

Abstract
Objective
To investigate the role of executive function (EF) skills, measured by parent-rating and performance-based instruments, as mediators of the effects of gestational age on functional outcomes and behavior symptoms in preterm and full term preschoolers.
Patients and methods
Children born preterm (n=70; mean gestational age 29.6 weeks and mean birth weight 1365g) were compared to children born full term (n=79) on composite measures of EF (using the Behavior Rating Inventory of Executive Function and a performance-based EF battery), adaptive function, prereading skills, and behavior symptoms. For the entire sample, mediation analyses examined the effect of gestational age on outcomes with EF as mediator.
Results
Compared to children born full term, children born preterm had significantly higher parent-rated EF scores and lower performance-based EF scores, both indicating more problems; further, children born preterm had lower adaptive function and prereading scores and more problematic behavior. Gestational age contributed to adaptive function, prereading skills, and behavior symptoms for all children. EF acted as a mediator of gestational age for all three outcomes; different patterns emerged for parent-rated and performance-based EF evaluations. For adaptive function, both EF measures significantly mediated effects of gestational age; for prereading skills, only performance-based EF was significant; for behavior symptoms, only parent-rated EF was significant.
Conclusions
We propose standard assessment of EF, using both parent-rating and performance-based EF measures, in young preterm children and other children at risk of EF impairments. EF skills are measurable, mediate important functional outcomes, and may serve as intervention targets.
Keywords: premature birth, preterm, executive function, adaptive function, reading, behavior, mediation
Preterm birth is associated with adverse outcomes, including impairments in multiple functional domains and increases in the number of behavior problems. Executive function (EF) skills -- interrelated cognitive processes used to direct goal-oriented behavior -- may contribute to functional abilities. The overall goal of this study is to determine if weakness in EF skills may help explain adverse outcomes in children born prematurely.
The study of EF in typically developing children has focused on the developmental trajectory of EF skills such as inhibitory control (i.e., resisting an automatic response in order to do what is requested or needed), working memory (i.e., holding information on-line despite competing information or while manipulating other information), cognitive flexibility (i.e., adjusting to changed demands; switching between rules or tasks), and organization, sequencing, and planning.1, 2 Studies of typically developing children also focus on EF skills as correlates or predictors of academic outcomes or behavior problems, including inattentiveness, hyperactivity, and impulsivity.3–5 We focused on children born preterm as a population at high-risk for EF impairments. There are two reasons that children born preterm may be a useful model with the potential to elucidate the neurobiological basis of EF impairments: 1) preterm children are at risk for brain injury in multiple structures, including white matter pathways,6, 7 and 2) EF skills have been linked to brain structures and neural networks in several neuropsychological and neuroimaging studies of typical and atypical development.1, 8–10
Studies of children born preterm have documented impairments in EF,11, 12 as well as impaired adaptive function and learning and behavior problems.13–15 While the independent associations between preterm birth and adverse outcomes are well-established, less is known about the relations between functional outcomes and EF impairments in children born preterm. The biological factors associated with preterm birth affect long-term outcomes, but likely act in concert with environmental factors to influence EF abilities. We were interested in whether measures of EF serve as an intervening or mediating variable between the effects of gestational age and functional outcomes.
We focused on three functional outcomes that are associated with EF skills in typical and clinical populations. The first outcome is adaptive function. In typical populations and in clinical populations (such as children with autism spectrum disorders16 and adolescents with externalizing behaviors17), EF skills have been shown to correlate with overall adaptive function across the lifespan.18 In children born preterm, much less is known about the relationships between EF skills and adaptive outcomes. Two studies that have examined the links between EF skills and overall adaptive function have evaluated school-aged preterm children,15, 19 but the association has not been adequately evaluated in preschool-aged children born preterm.
The second outcome is early literacy or prereading skills. Associations between EF skills and academic achievement have been well studied in typically developing children; these studies provide support for the belief that EF skills are critically important for school success. Cross-sectional studies of school-aged children show links between EF and math,20 language skills,21 and science.22 Longitudinal studies starting in preschool also find links between EF and later academic achievement.1, 3, 4, 20, 23 Complex memory performance at age 5 predicts performance on measures of language, mathematics and literacy at age 8.24 The studies of preterm children linking EF skills and academic achievement,25 including reading,19, 26–28 math,28, 29 and spelling,26 have focused on school-aged children.
The third outcome is behavior problems or symptoms. In typical and clinical populations, EF skills have been shown to correlate with behavior problems or symptoms.30, 31 Increased inattention and internalizing behaviors have been well-documented in preterm children,11, 14 although only a few studies have used mediation models to investigate whether cognitive abilities, including EF, act as mediators to influence behavior outcomes.32–34 In a longitudinal study, Nadeau and colleagues found that general intellectual ability measured at age 5 years 9 months mediated the effects of gestational age on both hyperactivity and inattention at age 7 years; further analysis revealed that a specific working memory factor mediated inattention.34 To date, the question of whether EF skills mediate behavior symptoms has not been examined in preschoolers born preterm.
Our principal study aim was to assess whether EF mediated the relationships between gestational age and three functional outcomes in preschool children: adaptive function, prereading skills, and behavior symptoms. We used a group of children born preterm as a biologic model with increased risk for EF impairments and previously described differences in parent-rated EF versus performance on laboratory tests to assess EF (hereafter referred to as performance-based EF).35 Previously, we have shown that parent-rated and performance-based EF identified overlapping and distinct groups of children with EF impairments, suggesting that the two types of EF measures tap overlapping and unique aspects of the EF construct.35 Therefore we were interested in examining both types of measures in relation to functional outcomes. We hypothesized that (1) compared to children born at term, children born preterm have poorer adaptive function and prereading skills and more behavior symptoms; (2) after accounting for any influence of socioeconomic status, gestational age directly contributes to functional outcomes and to both parent-rated and performance-based EF; and (3) both parent-rated and performance-based EF act as mediators of the effect of gestational age on all three functional outcomes.
METHODS
Participants
Participants were 3 to 5 year old children recruited from Palo Alto, CA, and surrounding counties. Study subjects had a history of preterm birth (PT) (≤ 34 weeks gestation) and BW < 2500 g (n = 70). A comparison group was comprised of children born full term (FT) (≥ 37 weeks) and had no major medical complications (n = 79). Exclusion criteria for all participants included sensory impairments (i.e., blind or deaf), identified genetic syndrome or congenital heart disease, and inability to comprehend task instructions. Comprehension was not formally assessed with language or intelligence tests prior to enrollment; however, ability to participate was estimated during an IRB-approved phone screening. Parents were asked questions to assess parent perception of the child’s overall development (i.e., “How is your child doing compared to other children his or her age? Has your child had a recent developmental or IQ test?”) Medical complications at birth in the preterm group included: 11 had abnormal findings on head ultrasound or MRI (at least grade 2 intraventricular hemorrhage or IVH, echodensities, or cystic lesions) and 10 had mildly abnormal findings (grade 1 IVH or choroid plexus cyst); 40 had respiratory distress syndrome (RDS) and 7 developed chronic lung disease; 5 had necrotizing enterocolitis; and 8 were small for gestational age (SGA, defined as lying at or below the 3rd percentile in birth weight for GA). RDS was associated with GA. Given the relatively small number of PT children with other medical complications, in our analyses we use GA as a summary indicator of neonatal complications.
The study population consisted of a convenience sample of children born from 2004 to 2009. PT subjects were recruited by letters sent to families of children who were evaluated at High Risk Infant Follow-up Services at Lucile Packard Children’s Hospital at Stanford in Palo Alto, CA, and by postings on local parent message boards. Comparison group children born full term were recruited by postings on parent message boards, by flyers in general pediatric clinics, and by word of mouth. Children born full term were group-matched to children born preterm for age, gender, ethnicity, and race. Maternal education (3 categories: < 4-year college degree, 4-year college degree, MA or higher) was used as the measure of socioeconomic status (SES).
