in the mainstream way to diagnose pathology.107–111
Approximately 88% of the upper cervical techniques evaluated in this study traced their origin to a time when the BJ Palmer was teaching this method at his school, and all the full spine techniques originated before or after this phase. Palmer was arguably the most vociferous and well-known chiropractor of his time. This may have resulted in his influence beyond his immediate circle of followers, possibly influencing the development of technique systems throughout the profession.
Many of the systems reviewed in this study included in their radiographic paradigm subluxation reduction/improved spinal position as the sole or main outcome measure for their patients but did not include in their materials information about reduced pain, increased activities of daily living, or any other subjective or objective patient-based measures. This is not to say that individual practitioners using those systems do not use clinical outcome measures. This is only to mean that these outcomes were not included in the publicly available documents representing the techniques. Several of the techniques actively disclaimed treating symptoms or health conditions but seemed to take credit if positive effects were noted during a course of care. For example, on one Web site, it stated, “Orthogonally-based upper cervical care is not a treatment for conditions or diseases, however, this subluxation-centered care has been shown to have an associative effect on various conditions.”21 Another says, “The procedure cures nothing, but it allows the body to cure itself. It restores body balance and proper nerve flow so that organs, limbs, and tissues can resume normal functioning. This is why we see so many different conditions with no apparent relationship responding to the SONAR procedure.”112 And yet another states, “We are saying that we make no cures and can give no guarantees.…”59 BJ Palmer did not always advocate the use of posttreatment radiography. However, it seems reasonable that at least some of the influence for repeated films may have come from Palmer because he wrote at length material that could be interpreted as advocating this practice.
The techniques included in this study seem to claim broad health benefits from their systems. BJ Palmer may have had direct or indirect influence on this paradigm. In 1934, BJ Palmer wrote, “Disease, per se, can be and should be ignored. Symptoms, pathologies, diagnoses, histories of effects could be discounted even tho [sic] not denied… dis-ease is simple, not complex… dis-ease was [sic] single, not multiple, one thing [subluxation], not thousands.”26 The monism of vertebral subluxation as the cause of suboptimal health would seem to foster the idea that any useful outcome measure would focus on demonstrating the reduction of the misaligned vertebra. This is not representative of all chiropractors; there are many that judge the success of their methods by the health of patients, not perceived changes in osseous position.113,114 At present, little evidence exists for the broad systemic effects of chiropractic methods.105,106 In addition, Gleberzon115 in 2001 and Owens116 in 2002 found little evidence that links chiropractic radiographic measurements to clinical outcomes.
Fuller117 noted that chiropractic gained ground by publicly focusing on clinical outcomes and generally deemphasizing the metaphysical aspects in the foundation of the profession. Nonetheless, the writings examined in this study seemed to be based on early chiropractic theories or each technique’s particular variants of them, which carry metaphysical overtones. The techniques discussed here seemed to have been developed empirically, rather than through systematic, scientific investigation.21,68,43,70 The publicly available documents simply asserted that chiropractic subluxation was the primary cause of poor health and plain radiography was the method to find the subluxations. However, they provided no evidence to support these claims.
According to their publications, the majority of technique originators based their techniques on information from previous technique instructors. Using a method similar to philosophers, they built their methods, founding one theory upon another, rather than testing theories in controlled scientific studies and allowing scrutiny from the outside (Appendix 2). Many of these technique founders seemed to use radiography to interpret minute spinal asymmetries and perceived changes as evidence supporting broad assertions about health. This is similar to what BJ Palmer stated when he wrote that he bought an x-ray machine to “prove” subluxations.1 It may be that many of his chiropractic technique descendants also worked diligently in their efforts to demonstrate or quantify subluxations based upon an a priori assumption. None of the documents found for this study demonstrated evidence that the technique originators examined the underlying theory that a misaligned vertebra affected a nearby nerve, causing disease. In the documents reviewed, the mechanisms were not described, only the methods of finding the subluxations and the treatment of them. Interestingly, the words science and research continually appeared in the techniques’ publications.118 A trend in these techniques showed circular logic: the idea of subluxation supported the use of radiography, and radiography verified the existence of the subluxation, each component being necessary to the viability of the other.
Hildebrandt119 noted that chiropractic spinography at that time was a “somewhat provincial” procedure and had not received constructive scrutiny from the broad scientific communities of the health care professions. In an effort to rectify that situation, Hildebrandt published his book Chiropractic Spinography to expose a more complete record of those methods to the world outside chiropractic so that judgement could be rendered.119 He continued with a caution regarding overstatement of the status of chiropractic spinal radiographic procedures by saying:
“Instead of developing spinographic procedures to evaluate biomechanical knowledge first evolved through unbiased research, they were generally attempting to develop or ‘tailor’ biomechanical knowledge to support the spinographic procedures they were already advocating… some concepts of spinal biomechanics were developed which were later difficult to reconcile with accepted knowledge of human anatomy and physiology. These concepts, in some cases, became so ingrained in certain elements of the profession that even today it is difficult to separate established fact from that which was arbitrarily accepted as established because it has been taught that way for so long.”119
Unfortunately, modesty of claims and critical inquiry to the deepest levels of the system (ie, examination of the existence of chiropractic subluxation as demonstrable on radiographs its mechanism of clinical relevance to the patient) were not found in any of the public documents of the systems examined in this article.
Another question raised in gathering the histories of the development of these techniques was their quantity. Twenty-three seems to be a great number of technique systems that were all similar in their methods and goals. Cooperstein and Gleberzon25 attributed the proliferation of chiropractic technique systems to dissatisfaction in the profession with the original Palmers’ (both DD’s and BJ’s) attitudes, behaviors, and proprietary methods.25 Certainly, infighting was rife in the early profession and continues today120; but this seems to be an incomplete explanation. A number of other factors have also been proposed, including the fact that chiropractic developed at the margin of health care, lack of market penetration, an economic advantage of retaining several techniques, the view of the chiropractor as a generalist, the mercantile bent of the founders, lack of knowledge regarding research methods, the quest for nerve interference, the allure of name-brand techniques, and the glass house effect, that is, the fact that few of the techniques had much substance in evidence.121 Nelson122 noted that a proliferation of contradictory techniques was inevitable given the cognitive and epistemological methods used by technique developers.
