

Abstract
Tenodesis of the long head of the biceps tendon (LHB) at the upper part of the bicipital groove has been related to persistent postoperative bicipital pain. This is possibly due to the inflammation of the remaining tendon within the groove. This, in turn, could be attributed to the continual mechanical stress placed on the tendon in the narrow bicipital groove. Theoretically, should the LHB be more “relaxed,” the mechanical stress applied on it would be diminished. On the basis of this rationale, we present an arthroscopic biceps tenodesis technique, according to which the tendon is fixed at the entrance of the bicipital groove, using a bioabsorbable screw, relaxed by 5 mm. In this lax position, the residual LHB tension is expected to be decreased compared with the initial tension, whereas no cosmetic deformity (Popeye sign) or impaired muscular performance is anticipated.
Tenodesis is the ideal treatment for persistent painful pathology of the long head of the biceps tendon (LHB) in young and active patients, especially with thin arms, because it preserves muscular performance and has a good cosmetic result.1,2 Various techniques, both arthroscopic and open, have been described concerning fixation options and proximal (upper portion of the groove) or distal (“suprapectoral” or “subpectoral”) tenodesis location.3-5
Specifically, it has been advocated that proximal tendon fixation is related to persistent postoperative bicipital pain. This is possibly due to the inflammation of the remaining tendon within the groove. Indeed, Sanders et al.,6 in a retrospective study, found that there is an increased revision rate when the biceps tendon is fixed proximally compared with distally. These findings are further supported by Refior and Sowa,7 who—in a cadaveric study—showed that the distal part of the biceps, as it exits the bicipital groove, exhibited degenerative and inflammatory changes. They attributed these findings to the continual mechanical stress placed on the tendon in the narrow bicipital groove.
Theoretically, should the biceps be more “relaxed,” the mechanical stress applied on it would be diminished. On the basis of this rationale, we present an arthroscopic biceps tenodesis technique, according to which the tendon is fixed proximally but in a lax position.
Surgical Technique
The patient is placed in the beach-chair position, under general anesthesia and an interscalene block. Two kilograms of caudal traction is applied on the arm, which is flexed 30°. A standard posterior viewing portal is created. The intra-articular pressure is calibrated to 50 mm Hg using a pump (FMS DUO Fluid Management System; DePuy Mitek, Warsaw, IN). Diagnostic arthroscopy is performed. If the diagnosis of LHB pathology is confirmed, the “tenodesis” portal is created using spinal needle localization. The needle is inserted through the rotator cuff interval and over the biceps tendon. It must be oriented toward the entrance of the bicipital groove. That is the point at which the bio-tenodesis will take place. Once the direction is determined, the portal is created, through the rotator cuff interval. With the elbow in extension and with the use of a hook probe with 5-mm markings, the length of the LHB is evaluated from its insertion onto the labrum to its entrance into the bicipital groove (distance A) (Fig 1).
Fig 1.
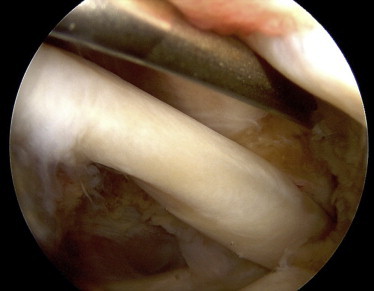
The length of the LHB is evaluated using a hook probe with 5-mm markings from its insertion onto the labrum to its entrance into the bicipital groove. The elbow must be kept in extension.
LHB tenotomy is carried out just above the labrum using bipolar radiofrequency ablation (Coolpulse 90; DePuy Mitek) through the tenodesis portal with the elbow in flexion. Care is taken not to affect the labrum. The pathologic LHB is generally flattened. This morphology inhibits the intragroove migration of the tendon after it has been dissected (Video 1). This is why we do not use any sutures to keep the tendon in an intra-articular position during tenotomy. Thus the duration of the operation is diminished. The tendon is grasped and exteriorized through the anterior portal with a suture retriever (Video 1). To facilitate tendon exteriorization, the elbow is flexed and the forearm is supinated. A clamp (Kocher forceps) is placed at the tip of the tendon to facilitate its pulling and further handling. In case of a hypertrophic LHB, its proximal end is regularized using the No. 11 blade to facilitate its entrance into the tunnel. By use of a ruler and a marker, a mark is made on the tendon at a distance (distance A, the intra-articular length of the LHB that was previously measured) from its free end. By use of No. 2 FiberLoop (Arthrex, Naples, FL), 5 stitches are made on the tendon between the initial mark and its free end. A new mark is made 5 mm proximal to the initial mark (Fig 2).