The study was approved by the Stanford University Institutional Review Board. A parent or legal guardian provided informed consent. Participants were compensated for participation.
Measures and Variables
Participant characteristics
GA, birth weight, and medical complications were gathered from parent report and medical records. Demographic information included race, ethnicity, maternal and paternal education, household composition, and parent report of services.
IQ
Full scale IQ was estimated using the two-subtest format of the Stanford-Binet Intelligence Scales, 5th edition,36 an assessment of intelligence and cognitive abilities in individuals age 2–85+ years. Vocabulary and object-series/matrices subtests are combined to provide the Abbreviated Battery IQ (ABIQ).
Behavior Rating Inventory of Executive Function-Preschool version
(BRIEF-P), a standardized parent-rating scale of behavioral manifestations of EF in children 2.0–5.11 years.37 Sixty-three items measure aspects of EF: Inhibit, Shift, Emotional Control, Working Memory, and Plan/Organize. Three broad indices (Inhibitory Self-Control, Flexibility, Emergent Metacognition) and a composite score (Global Executive Composite, GEC) are also reported. Items are rated on a 3-point scale of “never,” “sometimes,” or “often.” Scores are reported as t-scores (mean of 50, SD of 10) in which higher scores indicate greater executive dysfunction. Scores at or above 65 are considered clinically significant. The measure is normed for gender and age by two groupings: 2:0 to 3:11 and 4:0 to 5:11. Content validity is based on factor analysis of clinical and normative samples, convergence/discriminance with preschool rating scale measures, and on the ability to detect EF deficits in children with risk factors or disorder.38 Examples of items from the BRIEF-P that tap specific EF constructs are as follows: inhibit—”acts too wild or out of control”; working memory—”cannot stay on the same topic when talking” and “has trouble remembering something, even after a brief period of time”; plan/organize—”has trouble thinking of a different way to solve a problem or complete an activity when stuck” and “when instructed to clean up, puts things away in a disorganized, random way.” We used the GEC as a summary measure of parent-rated EF skills.
Performance EF Battery
Tasks were selected to represent core EF constructs based on the developmental literature in typical and PT preschoolers.11, 12, 39–41 Tasks included: (1) 3- and 6- Boxes Task measures self-ordered working memory and planning.42 Three, and then six, stationary boxes with different color lids are baited with a treat in view of the child. The child’s task is to find all treats in the least number of reaches by keeping track of the boxes that have already been searched. (2) Verbal Fluency measures idea generation with language and organizational components (i.e., the use of subcategories as a strategy results in increased productivity).43 The task requires the child to generate as many words as possible within specific categories (i.e., animals, foods) in one minute. (3) Day/Night measures complex response inhibition, defined as response inhibition coupled with working memory.44 The child must hold a rule in mind and respond while inhibiting a prepotent response, suppressing competing visual information when responding. The child should respond “night” when shown a picture of the sun and “day” when shown a picture of moon and stars.45 (4) Bird/Dragon also measures complex response inhibition, defined as response inhibition and working memory.46 A modified “Simon Says” task, the child should follow verbal instructions of one puppet (bird), but not the other puppet (dragon). (5) Dimensional Change Card Sort, measures cognitive flexibility/task switching and attention shifting.47 The child is shown cards depicting colored shapes that can be sorted according to color or shape. The child must sort according to one dimension and then shift to sort according to the other dimension.
We previously have reported gestational age-based group differences on each of the tasks in the EF battery and have described the measures in greater detail, demonstrating that performance-based EF is significantly correlated with BRIEF-P indexes.35 We converted continuous outcome measures from the performance-based EF tasks to z-scores derived from performance (mean, SD) of full term subjects in the three age groups of 3, 4, and 5 years.35 Factor analytic studies of EF in younger children suggest that EF skills are less differentiated at younger ages.48 Therefore, in our analyses, we used an average z-score for the 5 EF tasks as a summary indicator of performance-based EF.35
Vineland Adaptive Behavior Scales, Second Edition (Vineland II), Parent/Caregiver Rating Form.49
This well-known measure of adaptive skills from birth to adulthood generates standard scores (mean=100, SD=15), percentiles, and age equivalents in the following domains: Communication, Daily Living Skills, Socialization, and Motor Skills. A composite score, the Adaptive Behavior Composite, is also generated. We used the Adaptive Behavior Composite as a summary measure of children’s overall adaptive function.
Test of Preschool Early Literacy (TOPEL).50
The TOPEL measures abilities related to early literacy and is designed to identify children at risk of having or developing problems in literacy. It is comprised of three subtests, Print Knowledge, Definitional Vocabulary, and Phonological Awareness. We selected the Phonological Awareness subtest in order to measure a child’s ability to detect and manipulate the sounds in spoken language independent of meaning. The Phonological Awareness subtest includes 12 elision items (e.g. “Say playground without ground”) and 15 blending items (e.g., “What word do these sounds make: f –ox?”). Practice items with feedback ensure comprehension of the tasks. Children are first presented with tasks that require manipulation of compound words before moving on to more difficult items involving elision or blending of individual phonemes.
Child Behavior Checklist
Parents completed the Child Behavior Checklist for Ages 1.5–5 (CBCL/1.5–5),51 a well-validated, broadband behavior rating questionnaire that includes 99 items rated on a 3-point Likert scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). The items describe specific kinds of behavioral, emotional, and social problems that characterize preschool children. Items are grouped into syndrome scales designated as Emotionally Reactive; Anxious/ Depressed; Somatic Complaints; Withdrawn; Attention Problems; Aggressive Behavior, and Sleep Problems. Syndrome scales are combined to generate two broadband scales: Internalizing (consists of Emotionally Reactive, Anxious/Depressed, Somatic Complaints, and Withdrawn) and Externalizing (consists of Attention Problems and Aggressive Behavior). A Total Problems score is generated from the sum of scores for all 99 items. Scores are reported as t-scores (mean=50, SD=10) in which higher scores indicate more problems. T-scores are normed for gender and age. For Total, Internalizing, and Externalizing, scores above 63 (> 90th percentile) are considered in the clinical range. Scores of 60–63 are considered in the borderline clinical range. We focused on the Total Problems t-score as a summary measure to capture a wide range of behavior symptoms.
Analyses
To compare demographic variables, IQ, composite EF scores (i.e., EF battery z-score, BRIEF-P GEC), and functional outcome scores between FT and PT groups, we used t-tests for continuous variables and Pearson chi-square for dichotomous outcomes. We used chi-square to assess group differences in proportions of participants with scores in the borderline and clinical ranges compared to nonclinical ranges or the below-average compared to average/above-average range. We used Spearman correlation to assess the relationships between the BRIEF-P GEC and EF battery z-score as well as between BRIEF-P subscales and the five individual EF tasks.
To investigate the contribution of GA to functional outcomes and the potential role of parent-rated and performance-based EF skills as mediators, we chose the mediation analysis method of Hayes and Preacher.52 Mediation analysis tests whether the effects of a given predictor variable on an outcome can be accounted for by its effect on an intermediate variable, or mediator, which in turn affects the outcome. Many past mediation studies have used a causal steps approach, for example Baron and Kenny,53 which relies on tests of significance of individual paths in a mediation model and inferring the existence of an indirect effect rather than quantifying it.54 SPSS Process macros, version 2.11, by Hayes and Preacher52 allows for quantification of indirect effects in multiple mediator models using bootstrapping. The method is advantageous in that it respects any irregularity of the sampling distribution of the indirect effect rather than assuming that it is normal. We used a bootstrapping method with 10,000 re-samples to examine mediation effects since the technique makes no distributional assumptions. An indirect effect can be interpreted as significant with 95% confidence if zero is outside of the confidence interval. The method assesses the (1) total effects model (c in Figure 1a), a model of the outcome variable when estimated from the predictors and covariates without the mediator(s), (2) the direct effect (c’ in Figure 1b), or the effect of the predictors and covariates on the outcome while including the mediator(s), and (3) the indirect effect through the mediator (paths a and b in Figure 1b). When evaluating mediators simultaneously, the method also estimates the effect and confidence interval for the difference between the indirect effects resulting from these mediators, allowing for the comparison of each mediator’s relative importance in explaining the relationship between the predictor and outcome. Another advantage is that for models with a single mediator and no covariates, the method generates a value called kappa-squared (κ2) which expresses the indirect effect as a ratio to the maximum possible indirect effect that could have been found given the study design. Because kappa-squared is a proportion between 0 and 1, it can be interpreted and equated to the values used for R2: a small effect is .01, a medium effect is approximately .09, and a large effect is .25.55, 56
Figure 1.