This current study found a trend in the writings that the inspiration to become a chiropractor or to start a technique came from a powerful personal experience with chiropractic treatment, typically as a patient. Emotions can be potential motivators of information seeking.123 More than one-third of the technique originators credited chiropractic for personal health benefits and reported being moved to investigate and alter the techniques that had been applied to them. It seems reasonable that the personal health improvements attributed to chiropractic treatment could have been motivational for some of the eventual technique originators to gather further information within the chiropractic realm, as it had been revealed to them. This may be another link joining these techniques.
Around the 1940s, a shift occurred in chiropractic. Part of the profession moved away from the use of radiography for subluxation detection and began using it primarily as a diagnostic tool for pathology, similar to the medical profession.124–126
Limitations
It is possible that some techniques were not included in this study. They could have been missed if they no longer exist, had very small numbers of practitioners, and/or had no Internet presence. This article only sampled the public statements from techniques’ official Web sites, papers, and textbooks; nuances and variations would likely be revealed by interviews with the spokespeople for the techniques for those techniques that are not defunct. Because Web sites are sometimes created or edited by external individuals or companies conversant with information technology but not necessarily the content of the sites they design, they may not always accurately reflect information presented to them for publication. Differences would also likely be found if individual practitioners were interviewed on how they practically applied the techniques in their own practices, rather than just how the techniques officially advocate use of their system. This study was limited to only those documents that the technique endorsed or provided publicly. It is possible that there are other available documents that contain additional information—such as descriptions of mechanisms, scientific foundations, or other information—that the author was not able to find in the search. As these types of public documents (eg, Web site for a technique system) are typically not intended for scientific purposes, it may not be appropriate to judge the technique solely on the available content. It is possible that scientific evidence for these techniques is published in other sources.
Future Studies
The history of the development of the remaining branch of the chiropractic radiology family, that is, those practitioners that adopted the technology to assist with pathological diagnosis rather than chiropractic subluxation detection, should be studied to round out investigation of the development of diagnostic imaging in the profession. In examining the writings of those included in the current study, many of the technique originators referenced other belief systems as part of their methods. This includes mention of terms of spiritual nature, such as God, a god, a universal intelligence, or a vital force. For future studies, the theme of belief, rather than skepticism, in chiropractic technique systems that advocate radiography for subluxation detection also warrants further investigation. The current study revealed a trend for technique originators to be motivated from strong personal health experiences. It may be useful to study the motivations for becoming a chiropractor or for originating a chiropractic technique that does not involve radiography for subluxation detection to determine how these groups may differ and what sort of expectations are present when embarking on a career in chiropractic. Some of the findings reported in this study denoted an epistemology of appeal-to-authority, advocating belief in the basic paradigm of predecessors, that is, that vertebral misalignments/subluxations are quantifiable on plain radiography, rather than scientific skepticism. Future studies should focus on what scientific evidence each of the techniques use to support their health-related claims. Findings from the current study evoke questions about the fulfillment of all 3 components of the fiduciary relationship to patients,127 particularly the duty of loyalty, that is, placing the interests of the patient above those of the practitioner. Further evaluation of these factors should be completed in future studies.
Conclusions
The evaluation of public documents shows that chiropractic technique systems that advocate radiography for subluxation misalignment detection are closely related by descent, by claims of broad health effects from chiropractic subluxation, and by radiographic paradigm.
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.
Appendix 1. Statements From Publicly Obtained Sources About the Broad Health Effects of Osseous Misalignment From Each of the Techniques
Advanced Orthogonal
“By God’s design, the balanced function of the brain and nervous system is essential to the integrity of health. Our focus is on identifying and correcting the structural causes of this dysfunction, to restore and maintain the health and well-being of all those whom we serve. Too many people are suffering from conditions that are impeding their ability to live fruitful and productive lives.”35
Applied Spinal Biomechanical Engineering
“A chiropractic doctor detects and corrects these spinal misalignments (vertebral subluxation causing nerve interference), restoring normal nerve impulses to the body allowing the body's own innate healing capabilities to function optimally.”37
Applied Upper Cervical Biomechanics