Fig 2.

The LHB is exteriorized. By use of No. 2 FiberLoop, 5 stitches are made on the tendon up to its free end, covering a distance that corresponds to its intra-articular length. A new mark is made 5 mm proximal to the initial mark (arrow). The tendon must be inserted into the humeral head tunnel for its fixation up to this new mark (asterisk). Thus the residual tendon is relaxed by 5 mm.
Through the superolateral portal, the humeral tunnel is prepared. A 2.4-mm guidewire is drilled into the humerus at the entrance of the bicipital groove. By use of a 7-mm cannulated drill bit over the 2.4-mm guidewire, a tunnel 25 mm deep is created (Video 1). Bone debris and tissue that may obstruct tendon introduction are removed by radiofrequency ablation (Coolpulse 90). The cannulated Bio-Tenodesis driver (Arthrex) is loaded with a cannulated biodegradable 7 × 23–mm screw (Bio-Tenodesis Screw; Arthrex). The free ends of the FiberWire suture (Arthrex) attached to the tendon are passed through the distal loop of the cannulated Bio-Tenodesis driver and retrieved proximally on the handle until the tendon reaches the distal tip of the driver. The proximally retrieved sutures are then secured on the driver (Video 1). With the elbow in extension, the tendon is introduced inside the tunnel. It is inserted up to the proximal mark. Thus a relaxation of 5 mm is achieved. After screw placement, the material is removed and the sutures are cut. Then, repair of any coexisting lesions is performed. We suggest performing the bio-tenodesis before any other act to avoid swelling of the shoulder.
Discussion
The proposed technique addresses an arthroscopic tenodesis of the LHB at the entrance of the bicipital groove that aims to provide decreased tension to the residual tendon compared with the initial tension. This is accomplished because the length of the residual tendon up to the tenodesis insertion point is greater by 5 mm compared with the correspondent tendon length before the operation. This denotes a decrease in the mechanical stress on the LHB and therefore, as outlined in our rationale, diminution of the risk of persistent tendon pathology and pain.6,7 In addition, the elongation is only 5 mm, which rules out the cosmetic deformity (Popeye sign) encountered after tenotomy.
Some skepticism may exist regarding the consequential muscular strength because the normal length-tension relation is not maintained. However, the clinical significance of this phenomenon remains doubtful. Wittstein et al.8 examined isokinetic strength and endurance for elbow flexion and forearm supination after LHB tenotomy and tenodesis and found that there was no difference between the operated and nonoperated sides for both groups and all parameters apart from supination peak torque for the tenotomy group. Thus the clinical relevance of the potential muscle strength deficit after the relaxed LHB tenodesis seems trivial.
Furthermore, according to the proposed technique, no action is taken distally, inside the biceps pulley. Thus the vascularization of the tendon is respected.9
Finally, biomechanical studies have proved that LHB tenodesis with a 25-mm interference screw or even a 15-mm interference screw is sufficient,10 explaining why interference screw fixation has been chosen.
The 5-mm elongation of the residual LHB according to the relaxed LHB tenodesis offers the advantage of limited risk of persistent tendon pathology and pain without cosmetic deformity (Popeye sign). In addition, the vascularization is respected. Care should be taken, however, when exteriorizing and preparing the tendon (Table 1).
Table 1.