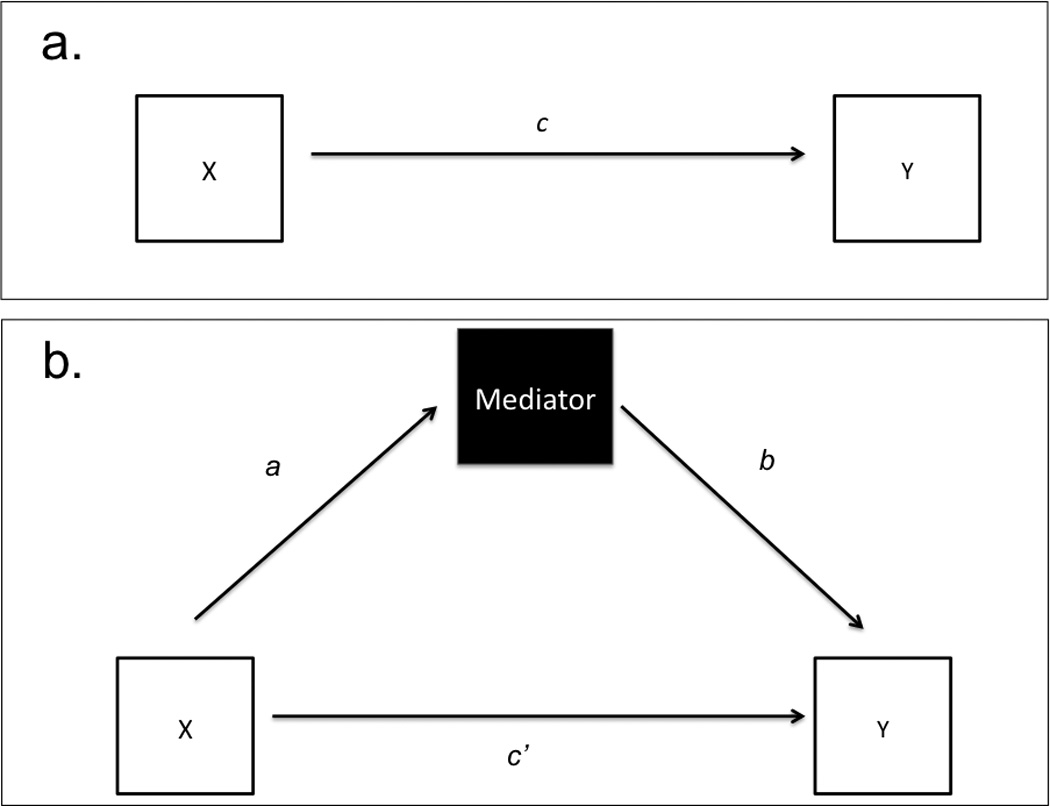
1a. Total Effects Model—shows the relationship (c) between predictor X and outcome Y. 1b. A simple mediation model in path diagram form includes the mediator and its relationship to predictor X (a) and outcome Y (b), or indirect effect. The direct effect between X and Y (accounting for the mediator in the model) is illustrated by c’.
In the mediation models, we used GA as the main predictor variable and maternal education as a covariate. To assess EF skills as mediators, we used the BRIEF-P GEC as a measure of parent-rated EF and the EF battery z-score as a measure of performance-based EF. The functional outcomes of interest were overall adaptive function, as measured by the Vineland Adaptive Behavior Composite score, prereading skills, as measured by the TOPEL Phonologic Awareness subtest standard score, and behavior symptoms, as measured by the CBCL Total Behavior Problems t-score. The BRIEF-P, Vineland, and CBCL are normed for age and sex, therefore age and sex variables were not included in the models. If maternal education was not significant in the models, we would re-estimate the models without any covariates in order to generate the kappa-squared value.
Missing data
For the BRIEF-P, data were incomplete for 4 PT participants. Data were missing from the EF battery as follows: 1 PT child for the bird/dragon task (would not play); 1 PT and 1 FT child for the day/night task (technical failure); 14 PT and 6 FT for the verbal fluency task (change in testing protocol). There were no significant differences in demographic variables for PT and FT groups completing the verbal fluency task compared to the larger study sample. For the Vineland, data were incomplete for 9 PT and 5 FT participants. The testing protocol was shortened for younger participants in order to minimize fatigue, such that most 3-year old participants did not complete the TOPEL. Seventy-five children completed the TOPEL; 42 FT and 32 PT did not. The demographics of the smaller sample completing the TOPEL showed no differences in participant characteristics and demographic variables compared to the patterns in the larger sample, except for a mean age of 4.8 years in both groups. CBCL data were incomplete for 1 PT participant. For analyses with missing data, degrees of freedom were adjusted accordingly. Significance level was set at p < .05.
RESULTS
Participant Characteristics
There were no differences between PT and FT groups in terms of age, race, ethnicity, or gender. (Table 1) By design, PT and FT groups differed in GA and birth weight. Compared to the PT group, a larger proportion of the FT group was in the highest SES group. Although fewer data were available, paternal education showed the same pattern of results. Mean IQ scores were in the average range, but significantly lower in the PT compared to FT group. Forty-one (60%) PT children received early intervention compared to no FT children. There were no differences between PT and FT groups in the number of children attending daycare, preschool, or kindergarten.
Table 1.
Participant characteristics, demographics, and IQ scores
| Preterm (n = 70) |
Full Term (n = 79) |
|||||
|---|---|---|---|---|---|---|
|
Participant Characteristicsa |
Mean (SD) | Range | Mean (SD) | Range | t or X2 | p |
| Age (years) | 4.6 (.76) | 3.0–5.9 | 4.4 (.82) | 3.1–5.9 | −1.5 | .135 |
| Perinatal Data | ||||||
| GA (weeks) | 29.6 (2.6) | 24–34 | 39.3 (1.4) | 37–42 | 27.4 | <.001* |
| Birthweight (g) | 1365 (455) | 468–2495 | 3331 (507) | 2239–4510 | 24.8 | <.001* |
| Demographicsb | Preterm | Full Term | p | |||
| Race, n (%) | .064 | .876 | ||||
| White | 42 (60) | 49 (61) | ||||
| Nonwhite | 28 (40) | 31 (39) | ||||
| Ethnicity, n (%) | 1.5 | .480 | ||||
| Nonhispanic/ Nonlatino |
47 (67) | 60 (76) | ||||
| Hispanic/Latino | 8 (11.4) | 6 (7.6) | ||||
| Mixed | 15 (21.4) | 13 (16.5) | ||||
| Gender, n (%) | 2.4 | .102 | ||||
| Male | 40 (57) | 35 (44) | ||||
| Female | 30 (43) | 45 (56) | ||||
| Maternal Education, n (%) |
5.1 | .029* | ||||
| < master’s degree |
44 (63) | 35 (45) | ||||
| ≥ master’s degree |
26 (37) | 43 (55) | ||||
| Cognitive Scores | Mean (SD) | Range | Mean (SD) | Range | t | p |
| IQa | 101.9 (15) | 73–127 | 110.2 (13) | 82–139 | 3.7 | < .001* |
| Proportionsb | ||||||
| n (%) with IQ score <85 | n (%) with IQ score <85 | X2 | p | |||
| 10 (14.3) | 1 (1.3) | 9.2 | <.001* | |||
Data analyzed by t-test
Data analyzed by chi-square (asymptotic or exact significance: 2-sided)
Group Differences
Compared to FT children, PT children had significantly higher GEC scores and lower average EF battery z-scores, indicating more EF problems. PT children had significantly lower mean scores for the Vineland Adaptive Behavior Composite and Phonologic Awareness subtest, indicating poorer function, than did FT children. The mean scores for all CBCL broadband scales were significantly higher for the PT group, compared to the FT group, indicating more behavior symptoms. Compared to FT children, there were significantly greater proportions of PT children with scores in the borderline and clinical range or below-average ranges for all measures except the TOPEL. (Table 2)
Table 2.