“The foundation of the chiropractic profession stands upon the premise that health and disease are nervous system dependent,” “How can I transcend the practice of pain management to the practice of true health care? We all have been told that chiropractic can effect [sic] the body as a whole, but where is this practice? These are the questions our association is striving to provide objective answers to.”64
“If you are ready for a practice that delivers consistent broad-scope health care, then welcome to the IUCCA [International Upper Cervical Chiropractic Association].”64
Atlas Orthogonality
“When the atlas bone is properly aligned, that is in the orthogonal—or neutral—position, the rest of the spinal vertebra [sic] come into better alignment allowing the body to heal itself.”18
Blair
“The nervous system controls and regulates all parts and functions in the body. When there is nerve interference (subluxation) your body loses the ability to properly self regulate and heal itself. The result can be pain and illness. Blair upper cervical care is often the key to people regaining and maintaining good health.”128
Chiropractic BioPhysics
“[Our goal is to] correct human spines and alleviate human suffering.”33
Cowin Upper Cervical Orthogonal
“Our procedures are based on the traditional chiropractic concept of vertebral subluxation.”129
Duff
“Most of this problem (Subluxation) exists at the base of the skull or known as the upper cervical region of the spine. It is at this level of the spine that can produce many health problems.”67
Gonstead
“…compressed nerves often become inflamed and impede the proper transmission of impulses to the section of the body controlled by these nerves. A seemingly endless list of ailments and pain may be brought about by these subluxations.”130
Grostic
“Orthogonally-based upper cervical care is not a treatment for conditions or diseases, however, this subluxation-centered care has been shown to have an associative effect on various conditions.”21
Kale
“When one or both of the top two bones (Atlas and Axis) misalign, creating pressure on the ‘Brain Stem’ and causes an interference of nerve flow to all parts of the body. This is what causes the body organs and tissues to malfunction, thus causing disease.”76
“Mild to moderate [spinal] malfunction results in sickness and disease, while extreme malfunction results in DEATH!!” [emphasis original]39
Knee Chest Upper Cervical Specific
“Upper Cervical Specific Chiropractic Care [emphasis original] focuses on removing nerve irritation to restore communication between the brain and the body. Restoring function at the level of the brainstem and upper cervical spine (the control center of the body) is essential so that the body may heal itself and have optimal vitality. With the nervous system functioning at 100% the body has the potential to heal itself from even the most complex of ailments.”76
Logan Basic
“Displacement of the sacrum is the cause of disease.”131
Mears
“The Mears Technique is a specific upper cervical system of X-ray analysis and adjustment that carries on where the H.I.O. concept ends.”83
National Upper Cervical Chiropractic Association
“The postural rebalancing created by the upper cervical adjustment allows for the body to have less gravitational stress and therefore the person can direct that now unused energy to self-healing, maintenance and thinking.”132
Orthospinology
“Since Orthospinology is essentially inseparable from Grostic; the same concepts apply.”68
Palmer Upper Cervical Specific (Hole-in-One)
“That the sunnum bonum of all life and death, health or disease issues pivoted around a study of the correct or incorrect position of vertebrae.”7
Pettibon
“The purpose of the chiropractic adjustment is to work “with” the innate intelligence of the body to produce a predictable response. Our specific adjusting forces are designed to cause innate to react positively with its environment. An adjustment must be a positive, constructive force that causes the body to predictably react to its environment, correcting the spine so the nerves can function normally resulting in health to be expressed optimally.”92
Pierce Results
“By correcting subluxations more effectively, Dr. Pierce began to see many things heal faster, even spines that never changed on x-ray were now exhibiting complete corrections in minutes! (Thanks to Innate!)”56
Spinal Orthopaedic Neurological Advancement and Research
“[The] result of a misaligned atlas is the restriction or distortion of critical messages at the brainstem and upper-spinal cord, disrupting the brain's communication. Every cell, organ, or tissue that is not receiving adequate nerve energy and communication from the brain will suffer and degenerate.”104
Spinal Stressology
“When you put subluxations in terms of a disorganized system and the treatment of subluxations as you are trying to release that pattern of disorganization and bring it back into a reorganized format, where it can recover and create its own homeostasis…”59
Sutter
“That disease is caused by an interference with the Creative Intelligence that wills normality within the body. That such interference is caused by obstruction of nerve impulse flow from the brain to the body due to a subluxated spinal vertebra. That this Chiropractic principle is the greatest boon to suffering humanity and supplies a need for which there is no substitute.”84
Zimmerman
“When pressure is removed from the spinal cord, the effect is the same as turning on the electric power to a light bulb. Without the electricity the lamp does not produce any light. When the patient’s body is deprived of energy by a nerve pressure, anything can go wrong and death may occur. All it takes to restore the flow of energy to the sick body is ONE accurate adjustment.” [emphasis original]86