Tips
| The tenotomy must be carried out proximally, at the insertion of the tendon to the labrum. The pathologic LHB is generally flattened. This morphology inhibits the intragroove migration of the tendon after it has been dissected. No sutures are needed to keep the tendon in an intra-articular position during tenotomy. |
| Tendon exteriorization is facilitated when the elbow is flexed and the forearm is supinated. |
| In case of a hypertrophic LHB, its proximal end is regularized using the No. 11 blade to facilitate its entrance into the tunnel. |
| The bio-tenodesis should be performed before any other act to avoid swelling of the shoulder. |
In conclusion, relaxed LHB tenodesis is an easily reproducible, effective, and fast technique. It is an arthroscopic technique necessitating 2 portals and permitting the surgeon to treat any coexisting pathology at the same time.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Relaxed biceps tenodesis technique in a right shoulder. The patient is placed in the beach-chair position, under general anesthesia and an interscalene block. Two kilograms of caudal traction is applied on the arm, which is flexed 30°. A standard posterior viewing portal is used. The tendon is fixed at the entrance of the bicipital groove, using a bioabsorbable screw, relaxed by 5 mm. In this lax position, the residual LHB tension is expected to be decreased compared with the initial tension, whereas no cosmetic deformity (Popeye sign) or impaired muscular performance is anticipated.
References
- 1.Shank J.R., Singleton S.B., Braun S. A comparison of forearm supination and elbow flexion strength in patients with long head of the biceps tenotomy or tenodesis. Arthroscopy. 2011;27:9–16. doi: 10.1016/j.arthro.2010.06.022. [DOI] [PubMed] [Google Scholar]
- 2.Koh K.H., Ahn J.H., Kim S.M., Yoo J.C. Treatment of biceps tendon lesions in the setting of rotator cuff tears: Prospective cohort study of tenotomy versus tenodesis. Am J Sports Med. 2010;38:1584–1590. doi: 10.1177/0363546510364053. [DOI] [PubMed] [Google Scholar]
- 3.Lutton D.M., Gruson K.I., Harrison A.K., Gladstone J.N., Flatow E.L. Where to tenodese the biceps: Proximal or distal? Clin Orthop Relat Res. 2011;469:1050–1055. doi: 10.1007/s11999-010-1691-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Boileau P., Krishnan S.G., Coste J.S., Walch G. Arthroscopic biceps tenodesis: A new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18:1002–1012. doi: 10.1053/jars.2002.36488. [DOI] [PubMed] [Google Scholar]
- 5.Scully W.F., Wilson D.J., Grassbaugh J.A., Branstetter J.G., Marchant B.G., Arrington E.D. A simple surgical technique for subpectoral biceps tenodesis using a double-loaded suture anchor. Arthrosc Tech. 2013;2:e191–e196. doi: 10.1016/j.eats.2013.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sanders B., Lavery K., Pennington S., Warner J.J.P. Biceps tendon tenodesis: Success with proximal versus distal fixation (SS-16) Arthroscopy. 2008;24S: e9 (abstr) [Google Scholar]
- 7.Refior H.J., Sowa D. Long tendon of the biceps brachii: Sites of predilection for degenerative lesions. J Shoulder Elbow Surg. 1995;4:436–440. doi: 10.1016/s1058-2746(05)80035-7. [DOI] [PubMed] [Google Scholar]
- 8.Wittstein J.R., Queen R., Abbey A., Toth A., Moorman C.T., III Isokinetic strength, endurance, and subjective outcomes after biceps tenotomy versus tenodesis: A postoperative study. Am J Sports Med. 2011;39:857–865. doi: 10.1177/0363546510387512. [DOI] [PubMed] [Google Scholar]
- 9.Cheng N.M., Pan W.R., Vally F., Le Roux C.M., Richardson M.D. The arterial supply of the long head of biceps tendon: Anatomical study with implications for tendon rupture. Clin Anat. 2010;23:683–692. doi: 10.1002/ca.20992. [DOI] [PubMed] [Google Scholar]
- 10.Slabaugh M.A., Frank R.M., Van Thiel G.S. Biceps tenodesis with interference screw fixation: A biomechanical comparison of screw length and diameter. Arthroscopy. 2011;27:161–166. doi: 10.1016/j.arthro.2010.07.004. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Relaxed biceps tenodesis technique in a right shoulder. The patient is placed in the beach-chair position, under general anesthesia and an interscalene block. Two kilograms of caudal traction is applied on the arm, which is flexed 30°. A standard posterior viewing portal is used. The tendon is fixed at the entrance of the bicipital groove, using a bioabsorbable screw, relaxed by 5 mm. In this lax position, the residual LHB tension is expected to be decreased compared with the initial tension, whereas no cosmetic deformity (Popeye sign) or impaired muscular performance is anticipated.