Group difference in executive function, functional outcomes, and behavior.
| Preterm | Full Term | ||||||
|---|---|---|---|---|---|---|---|
|
Executive Functiona |
(n = 66) | (n = 79) | |||||
| BRIEF | Mean (SD) | Range | Mean (SD) | Range | t | p | |
| Global Executive Composite (GEC) |
54.3 (15) | 31–95 | 43.5 (8) | 33–67 | −5.2 | < .001* | |
| EF Battery | (n = 70) | (n = 79) | |||||
| Z-score | −.844 (1.1) | −4.19–.6 | −.004 (.52) | −1.37–1.2 | 5.91 | <.001* | |
| Outcomesa | |||||||
| Vineland | (n = 61) | (n = 74) | |||||
| Adaptive Behavior Composite (ABC) |
97 (12.7) | 68–128 | 111 (11.6) | 79–134 | 6.91 | <.001* | |
| Test of Preschool Early Literacy |
(n = 38) | (n = 37) | |||||
| Phonological Awareness |
103 (16) | 65–129 | 112 (13) | 79–129 | 2.79 | .007* | |
| Child Behavior Checklist (CBCL) |
(n = 68) | (n = 79) | |||||
| Total | 48.6 (10.7) | 28–77 | 40.6 (7.2) | 28–62 | −5.3 | < .001* | |
| Internalizing | 48.5 (11.2) | 29–73 | 42.3 (8.3) | 29–64 | −3.8 | < .001* | |
| Externalizing | 48.2 (10.7) | 28–76 | 40.5 (8.1) | 28–65 | −4.9 | < .001* | |
| Proportionsb | X2 | p | |||||
| GEC | n (%) with T-score > 64 | n (%) with T-score > 64 | |||||
| 16 (24) | 1 (1.3) | 18.3 | < .001* | ||||
| Z-score | n (%) with score ≤ −1SD | n (%) with score ≤ −1SD | |||||
| 25 (36) | 2 (3) | 28 | <.001* | ||||
| ABC | n (%) with score <85 | n (%) with score <85 | |||||
| 10 (16.4%) | 1 (1.4%) | 10.1 | .001* | ||||
| Phonological Awareness |
n (%) with score <85 | n (%) with score <85 | |||||
| 1 (2.7%) | 5 (13.2%) | 2.8 | .095 | ||||
| CBCL | n (%) with T-score > 59 | n (%) with T-score > 59 | |||||
| Total | 11 (16.2) | 1 (1.3) | 10.8 | .001* | |||
| Internalizing | 12 (17.6) | 4 (5.1) | 6.0 | .015* | |||
| Externalizing | 9 (13.2) | 1 (1.3) | 8.3 | .004* | |||
Data analyzed by t-test
Data analyzed by chi-square (asymptotic or exact significance: 2-sided)
Correlations Among EF Measures
We used Spearman correlations to evaluate the association between the GEC score and EF battery z-score. The variables showed small but significant correlation with r = ‒.176, p = .034. Moderate to high correlations were found in the expected direction among the BRIEF-P subscales, r ranging from .38 to .83, all p < .001. (Table 3) Modest to moderate correlations were found in the expected directions among most of the performance-based EF measures, as previously reported, with r ranging from .17 to .505 (p < .05 to p < .001).35 Performance on the 6-Boxes task correlated with Inhibition, Shift, and Plan/Organize subscales on the BRIEF-P, r ranging from .17 to .24, p < .05 (Table 3). Performance on the Verbal Fluency task correlated only with the Plan/Organize subscale, r = −.25, p < .001; Bird-Dragon task with Working Memory and Plan/Organize subscales, r = −.22, p < .001, and r = −.17, p < .05, respectively; and Card Sort task with the Working Memory subscale, r = −.17, p < .05. The Day/Night task did not correlate with any BRIEF-P subscales.
Table 3.
Correlations among BRIEF-P subscales (Variables 1 through 5) and EF tasks (Variables 6 through 10)
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Inhibition | 1 | |||||||||
| 2. Shift | .376*** | 1 | ||||||||
| 3. Emotional Control |
.624*** | .520*** | 1 | |||||||
| 4. Working Memory |
.676*** | .435*** | .584*** | 1 | ||||||
| 5. Plan/Organize | .704*** | .440*** | .613*** | .827*** | 1 | |||||
| 6. 6-Boxes | .176* | .243** | .149 | .156 | .184* | 1 | ||||
| 7. Verbal Fluency | −.091 | −.153 | −.124 | −.145 | −.240** | −.245** | 1 | |||
| 8. Day/Night | .028 | −.070 | .084 | −.116 | −.070 | −.193* | .256** | 1 | ||
| 9. Bird/Dragon | −.054 | −.163 | −.112 | −.215** | −.170* | −.308*** | .505*** | .442*** | 1 | |
| 10. Dimensional Change Card Sort |
.005 | −.034 | −.039 | −.172* | −.140 | −.158 | .265** | .166* | .239** | 1 |
Note:
p < .05;
p < .01;
p < .001
Abbreviations: BRIEF-P, Behavior Rating Inventory of Executive Function-Preschool version; EF, executive function
Mediation Analyses
We first ran the total, indirect, and direct effects models, with maternal education as a covariate, for all three functional outcomes using the entire sample. Maternal education was not significant in any of the models for each of the functional outcomes, so the models were re-estimated without maternal education, and subsequent results are reported without the covariate.
For adaptive function, we first examined the “total effects” model--the contributions of GA to Adaptive Behavior Composite score, with no mediator in the model. The total effects model was significant, accounting for 26.4% of the variance in outcome, F(1, 131)= 47, p < .001; GA was significant. (Figure 2, bottom) The models predicting to the mediators of parent-rated EF and performance-based EF were also significant. GA predicted 21% of the variance in parent-rated EF, F(1, 131) = 33.9, p < .001, and 17% of the variance in performance-based EF, F(1, 131) = 27.7, p < .001. The overall model, which included both EF measures simultaneously as potential mediators, was significant, accounting for 39% of the variance in Adaptive Behavior Composite score, F(3, 129) = 27.3, p < .001. The “direct effects” model was significant (c’ in Figure 2). The “indirect effects” model was significant for gestational age on adaptive function through parent-rated EF, b = .366, CI [.14, .67], and through performance-based EF, b = .284, CI [.10, .51]. Since both mediators were significant, we conducted a comparison of indirect effects; the contrast between parent-rated EF and performance-based EF was not significant, b = .082, CI [−.24, .44], indicating no difference between the mediators in their contributions to the indirect effect.
Figure 2.