Appendix 2. Findings From Publicly Available Documents on the Paradigm of Radiography for Each Technique
Advanced Orthogonal
“This assessment can only be obtained by looking at very precise x-rays from all 3 dimensions. The views are left (sagittal or side), center (nasium or front) and right taken from above (vertex).”133
“Digital x-ray analysis to measure misalignments to the 1/100th of a degree.”94
Applied Spinal Biomechanical Engineering (ASBE)
“ASBE utilizes very low radiation dosage static and dynamic spinal radiographs to help with objective pre-treatment and post-treatment diagnostic rational [sic] for the reduction of vertebral subluxations.…”41
“ASBE starts the analysis with the static weight bearing x-ray views. Then adds intersegmental bilateral lateral flexion biomechanical analysis.”41
Applied Upper Cervical Biomechanics (AUCB)
“Radiographic landmarks form the foundations of entire systems of analysis; hence their reliability is paramount to the accuracy of the evaluation.”134
Atlas Orthogonality
“The first step of the diagnosis is to determine the degree in which the atlas is misaligned. Very precise x-rays are taken which show the doctor exactly how the atlas is displaced. The x-rays taken are invaluable in making the most precise atlas correction which is as unique to the patient as their own fingerprint.”18
“One of the most important post adjustment steps are post x-rays, which are taken immediately after the initial treatments.… These three dimensional x-rays are taken and analyzed to verify that the best possible correction was rendered. The doctor may then show the patient the comparison between before and after x-rays. Post x-rays are an illustration of the exact change that has taken place because of the atlas orthogonal correction.”18
Blair
“This ‘blue print’ of your neck [created from the radiographs] allows the Blair chiropractor to deliver the adjustment that is exactly what your body needs.”128
“These x-rays are “the hallmark of the Blair Upper Cervical Technique.”89
Chiropractic BioPhysics
“CBP protocols require that the doctor must measure the displacements on spinal radiographs (segmental Subluxation). Both lateral-side view and anterior to posterior (AP) or frontal view CBP x-ray line drawing procedures [are necessary].”135
Cowin Upper Cervical Orthogonal
“Before a patient receives a first adjustment (treatment), we spend an hour or more analysing the X-rays.”19
“After the first ‘trial-adjustment’, we take two new X-rays and compare them with two of the three initial X-rays to find out what changes in vertebral position may have been achieved by this adjustment attempt. Getting the best adjustment, may require several 'trial-adjustments' over a number of visits.”19
“The other comparison X-ray in the series (sagittal plane natural lateral) is taken about 18 months later in the hope of finding evidence of improved posture. The chiropractors interpret this kind of improvement as resulting from the patient's new self-help activities over this time.”19
“Measurements “as small as 0.75 degrees (or, translated into linear measurements, each as small as 28 thousandths of an inch or 0.7 mm)”19
Duff
“Dr. Duff's speciality is in aligning the upper top two vertebrae Atlas Axis, C1 and C2 [sic] by using specific X-Ray views.”66
Gonstead
“…full-spine radiographs are taken in the standing, weight-bearing position to fully substantiate the examination findings.”20
Grostic
“The analysis of your x-ray views will reveal the exact degree of misalignment or imbalance. The mathematical measurements taken from your x-ray films give the doctor the correct formula to realign your spine.”21
Kale
“Three x-ray views are required to determine the subluxation of the Atlas (top cervical vertebra); they are AP open mouth, lateral (through C1), and base posterior.”136
Knee-Chest Upper Cervical Specific
“6 week “X-ray Bootcamp”137
“The misaligned segments are identified through the use of Digital Laser-aligned Radiography. Because the misalignment is very slight (measured in millimeters) it is very important that precise x-ray equipment is used.”76
Logan Basic
“Full spine radiography is required.”138
“Ten patterns of ‘distortion’ or what was considered abnormal spinal curvatures, which were marked on the radiographs.”25
Mears
“…more reliable [radiographic] points of reference to determine cervical distortion more accurately. This in turn led to the need to modify the adjusting procedure used in the H.I.O. technique.”83
National Upper Cervical Chiropractic Association
“NUCCA’s forte, even among the other upper cervical specific groups, has been to deal directly with postural imbalance. Indications when to and when not to intervene are dependent upon postural measurements. The direction of vectored manipulation, the how to intervene, is dependant [sic] on X-ray analysis and an understanding of biomechanics and patient abnormalities.”100
“NUCCA practitioners in general appear to have a more rigorous system with more pervasive and refined posture measurements, more meticulous X-ray procedures, and consistently better corrections as evidenced by its certification process and standards.”100
“Gregory was able to independently develop or improve upon both the accuracy and precision of all levels of analysis of the “Grostic” system by 1) development of a double-pivot-point system in X-ray analysis (1962)… 5) design of better film analytical instruments… 7) design and development of the Anatometer which reduces the need for X-rays (1978), 8) classification of C-1 subluxations into basic types(1980).…”100
Orthospinology
“Uses Grostic radiographic analysis90 including post treatment radiographs.”21
Palmer Upper Cervical Specific (HIO, Toggle Recoil)
“Radiographs are necessary to demonstrate subluxation.”1