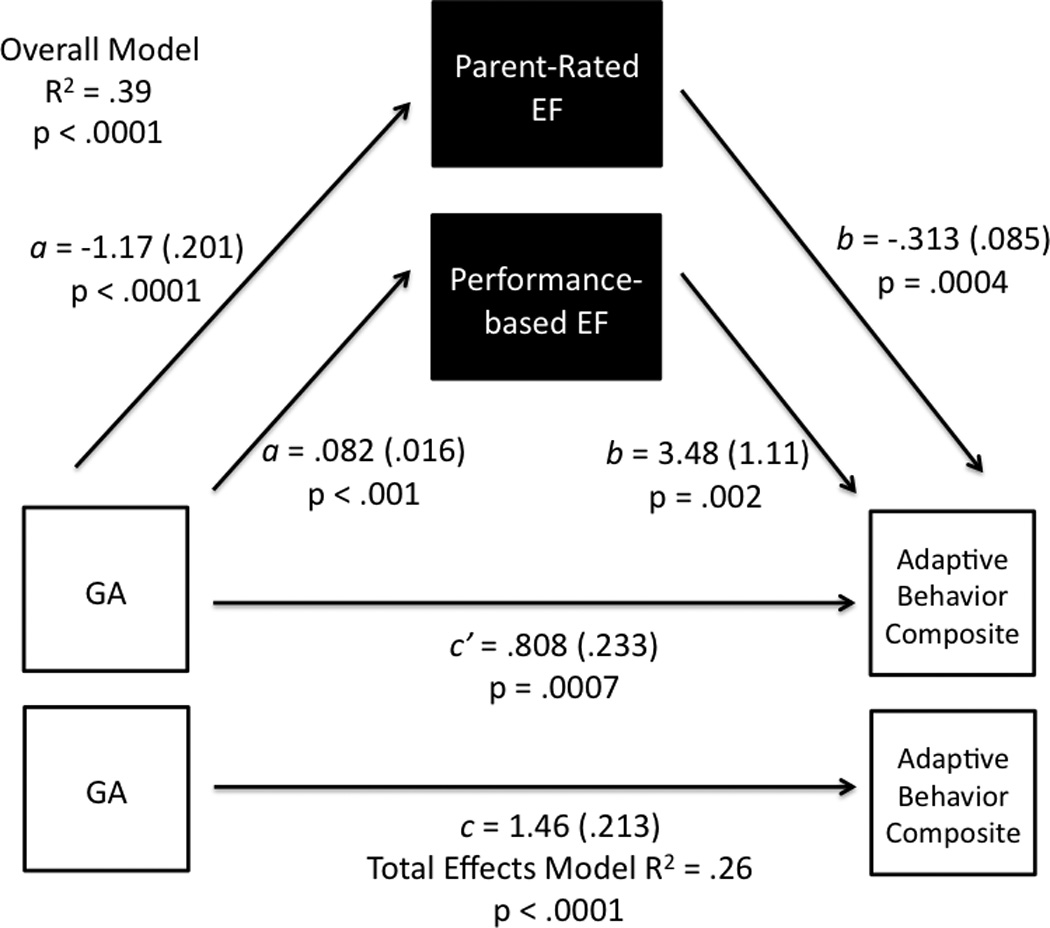
The Total Effects Model is in the lower part of the figure; the multiple mediation model in path diagram form with both parent-rated EF and performance-based EF in the model is directly above. T-statistics and significance level are presented for each path (inner values correspond to performance-based EF and outer values to parent-rated EF). Indirect effects of gestational age on the Adaptive Behavior Composite through both parent-rated and performance-based EF were significant.
For prereading skills, the total effects model evaluating the contributions of GA to Phonological Awareness score with no mediator in the model was significant, accounting for 9.8% of the variance in outcome, F(1, 70)= 7.59, p = .0075 (Figure 3, bottom). The models predicting to the mediators of parent-rated EF and performance-based EF were also significant, with GA predicting 21% of the variance in parent-rated EF, F(1, 70) = 19, p < .0001, and 19% of the variance in performance-based EF, F(1, 70) = 16.4, p = .0001. The overall model, which included both EF measures simultaneously as potential mediators, was significant, accounting for 25% of the variance in Phonological Awareness score, F(3, 68) = 7.7, p = .0002. The direct effect model was not significant (c’ in Figure 3). The indirect effect model of gestational age on prereading function was significant for performance-based EF, b = .548, CI [.24, .95], but not for parent-rated EF, b = .195, CI [−.13, .55]. Re-estimating the models with only performance-based EF as the mediator resulted in kappa-squared of .174, CI [.07, .3], or 17.4% of the maximum value, indicating a medium effect.
Figure 3.
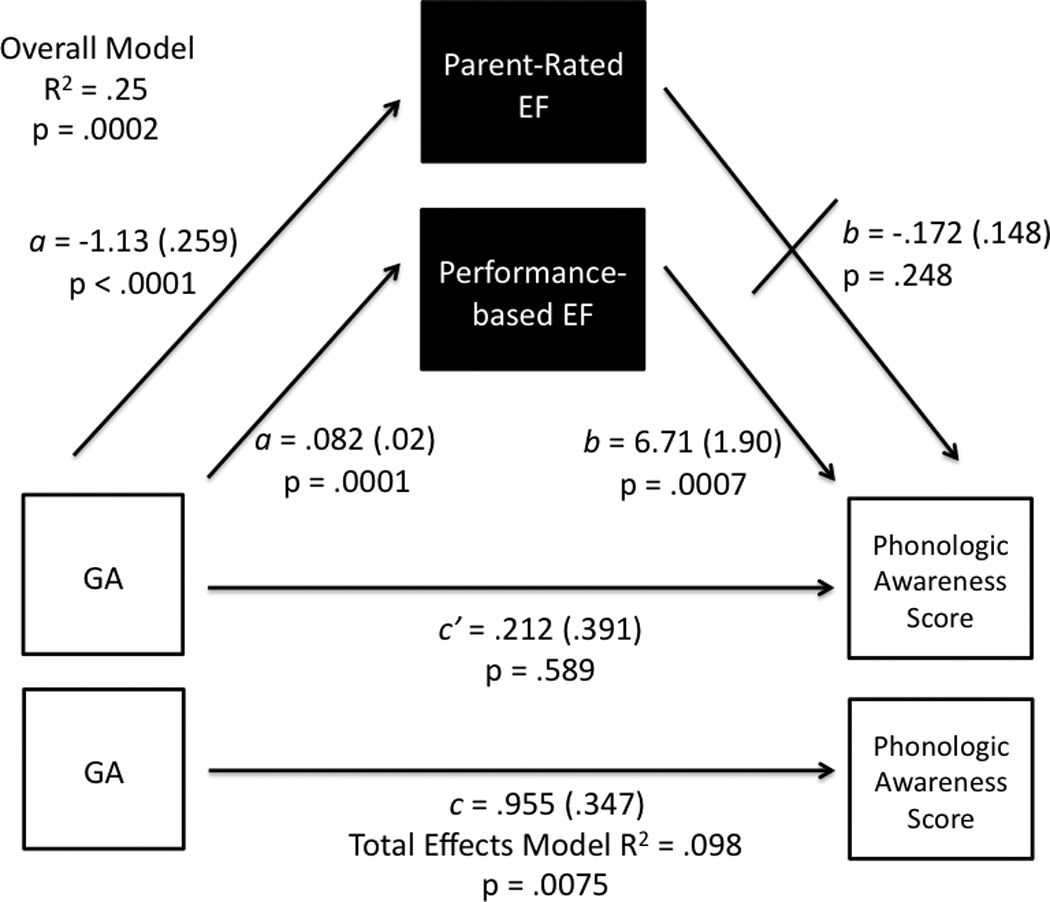
The Total Effects Model is in the lower part of the figure; the multiple mediation model in path diagram form with both parent-rated EF and performance-based EF in the model is directly above. T-statistics and significance level are presented for each path (inner values correspond to performance-based EF and outer values to parent-rated EF). Indirect effect of gestational age on the Phonologic Awareness Score through performance-based EF was significant.
For behavior symptoms, the total effects model evaluating the contributions of GA to Total Problems score with no mediator in the model was significant, accounting for 19% of the variance in outcome, F(1, 142)= 34, p < .0001 (Figure 4, bottom). The models predicting to the mediators of parent-rated EF and performance-based EF were also significant, with GA predicting 21% of the variance in parent-rated EF, F(1, 142) = 37, p < .0001, and 17% of the variance in performance-based EF, F(1, 142) = 29, p < .0001. The overall model, which included both EF measures simultaneously as potential mediators, was significant, accounting for 57% of the variance in Total Problems score, F(3, 140) = 61, p < .0001. The direct effect model was significant (c’ in Figure 4). The indirect effect model of gestational age on Total Problems score was significant for parent-rated EF, b = −.59, CI [−.87, −.37], but not for performance-based EF, b = .07, CI [−.03, .19]. Re-estimating the models with only parent-rated EF as the mediator resulted in kappa-squared of .329, CI [.23, .44], or 32.9% of the maximum value, indicating a large effect.