“Post-treatment radiographs show correction.”26
Pettibon
“The Pettibon Rehabilitation System starts with an x-ray examination. Seven views of the spine are routinely taken, more if necessary.”22
“Pettibon x-ray analysis may involve over 41 lines and 23 angles to specifically locate the displaced vertebra.”92
“The initial set of examination x-rays are compared to x-rays taken during treatment to assess progress and ultimately to prove the treatment's success. Whether the x-rays are for diagnosis, testing, assessing progress, post-treatment evaluation and/or proof, patients are seated and the x-rays are always taken, marked, and measured the same way, every time.”22
Pierce Results
“By correcting subluxations more effectively… even spines that never changed on x-ray were now exhibiting complete corrections in minutes!”56
Spinal Orthopedic Neurological Advancement and Research
“SONAR was developed Thomas Elliott, Jr., D.C. who was a NUCCA practitioner. SONAR employs procedures for taking and analyzing x-rays.”68
“…linear and torque forces in the exact angle and amplitude as determined by x-ray analysis.”83
Spinal Stressology
“Standing and seated front-view and side-view full spine x-rays are recommended in severe pain patterns, work related injuries, automobile accidents and degenerative disease conditions. A system analysis consists of standing and seated front-view and side-view full spine x-rays. We can scientifically measure abnormal stress, and predict what specific damage it will cause if not corrected.”58
“A mental-emotional profile is an evaluation based on standing and seated, front and side view, full spine X-rays.”139
Sutter
“The exact variation of the atlas subluxation in relation to its surrounding structures peculiar to the individual case must be accurately determined. This can only be done through a specialized X-ray technique and analysis.”23
Zimmerman
“Due to the precision of the x-rays and other methods, [the chiropractor] is trained to place the tip of the machine so accurately as to do that which has never been done before.”86
“Two views taken down through the hole-in-the-head [sic] plus a side view and a front to back view constitute an X-Ray set. Analysis of these X-Rays provides the information needed to make the proper adjustment.”24
References
- 1.Palmer B.J. Introduction of spinography: its origin, purpose, field of labor and why. In: Thompson E.A., editor. Chiropractic spinography. 2nd ed. Palmer School of Chiropractic; Davenport, IA, USA: 1919. [Google Scholar]
- 2.Palmer B.J. Palmer School of Chiropractic; Davenport, IA, USA: 1924. The hour has struck. [Google Scholar]
- 3.Keating J.C., Jr. Association for the History of Chiropractic; Davenport, Iowa: 1997. B.J. of Davenport: the early years of chiropractic. [Google Scholar]
- 4.Palmer B.J. 3rd ed. vol. II. Palmer School of Chiropractic; Davenport, IA, USA: 1920. (The science of chiropractic). [Google Scholar]
- 5.Palmer B.J. vol. XXVIII. Chiropractic Fountain Head; Davenport, IA, USA: 1952. (Answers). [Google Scholar]
- 6.Palmer B.J. vol. XXV. Chiropractic Fountain Head; Davenport, IA, USA: 1951. (Chiropractic clinical controlled research). [Google Scholar]
- 7.Thompson E.A. 2nd ed. Davenport; Iowa, USA: 1919. Chiropractic spinography. [Google Scholar]
- 8.Webster G.V. Concerning osteopathy. Rloyd J Rich Printer and Publisher; Carthage, NY, USA: 1915. Scientific proofs of osteopathy. [Google Scholar]
- 9.Hullett G.D. Journal Printing Company; Kirksville, MO, USA: 1906. A text book of the principles of osteopathy. [Google Scholar]
- 10.Hazzard C. Journal Printing Company; Kirksville, MO, USA: 1905. The practice and applied therapeutics of osteopathy. [Google Scholar]
- 11.Fryette H.H. Academy of Applied Osteopathy; Carmel, CA, USA: 1954. Principles of osteopathic technic. [Google Scholar]
- 12.Downing C.H. Ricardo J Orozco; San Francisco, CA, USA: 1935. Osteopathic principles in disease. [Google Scholar]
- 13.Burns L., Chandler L.C., Rice R.W. American Osteopathic Association; Chicago, IL, USA: 1948. Pathogenesis of visceral disease following vertebral lesions. [Google Scholar]
- 14.Booth E.F. The Caxton Press; Cincinnati, OH, USA: 1924. History of osteopathy and twentieth-century medical practice. [Google Scholar]
- 15.Murray C.H. Chas. H. Murray; Elgin, IL, USA: 1912. Practice of osteopathy. [Google Scholar]
- 16.Martin S.C. Chiropractic and the social context of medical technology, 1895-1925. Technol Cult. 1993;34(4):808–834. [PubMed] [Google Scholar]
- 17.Keating J.C., Jr. Several pathways in the evolution of chiropractic manipulation. J Manip Physiol Ther. 2003;26(5):300–321. doi: 10.1016/S0161-4754(02)54125-7. [DOI] [PubMed] [Google Scholar]
- 18.Roy W Sweat Foundation . 2013. About Atlas Orthogonal. [ http://www.atlasorthogonality.com/PatientSite/aboutAO.html. Accessed April 12, 2013] [Google Scholar]
- 19.Procedures followed at this clinic: x-rays & type of chiropractic adjustment. 2013. http://www.chirocowin.com.au/index.php?p=1_4 [Accessed May 10, 2013]
- 20.Gonstead Clnical Studies Society . 2013. What makes us so special? [ http://www.gonstead.com/index.php?content_type=general_content&content=10. Accessed April 05, 2013] [Google Scholar]
- 21.Eriksen K. 2002. Orthospinology upper cervical. [ http://www.upcspine.com/tech5.htm. Accessed April 25, 2013] [Google Scholar]
- 22.The Pettibon System Treatment. 2012. http://pettibonsystem.com/treatment [Accessed May 06, 2013]
- 23.Sutter M. 1941. Sutter Specific Atlas Correction. [ http://www.upcspine.com/tech17.htm. Accessed July 14, 2014] [Google Scholar]
- 24.Canepa L. 2013. Just think it! Dr Zimmerman's Specific Adjusting Machine (SAM) [ http://www.just-think-it.com/sam.htm. Accessed May 11, 2013] [Google Scholar]
- 25.Cooperstein R., Gleberzon B.J. 1st ed. Churchill Livingstone; Edinburgh: 2004. Technique systems in chiropractic. [Google Scholar]
- 26.Palmer B.J. vol. XVIII. Palmer School of Chiropractic; Davenport, IA, USA: 1934. (The subluxation specific—the adjustment specific). [Google Scholar]
- 27.Dye A.A. 1st ed. A Aug Dye, DC; Philadelphia, PA, USA: 1939. The evolution of chiropractic: its discovery and development. [Google Scholar]
- 28.Wernsing A. Origins of the atlas specific. Am Chiropr Assoc J. 1959;1(5):11–13. [Google Scholar]
- 29.Quigley W.H. The last days of B.J. Palmer: revolutionary confronts reality. Chiropr Hist. 1989;9(2):11–19. [PubMed] [Google Scholar]
- 30.Wardwell W.I. Mosby-Year Book; St. Louis: 1992. Chiropractic: history and evolution of a new profession. [Google Scholar]
- 31.Moore J.S. Johns Hopkins University Press; Baltimore: 1993. Chiropractic in America: the history of a medical alternative. [Google Scholar]
- 32.Gibbons R.W., Rehm W.S. 2nd ed. Who's Who in Chiropractic International Publishing Co; Littleton, Colo: 1980. Who's who in chiropractic, international. [Google Scholar]
- 33.Chiropractic BioPhysics Origins of CBP®. 2013. http://www.idealspine.com/origins-of-cbp/ [Accessed April 14, 2013]
- 34.The Pettibon System X-ray procedures. 2012. http://pettibonsystem.com/course/x-ray-procedures [Accessed May 06, 2013]
- 35.Advanced Orthogonal Mission statement. 2013. http://www.advancedorthogonal.com/mission-statement/ [Accessed April 05, 2013]
- 36.Society of Chiropractic Orthospinology About Orthospinology. 2013. http://www.orthospinology.org/patients/what-is-orthospinology [Accessed May 05, 2013]
- 37.ChiroMatrix - Discover Wellness . Borges Chiropractic on ASBE. 2013. Borges Chiropractic – Research Supports Chiropractic. [Available at: http://borgeschiro.com/custom_content/c_215929_research_supports_chiropractic.html. Accessed April 07, 2013] [Google Scholar]
- 38.Grostic R.J. Welcome to your health potential. 2013. http://www.grosticchiro.com/5825.html [Accessed April 25, 2013]
- 39.Kale Chiropractic Center The brain stem. 2013. http://kale.com/kaleweb/chiropractic/brainstem.htm [Accessed May 03, 2013]
- 40.UCRF Current research/funding. 2013. http://www.ucrf.org/projects-funding [Accessed May 04, 2013]
- 41.American Academy of Clinical Applied Spinal Biomechanical Engineering Applied Spinal Biomechanical Engineering. 2013. http://www.asbechiro.com/index.html [Accessed April 07, 2013]
- 42.Chiropractic BioPhysics About the founder. 2013. http://www.idealspine.com/about-the-founder/ [Accessed April 14, 2013]
- 43.Amman M.J. 2013. Who was Dr. Gonstead? The history of Clarence S. Gonstead, D.C. [ http://www.gonstead.com/index.php?content_type=general_content&content=3. Accessed January 31, 2013, 2013] [Google Scholar]
- 44.Cooperstein R. Gonstead chiropractic technique. J Chiropr Med. 2003;2(1):16–24. doi: 10.1016/S0899-3467(07)60069-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Keating J.C., Jr. 1998. Hugh B Logan and the Logan Basic College of Chiropractic. [ http://www.chiro.org/Plus/History/Colleges/LoganCC/LoganCC-chrono1.pdf] [Google Scholar]
- 46.Gielow V. Bawden Brothers; Davenport, IA: 1981. Old Dad Chiro: a biography of D.D. Palmer, founder of chiropractic. [Google Scholar]
- 47.Sausser W.L. New spinographic technique: the full length x-ray plate is a success. Chiropr J. 1933;1(7):25. [Google Scholar]
- 48.Keating J.C., Jr. 2005. A history of the Logan College of Chiropractic. [Google Scholar]
- 49.Keating J.C., Jr. 1996. Hugh B Logan and the Logan Basic College of Chiropractic. [Google Scholar]
- 50.Logan H.B. 1950. Textbook of Logan Basic methods: from the original manuscript of Hugh B. Logan. V. Logan & F. Murray. [Google Scholar]
- 51.Hutti L.J., Unger-Boyd M. Structural x-ray marking systems. In: Hutti L.J., editor. Textbook of Logan basic methods. 4th ed. LBM, Inc; Chesterfield, MO, USA: 2006. pp. 119–126. [Google Scholar]
- 52.Stechschulte P. 2004. Profiles in chiropractic: Walter 'Vern' Pierce, DC. A man all about results. [ http://www.chiro.org/ChiroZine/FULL/Verne_Pierce.html. Accessed 12/03/14] [Google Scholar]
- 53.Noel K.S. Memorial. 2013. Dr Glenn Stillwagon. [Available at: http://www.findagrave.com/cgi-bin/fg.cgi?page=gr&GSln=Stillwagon&GSiman=1&GScnty=2303&GSob=c&GRid=122344908&. Accessed 12/03/14] [Google Scholar]
- 54.Hunt J. 2014. Dr Walter 'Vern' Pierce biography. [ http://www.sequencesystem.com/Dr._Pierce_Bio.html. Accessed 12/03/14] [Google Scholar]
- 55.Organization TCR . The Chiropractic Resource Organization. 2014. Pierce System Results. [Accessed 12/03/14] [Google Scholar]
- 56.Galgano J., Jaszewski E. 2014. About Pierce Results. Pierce Results Seminars: systematic approach to correcting subluxations. [ pierceresults.com. Accessed July 10, 2014, 2014] [Google Scholar]
- 57.Ward S. monologue. 2013. The evolution of the Ward chiropractic method. [video, Available at: http://www.youtube.com/watch?v=vbjl2DdER4A. Accessed May 16, 2013] [Google Scholar]
- 58.Ward chiropractic About. 2013. http://www.chiroman.com/about/ [Accessed May 16, 2013]
- 59.Dynamic Chiropractic Editorial Staff . vol. 11. MPA Media; 1993. Lowell Ward, DC, Stressology Pioneer. (Dynamic chiropractic). [online ed] [Google Scholar]
- 60.Sinnott R. Upper Cervical. 2014. Palmer upper cervical specific—HIO (Hole-in-One) [ http://www.upcspine.com/PDF/HIO.pdf, Accessed 15/07/2014, 2014] [Google Scholar]
- 61.University P . 2013. Chiropractic techniques. [ http://www.palmer.edu/ChiropracticTechniques/. Accessed 06/05/13] [Google Scholar]
- 62.International Upper Cervical Chiropractic Association Publications. 2013. http://www.pacificchiro.com/iucca/iucca_publications_page.htm [Accessed April 12, 2013]
- 63.International Upper Cervical Chiropractic Association . 2013. Frequently asked questions. [ http://www.pacificchiro.com/iucca/iucca_faq_page.htm. Accessed April 12, 2013] [Google Scholar]