Figure 4.
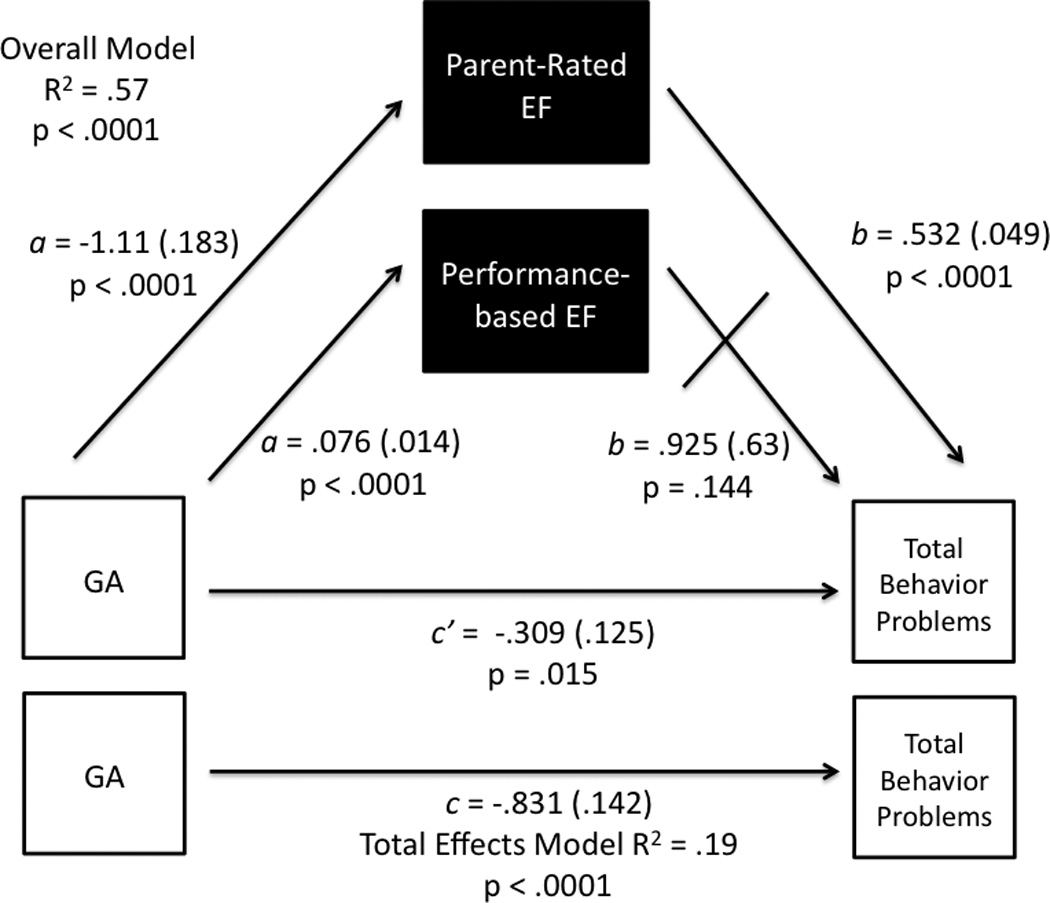
The Total Effects Model is in the lower part of the figure; the multiple mediation model in path diagram form with both parent-rated EF and performance-based EF in the model is directly above. T-statistics and significance level are presented for each path (inner values correspond to performance-based EF and outer values to parent-rated EF). Indirect effect of gestational age on the Total Behavior Problems score through parent-rated EF was significant.
**p significant at <.05
Abbreviations: GA, gestational age; EF, executive function
DISCUSSION
We confirmed our first hypothesis -- PT preschoolers had lower adaptive function and prereading skills and more behavior symptoms than did FT preschoolers. For the entire sample, we also confirmed our second hypothesis -- after accounting for socioeconomic status using maternal education, GA contributed to all three functional outcomes. In addition, GA contributed to both parent-rated and performance-based EF. Finally, our third hypothesis was confirmed -- mediation analyses revealed that EF was a significant mediator of the effects of GA on all three outcomes, although different patterns emerged for parent-rated and performance-based EF. For adaptive function, both parent-reported and performance-based EF measures significantly mediated effects of GA; for prereading skills, only performance-based EF was significant; and, for behavior symptoms, only parent-rated EF was significant.
Our study went beyond the typical outcome studies that focus on independent associations of adverse outcomes and preterm birth because we used an updated mediation model that has several advantages over past mediation methods. Only a few studies using mediation have been conducted in the preterm population, and focused, at most, on two outcomes.15, 19 We included three functional outcomes in the same study, allowing for a comprehensive examination of the role of both parent-rated EF and performance-based EF as mediators of outcome. Given the associations of EF with functional outcomes and behavior symptoms, evaluation of EF at young ages offers the opportunity to identify children at increased risk for later impaired function and possibly to intervene to improve outcomes.
Our finding of EF as a significant mediator of adaptive function is consistent with two studies of school-age preterm children that found that performance-based EF mediated adaptive skills measured by the Vineland15 or the CBCL Total Competence score, a composite measure of quantity and quality of child participation in home, school, and social activities.19 However, those studies did not include parent-rated EF in the models. Our findings are also consistent with other studies of clinical populations, including children with autism spectrum disorder (ASD) and externalizing behaviors, although these studies did not use mediation. One study of children with ASD found that parent-rated EF on the BRIEF was negatively correlated with most domains of adaptive function on the Vineland; this study did not include performance-based EF.16 Another study of children with high-functioning ASD and children with attention-deficit/hyperactivity disorder (ADHD) also found negative correlations between performance-based EF and subdomains of adaptive function on the Vineland.57 A study of adolescents with externalizing behaviors, including ADHD, oppositional-defiant disorder, and conduct disorder, found that performance-based EF skills predicted variance in overall adaptive function as measured by the Vineland, but did not gather parent-rated EF measures.17 In our study, whether measured by parent report or direct assessment, EF functioned as a significant mediator of adaptive function.
Our finding that performance-based EF mediated effects of gestational age on prereading skills is consistent with other mediation studies in typical children as well as school age or adolescent preterm children. Longitudinal studies of typical children showed that EF skills at preschool age were related to math and literacy abilities in kindergarten3, 4 and predicted math and reading achievement at age 7.20 Complex memory performance at age 5 predicted performance on measures of language, mathematics and literacy at age 8.24 Using structural equation modeling, Rose and colleagues found that the negative effects of prematurity on math and reading achievement in preterm 11-year olds was mediated by slower processing speed and performance-based EF.28 Two studies that focused on both adaptive function and academic outcomes found that performance-based EF mediated the effects of neonatal risk on academic achievement15 and the effects of GA on reading.19 Other studies of preterm children confirm links between performance-based EF and academic domains, such as math29 and reading,26, 27 but did not use mediation. A study of 9–10 year old children born very preterm found that processing speed, working memory, and birth group status were significant predictors of overall academic achievement as rated by teacher questionnaire.25
Our finding of parent-rated EF as a significant mediator of behavior symptoms or problems is consistent with Nadeau and colleagues, who found that sequential memory, an EF skill, mediated the effects of GA on inattention at 9–10 years of age.34 Other mediation studies examined only intellectual ability and not EF.32, 33 There are topically related studies of children born preterm that have examined the contributions of cognitive skills, including EF skills and general intellectual ability, to behavior problems or disorders including ADHD;58–60 however, these studies used regression model analytic approaches.