- 64.International Upper Cervical Chiropractic Association . 2013. Applied Upper Cervical Biomechanics post-graduate education program. [ http://www.pacificchiro.com/iucca/aucb_program_page.htm. Accessed April 12, 2013] [Google Scholar]
- 65.Eriksen K., Rochester R.P., Hurwitz E.L. Symptomatic reactions, clinical outcomes and patient satisfaction associated with upper cervical chiropractic care: a prospective, multicenter, cohort study. BMC Musculoskelet Disord. 2011;12:219. doi: 10.1186/1471-2474-12-219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Duff R. 2013. Home page. [ http://www.duffchiropractic.net. Accessed April 21, 2013] [Google Scholar]
- 67.Duff R. 2013. About us. [ http://www.duffchiropractic.net/About-Us.html. Accessed April 21, 2013] [Google Scholar]
- 68.Eriksen K., Rochester R. 1st ed. Lippincott Williams & Wilkins; 2007. Orthospinology procedures: an evidence-based approach to spinal care, based on the John F Grostic model and procedure. [Google Scholar]
- 69.National Upper Cervical Chiropractic Association . 2013. About historical highlights. [ http://www.nucca.org/historical_highlights.php. Accessed May 03, 2013] [Google Scholar]
- 70.Kale B. 2012. Upper cervical specific knee chest history part 1. [ http://kaleblog.typepad.com/the_tic/2012/10/upper-cervical-specific-knee-chest-history-part-1.html. Accessed March 07, 2014] [Google Scholar]
- 71.Hart J.F. Remembering Dr Lyle Wheeler Sherman. Chiropr Hist. 1996;16(2):67–75. [PubMed] [Google Scholar]
- 72.Chiropractic SCo Chiropractic history. 2014. http://www.sherman.edu/home/chiropractic-history.asp [sherman, March 07, 2014]
- 73.TheSpecific The Specific Chiropractic Center—Kale Chiropractic Research Clinic. 2014. http://thespecific.com/blog/2011/02/07/kale-chiropractic-research-clinic/ [Accessed March 07, 2014]
- 74.KCUCS About KCUCS. 2013. http://www.kcucs.com/about-kcucs/ [Accessed May 03, 2013]
- 75.Kale Chiropractic Center Dr Kale. 2013. http://kale.com/kaleweb/chiropractic/drkale.htm [Accessed May 03, 2013]
- 76.TheSpecific What is specific chiropractic? 2014. http://thespecific.com/blog/what-is-specific-chiropractic/ [Accessed July 11, 2014]
- 77.TheSpecific Why we're different. 2014. http://thespecific.com/blog/why-were-different/ [Accessed July 11, 2014]
- 78.KCUCS About KCUCS—leadership. 2014. http://www.kcucs.com/about-kcucs/leadership/ [Accessed July 11, 2014, 2014]
- 79.KCUCS What makes KCUCS unique. 2013. http://www.kcucs.com/about-kcucs/what-makes-kcucs-unique/ [Accessed May 03, 2013]
- 80.KCUCS Blog. 2014. http://www.kcucs.com/category/blog/ [Accessed July 11, 2014, 2014]
- 81.Kessinger R. KCUCS Upper Cervical Case Presentation Series. 2013. KCUCS Upper Cervical Case Presentation Series - Volume 1. [video, use of post tx radiography. Available at: http://www.youtube.com/watch?v=_soXsD5LIWU. Accessed July 14, 2014, 2014] [Google Scholar]
- 82.KCUCS Research. 2013. http://www.kcucs.com/research/ [Accessed May 03, 2013]
- 83.Sherman College of Chiropractic . Seventh Annual Subluxation Conference. 1999. (Conference abstracts). [Available at: http://www.chiro.org/LINKS/FULL/subcon7.html. Accessed May 07, 2014] [Google Scholar]
- 84.Sutter M. Max Sutter; Huntington Park, CA, USA: 1941. The master key to health: specific atlas correction. [Google Scholar]
- 85.Green B.N., Johnson C.D., Andrew T., Martin P. Improving historical research reports: a case report format and example in arden zimmerman, D.C. J Chiropr Humanit. 1998;8:43–54. [Google Scholar]
- 86.Zimmerman A.D. An adjusting machine to correct subluxation. Digest of chiropractic economics. Vol 5. Ponte Vedra Beach, FL, USA. Chiropr Econ. 1963;14:22–25. [Google Scholar]
- 87.Sweat R.W., Sweat MH. Today's chiropractic. Life University; Marietta, GA, USA: 1995. Guidelines for pre and post radiographs for care documentation; pp. 58–61. [Google Scholar]
- 88.Blair Chiropractic Society About Dr Blair. 2013. http://www.blairchiropractic.com/about_dr_blair.htm [Accessed April 12, 2013]
- 89.Blair Chiropractic Society The Patient Experience. 2013. http://www.blairchiropractic.com/doctorvisit [Accessed July 14, 2013]
- 90.Society of Chiropractic Orthospinology Chiropractic Orthospinology Basic I Class. 2013. http://www.orthospinology.org/seminars/seminar-descriptions/basic-1-outline [Accessed May 05, 2013]
- 91.The Pettibon System Our history. 2012. http://pettibonsystem.com/our-history [Accessed May 06, 2013]
- 92.Woggon D. Dennis Woggon; St Cloud, MN, USA: 2000. The science of Pettibon Spinal Biomechanics Systems Adjusting 2001. [Google Scholar]
- 93.Advanced Orthogonal History of Advanced Orthogonal. 2013. http://www.advancedorthogonal.com/history-of-advanced-orthogonal/ [Accessed April 05, 2013]
- 94.Advanced Orthogonal The Advanced Orthogonal difference. 2013. http://www.advancedorthogonal.com/the-pierce-difference/ [Accessed April 07, 2013]
- 95.Pierce G.S. Pierce Clinic of Chiropractic. 2013. What to expect. [Accessed July 14, 2014] [Google Scholar]
- 96.Pierce G.S. Pierce Clinic of Chiropractic. 2013. Conditions chiropractic helps. [Accessed July 14, 2014] [Google Scholar]
- 97.Pierce G.S. Pierce Clinic of Chiropractic. 2013. FAQ. [Accessed July 14, 2014] [Google Scholar]
- 98.Upper Cervical Research Foundation Home page. 2013. http://www.ucrf.org [Accessed May 04, 2013]
- 99.UCRF News room. 2013. http://www.ucrf.org/newsroom [Accessed May 04, 2013]
- 100.Palmer J, Creswell K. A Brief History of the modus operandi of measuring and correcting the atlas subluxation complex syndrome and the role of posture in the National Upper Cervical Chiropractic Association (NUCCA) standard of care. http://www.ucrf.org/themes/nuccra/images_new/pdf/palmer.pdf. Date unknown.