Our results showed different patterns for parent-rated and performance-based EF mediation of the effect of gestational age on functional outcomes and behavior symptoms. We previously reported on the associations between parent-rated and performance-based EF in this sample, and similar to other studies of typical and clinical populations, we found statistically significant correlations between some, but not all, EF constructs.35 In some studies, EF measurements correlate, but are not aligned (i.e., a parent rating for one EF construct correlates with a different EF construct).1, 61, 62 In other studies, correlations among measures are not significant63 or are only modest in magnitude.61 Explanations for the discrepancy between parent-rated EF and performance-based EF highlight differences in ecological validity between the two approaches. Parent ratings provide a global view of children’s behavior in everyday environments, and therefore may represent an ecologically valid assessment of EF skills in the context of naturalistic settings. However, parents also have emotional involvement with the children and their ratings may represent global impressions beyond the specific EF measure under consideration, explaining the relatively high intercorrelations. Performance-based measures attempt to isolate EF constructs and get a “pure” measurement in a distraction-free, one-on-one setting. The scores on these tasks are modestly to moderately correlated, indicating that the tasks may not be assessments of a pure ability or that the abilities themselves are overlapping. Though the performance-based measures are collected in the laboratory, ecological validity refers not only to how well an assessment captures behavior in a natural environment, but also to how well the assessment predicts individuals’ functional outcomes.64 Our findings, that both parent-rated and performance-based EF acted as mediators of relevant functional outcomes, suggest that both types of measures are ecologically valid, despite the modest or limited correlations among individual EF constructs measured by parent ratings or direct observation.
The study had limitations. The mean SES of the sample was high, consistent with the geographic area, and the results may not be representative of PT and FT populations with lower SES. Nonetheless, even with the resources and access to services accompanying higher SES, the PT children in our study demonstrated impairments in EF; lower IQ, adaptive and prereading skills; and more behavior symptoms compared to FT children. We did not conduct diagnostic interview to confirm behavior disorders. We recognize that EF measures may correlate with other factors; future research might address such factors including child brain function as elucidated by imaging techniques, parenting style, or parent knowledge of child development. We focused on EF skill as a potential mediator, as opposed to other domains of function or IQ, because we believe that EF is a potential target for intervention. Given the significant correlations between IQ and EF measures, we suspect that IQ might also serve as a mediator. However, IQ is a broad construct that is unlikely to serve as an intervention target. We had cross-sectional data, not longitudinal data, hence the mediation demonstrated is statistical. Future longitudinal work may clarify the relationships among EF skills and functional outcomes over time. The use of parent ratings for both behavior symptoms and EF raises concern for rater bias contributing to a significant mediation relationship. However, we had direct measurement of some variables, such as performance-based EF and TOPEL Phonological Awareness (for half of the sample); this lessens the likelihood that the observed relationships are based on shared response bias alone. Future work will include ratings from a second, non-parent informant, such as teacher or daycare provider reports, to decrease rater bias and will augment the direct observation or standardized assessment of additional functional outcomes.
CONCLUSION
Executive function mediated the effect of GA on adaptive function, prereading skills, and behavior symptoms. Parent-rated and performance-based EF behaved differently in each of the models, and both measures of EF served as unique mediators for adaptive function, raising important questions about the assessment of EF. The findings suggest that measures of EF, whether gathered by parent-report or directly, are tapping into related, but not completely overlapping constructs.35 We previously proposed standard assessment of EF in young children born preterm.35 Parent ratings of EF can be obtained in the pediatric office and provide a practical description of children’s EF strengths and difficulties in everyday environments. Additional monitoring and EF evaluation in children born preterm are warranted. EF skills are measurable in young children, mediate important functional outcomes, and are potentially malleable. Our future work will focus on targeted intervention for EF skills and whether such intervention may influence long-term outcomes.
Acknowledgements
We thank the children and families who participated in our study. Special thanks to Maya Chatav and Walter S. Chang for assistance with data collection and to Nidia Alduncin for assistance with data collection and manuscript figures.
Funding Sources: This work was supported by the Lucile Packard Foundation for Children’s Health under a Pilot Early Career Grant, the Society for Developmental-Behavioral Pediatrics under the Young Investigator Award, and the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, under the Mentored Patient-oriented Research Career Development Award Grant K23HD071971 to Irene M. Loe; and the National Center for Research Resources, National Institutes of Health under the Stanford Clinical and Translational Science Award 1UL1 RR025744.
Abbreviations
- ADHD
attention-deficit/hyperactivity disorder
- ASD
autism spectrum disorder
- BRIEF
Behavior Rating Inventory of Executive Function
- BW
birth weight
- CBCL
Child Behavior Checklist
- EF
executive function
- FT
full term
- GA
gestational age
- GEC
global executive composite
- IQ
intelligence quotient
- PT
preterm
- SD
standard deviation
- SES
socioeconomic status
Footnotes
Financial Disclosure: The authors have no financial relationships relevant to this article to disclose.
Conflict of Interest: The authors have no conflict of interest relevant to this article to disclose.
REFERENCES
- 1.Anderson P. Assessment and development of executive function (EF) during childhood. Child Neuropsychol. 2002;8:71–82. doi: 10.1076/chin.8.2.71.8724. [DOI] [PubMed] [Google Scholar]
- 2.Miyake A, Friedman NP, Emerson MJ, et al. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognit Psychol. 2000;41:49–100. doi: 10.1006/cogp.1999.0734. [DOI] [PubMed] [Google Scholar]
- 3.Blair C, Razza RP. Relating effortful control, executive function, and false belief understanding to emerging math and literacy ability in kindergarten. Child Dev. 2007;78:647–663. doi: 10.1111/j.1467-8624.2007.01019.x. [DOI] [PubMed] [Google Scholar]
- 4.Cameron CE, Brock LL, Murrah WM, et al. Fine motor skills and executive function both contribute to kindergarten achievement. Child Dev. 2012;83:1229–1244. doi: 10.1111/j.1467-8624.2012.01768.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Diamantopoulou S, Rydell AM, Thorell LB, et al. Impact of executive functioning and symptoms of attention deficit hyperactivity disorder on children’s peer relations and school performance. Dev Neuropsychol. 2007;32:521–542. doi: 10.1080/87565640701360981. [DOI] [PubMed] [Google Scholar]
- 6.Volpe JJ. Brain injury in premature infants: a complex amalgam of destructive and developmental disturbances. Lancet Neurol. 2009;8:110–124. doi: 10.1016/S1474-4422(08)70294-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Woodward LJ, Clark CA, Pritchard VE, et al. Neonatal white matter abnormalities predict global executive function impairment in children born very preterm. Dev Neuropsychol. 2011;36:22–41. doi: 10.1080/87565641.2011.540530. [DOI] [PubMed] [Google Scholar]