- 101.National Upper Cervical Chiropractic Association About Mission Statement. 2013. http://www.nucca.org/mission.php [Accessed May 03, 2013]
- 102.NUCC Association . NUCCA standards of care and practice guidelines. In: NUCCA, editor. NUCCA; 1992. [Google Scholar]
- 103.Elliott SONAR Chiropractic Elliott SONAR Chiropractic Doctors. 2013. http://www.sonarchiropractic.com/sonarchiropracticdocs.htm [Accessed May 07, 2013]
- 104.Elliott SONAR Chiropractic Healing through SONAR. 2013. http://www.sonarchiropractic.com/sonarchiropractic/healing-through-sonar.htm [Accessed May 07, 2013]
- 105.Bronfort G., Haas M., Evans R., Leininger B., Triano J. Effectiveness of manual therapies: the UK evidence report. Chiropr Osteopat. 2010;18:3. doi: 10.1186/1746-1340-18-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Clar C., Tsertsvadze A., Court R., Hundt G., Clarke A., Sutcliffe P. Clinical effectiveness of manual therapy for the management of musculoskeletal and non-musculoskeletal conditions: systematic review and update of UK evidence report. Chiropr Man Ther. 2014;22(1):12. doi: 10.1186/2045-709X-22-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Bussieres A.E., Patey A.M., Francis J.J. Vol. 7. 2012. Identifying factors likely to influence compliance with diagnostic imaging guideline recommendations for spine disorders among chiropractors in North America: a focus group study using the Theoretical Domains Framework; p. 82. (Implementation science: IS). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Bussières A.E., Peterson C., Taylor J.A.M. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults—an evidence-based approach: introduction. J Manip Physiol Ther. 2007;30(9):617–683. doi: 10.1016/j.jmpt.2007.10.003. [DOI] [PubMed] [Google Scholar]
- 109.Bussières A.E., Peterson C., Taylor J.A.M. Diagnostic imaging guideline for musculoskeletal complaints in adults—an evidence-based approach—part 2: upper extremity disorders. J Manip Physiol Ther. 2008;31(1):2–32. doi: 10.1016/j.jmpt.2007.11.002. [DOI] [PubMed] [Google Scholar]
- 110.Bussières A.E., Taylor J.A.M., Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults—an evidence-based approach: part 1: lower extremity disorders. J Manipulative Physiol Ther. 2007;30(9):684–717. doi: 10.1016/j.jmpt.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 111.Bussières A.E., Taylor J.A.M., Peterson C. Diagnostic imaging practice guidelines for musculoskeletal complaints in adults—an evidence-based approach—part 3: spinal disorders. J Manip Physiol Ther. 2008;31(1):33–88. doi: 10.1016/j.jmpt.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 112.Elliott SONAR Chiropractic How SONAR works. 2013. http://www.sonarchiropractic.com/sonarchiropracticdocs.htm [Accessed May 07, 2013]
- 113.Khorsan R., Coulter I.D., Hawk C., Choate C.G. Measures in chiropractic research: choosing patient-based outcome assessments. J Manip Physiol Ther. 2008;31(5):355–375. doi: 10.1016/j.jmpt.2008.04.007. [DOI] [PubMed] [Google Scholar]
- 114.Hinton P.M., McLeod R., Broker B., MacLellan E. Outcome measures and their everyday use in chiropractic practice. J Can Chiropr Assoc. 2010;54(2):118–131. [PMC free article] [PubMed] [Google Scholar]
- 115.Gleberzon B.J. Chiropractic 'name techniques': a review of the literature. J Can Chiropr Assoc. 2001;45(2):86–99. [Google Scholar]
- 116.Owens E.F., Jr. Chiropractic subluxation assessment: what the research tells us. J Can Chiropr Assoc. 2002;46(4):215–220. [Google Scholar]
- 117.Fuller R.C. Oxford Press; New York: 1989. Alternative medicine and American religious life. [Google Scholar]
- 118.Martin S.C. "The Only Truly Scientific Method of Healing". Chiropractic and American Science, 1895 - 1990. Isis. 1994;88:207–227. doi: 10.1086/356807. [DOI] [PubMed] [Google Scholar]
- 119.Hildebrandt R.W. 2nd ed. MS Hilmark Publications; Wheaton, IL, USA: 1980. Chiropractic spinography: a manual of technology and interpretation. [Google Scholar]
- 120.Simpson J.K. The five eras of chiropractic & the future of chiropractic as seen through the eyes of a participant observer. Chiropr Man Ther. 2012;20(1):1. doi: 10.1186/2045-709X-20-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Cooperstein R. ACA Today. American Chiropractic Association; 2005. The superproliferation of chiropractic techniques. [internet] [Google Scholar]
- 122.Nelson C.F. The cognitive roots of chiropractic theories adn techniques. J Chiropr Humanit. 1993;3(1):42–55. [Google Scholar]
- 123.Savolainen R. Emotions as motivators for information seeking: a conceptual analysis. Libr Inf Sci Res. 2014;36(1):59–65. [Google Scholar]
- 124.Young K.J., Keating J.C., Jr., Waldo G., Poehner D.C. DACBR: a force for progressiveness. Chiropr Hist. 2009;29(1):9–15. [Google Scholar]
- 125.Young K.J. Michael A. Giammarino, D.C., D.A.C.B.R.: student, teacher, leader. Chiropr Hist. 1998;18(2):33–38. [PubMed] [Google Scholar]
- 126.Young K.J. Joseph W. Howe, D.C., D.A.C.B.R. and the development of modern chiropractic radiology. Chiropr Hist. 1999;19(2):27–47. [PubMed] [Google Scholar]
- 127.Rodwint A. Stains in the fiduciary metaphor: divided physician loyalties and obligations in a changing health care system. Am J Law Med. 1995;21(2,3):241–257. [PubMed] [Google Scholar]
- 128.Blair Chiropractic Society Blair Chiropractic Society. 2013. http://www.blairchiropractic.com home page. [Accessed April 12, 2013]
- 129.UpCSpine Upper Cervical Orthogonal—Cowin. 2013. http://www.upcspine.com/tech1.htm [Accessed May 10, 2013]
- 130.Gonstead Clinical Studies Society Basic principles. 2013. http://www.gonstead.com/index.php?content_type=general_content&content=11 [Accessed April 05, 2013]
- 131.Logan H.B. Logan College of Chiropractic; St Louis, MO, USA: 1950. Textbook of Logan basic methods. [Google Scholar]
- 132.National Upper Cervical Chiropractic Association Patients frequently asked questions. 2013. http://www.nucca.org/faq.php [Accessed May 03, 2013]
- 133.Buchanan G. 2002. Advanced Orthogonal—Dr Stanley Pierce Sr and Jr. [ http://www.upcspine.com/tech7.htm. Accessed April 05, 2013] [Google Scholar]
- 134.International Upper Cervical Chiropractic Association Research page. 2013. http://www.pacificchiro.com/iucca/iucca_research_page.htm [Accessed April 12, 2013]
- 135.Chiropractic BioPhysics What is CBP. 2013. http://www.idealspine.com/what-is-cbp/ [Accessed April 14, 2013]
- 136.UpCSpine Kale Upper Cervical. 2013. http://www.upcspine.com/tech6.htm [Accessed May 03, 2013]
- 137.Kessinger R. 2013. Dr Robert Kessinger (KCUCS) [ http://www.youtube.com/KCUCS7. Accessed May 03, 2013] [Google Scholar]
- 138.Young K.J. Warren l. Sausser, D.C.: influence unrecognized. Chiropr Hist. 1997;17(1):75–83. [Google Scholar]
- 139.Ward S. 2013. Mental emotional profiles. [ http://chiroman.com/services/mental-emotional-profiles/. Accessed May 16, 2013] [Google Scholar]