- 8.Durston S, Casey B. What have we learned about cognitive development from neuroimaging? Neuropsychologia. 2006;44:2149–2157. doi: 10.1016/j.neuropsychologia.2005.10.010. [DOI] [PubMed] [Google Scholar]
- 9.Luna B, Padmanabhan A, O’Hearn K. What has fMRI told us about the development of cognitive control through adolescence? Brain Cogn. 2010;72:101–113. doi: 10.1016/j.bandc.2009.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Warren SL, Crocker LD, Spielberg JM, et al. Cortical organization of inhibition-related functions and modulation by psychopathology. Frontiers in Human Neuroscience. 2013;7:271. doi: 10.3389/fnhum.2013.00271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aarnoudse-Moens CSH, Weisglas-Kuperus N, van Goudoever JB, et al. Meta-Analysis of Neurobehavioral Outcomes in Very Preterm and/or Very Low Birth Weight Children. Pediatr. 2009;124:717–728. doi: 10.1542/peds.2008-2816. [DOI] [PubMed] [Google Scholar]
- 12.Mulder H, Pitchford NJ, Hagger MS, et al. Development of Executive Function and Attention in Preterm Children: A Systematic Review. Dev Neuropsychol. 2009;34:393–421. doi: 10.1080/87565640902964524. [DOI] [PubMed] [Google Scholar]
- 13.Aylward GP. Neurodevelopmental outcomes of infants born prematurely. J Dev& Behav Pediatr. 2005;26:427–440. doi: 10.1097/00004703-200512000-00008. [DOI] [PubMed] [Google Scholar]
- 14.Johnson S, Marlow N. Preterm Birth and Childhood Psychiatric Disorders. Pediatr Res. 2011;69:11R–18R. doi: 10.1203/PDR.0b013e318212faa0. [DOI] [PubMed] [Google Scholar]
- 15.Taylor HG, Klein N, Drotar D, et al. Consequences and risks of <1000-g birth weight for neuropsychological skills, achievement, and adaptive functioning. J Dev Behav Pediatr. 2006;27:459–469. doi: 10.1097/00004703-200612000-00002. [DOI] [PubMed] [Google Scholar]
- 16.Gilotty L, Kenworthy L, Sirian L, et al. Adaptive skills and executive function in autism spectrum disorders. Child Neuropsychol. 2002;8:241–248. doi: 10.1076/chin.8.4.241.13504. [DOI] [PubMed] [Google Scholar]
- 17.Clark C, Prior M, Kinsella G. The relationship between executive function abilities, adaptive behaviour, and academic achievement in children with externalising behaviour problems. J Child Psychol and Psychiatry. 2002;43:785–796. doi: 10.1111/1469-7610.00084. [DOI] [PubMed] [Google Scholar]
- 18.Cahn-Weiner DA, Boyle PA, Malloy PF. Tests of executive function predict instrumental activities of daily living in community-dwelling older individuals. Appl Neuropsychol. 2002;9:187–191. doi: 10.1207/S15324826AN0903_8. [DOI] [PubMed] [Google Scholar]
- 19.Loe IM, Lee ES, Luna B, et al. Executive function skills are associated with reading and parent-rated child function in children born prematurely. Early Hum Dev. 2012;88:111–118. doi: 10.1016/j.earlhumdev.2011.07.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bull R, Scerif G. Executive functioning as a predictor of children’s mathematics ability: Inhibition, switching, and working memory. Dev Neuropsychol. 2001;19:273–293. doi: 10.1207/S15326942DN1903_3. [DOI] [PubMed] [Google Scholar]
- 21.Gathercole SE, Pickering SJ, Gathercole SE, et al. Working memory deficits in children with low achievements in the national curriculum at 7 years of age. Br J Educ Psychol. 2000;70:177–194. doi: 10.1348/000709900158047. [DOI] [PubMed] [Google Scholar]
- 22.St Clair-Thompson HL, Gathercole SE. Executive functions and achievements in school: Shifting, updating, inhibition, and working memory. Q J Exp Psychol. 2006;59:745–759. doi: 10.1080/17470210500162854. [DOI] [PubMed] [Google Scholar]
- 23.Clark CA, Pritchard VE, Woodward LJ. Preschool executive functioning abilities predict early mathematics achievement. Dev Psychol. 2010;46:1176–1191. doi: 10.1037/a0019672. [DOI] [PubMed] [Google Scholar]
- 24.Gathercole SE, Tiffany C, Briscoe J, et al. Developmental consequences of poor phonological short-term memory function in childhood: a longitudinal study. J Child Psychol Psychiatry. 2005;46:598–611. doi: 10.1111/j.1469-7610.2004.00379.x. [DOI] [PubMed] [Google Scholar]
- 25.Mulder H, Pitchford NJ, Marlow N. Processing speed and working memory underlie academic attainment in very preterm children. Archives of Disease in Childhood Fetal & Neonatal Edition. 2010:95. doi: 10.1136/adc.2009.167965. [DOI] [PubMed] [Google Scholar]
- 26.Downie ALS, Frisk V, Jakobson LS. The Impact of Periventricular Brain Injury on Reading and Spelling Abilities in the Late Elementary and Adolescent Years. Child Neuropsychol. 2005;11:479–495. doi: 10.1080/09297040591001085. [DOI] [PubMed] [Google Scholar]
- 27.Frye RE, Landry SH, Swank PR, et al. Executive dysfunction in poor readers born prematurely at high risk. Dev Neuropsychol. 2009;34:254–271. doi: 10.1080/87565640902805727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rose SA, Feldman JF, Jankowski JJ. Modeling a cascade of effects: the role of speed and executive functioning in preterm/full-term differences in academic achievement. Dev Sci. 2011;14:1161–1175. doi: 10.1111/j.1467-7687.2011.01068.x. [DOI] [PubMed] [Google Scholar]
- 29.Aarnoudse-Moens CS, Weisglas-Kuperus N, Duivenvoorden HJ, et al. Executive Function and IQ Predict Mathematical and Attention Problems in Very Preterm Children. PLoS ONE. 2013;8:e55994. doi: 10.1371/journal.pone.0055994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Brocki KC, Eninger L, Thorell LB, et al. Interrelations between executive function and symptoms of hyperactivity/impulsivity and inattention in preschoolers: a two year longitudinal study. J Abnorm Child Psychol. 2010;38:163–171. doi: 10.1007/s10802-009-9354-9. [DOI] [PubMed] [Google Scholar]
- 31.Wahlstedt C, Thorell LB, Bohlin G. ADHD symptoms and executive function impairment: early predictors of later behavioral problems. Dev Neuropsychol. 2008;33:160–178. doi: 10.1080/87565640701884253. [DOI] [PubMed] [Google Scholar]
- 32.Conrad AL, Richman L, Lindgren S, et al. Biological and environmental predictors of behavioral sequelae in children born preterm. Pediatr. 2010;125:e83–e89. doi: 10.1542/peds.2009-0634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Loe IM, Lee ES, Luna B, et al. Behavior problems of 9–16 year old preterm children: Biological, sociodemograhic, and intellectual contributions. Early Hum Dev. 2011;87:247–252. doi: 10.1016/j.earlhumdev.2011.01.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nadeau L, Boivin M, Tessier R, et al. Mediators of behavioral problems in 7-year-old children born after 24 to 28 weeks of gestation. J Dev Behav Pediatr. 2001;22:1–10. doi: 10.1097/00004703-200102000-00001. [DOI] [PubMed] [Google Scholar]
- 35.Loe IM, Chatav M, Alduncin N. Complementary Assessment of Executive Function in Preterm and Full Term Preschoolers. Child Neuropsychol. doi: 10.1080/09297049.2014.906568. Published online April 22, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Roid GH. Stanford-Binet Intelligence Scales. Fifth Edition. Itasca, IL: Riverside Publishing; 2003. [Google Scholar]
- 37.Gioia GA, Isquith PK, Guy SC, et al. Behavior Rating Inventory of Executive Function-Preschool Version (BRIEF-P) Odessa, FL: Psychological Assessment Resources, Inc; 2002. [Google Scholar]
- 38.Gioia GA, Isquith PK, Retzlaff PD, et al. Confirmatory factor analysis of the Behavior Rating Inventory of Executive Function (BRIEF) in a clinical sample. Child Neuropsychol. 2002;8:249–257. doi: 10.1076/chin.8.4.249.13513. [DOI] [PubMed] [Google Scholar]
- 39.Aarnoudse-Moens CS, Smidts DP, Oosterlaan J, et al. Executive function in very preterm children at early school age. J Abnorm Child Psychol. 2009;37:981–993. doi: 10.1007/s10802-009-9327-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Carlson SM. Developmentally sensitive measures of executive function in preschool children. Dev Neuropsychol. 2005;28:595–616. doi: 10.1207/s15326942dn2802_3. [DOI] [PubMed] [Google Scholar]
- 41.Garon N, Bryson SE, Smith IM, et al. Executive function in preschoolers: a review using an integrative framework. Psychol Bull. 2008;134:31–60. doi: 10.1037/0033-2909.134.1.31. [DOI] [PubMed] [Google Scholar]
- 42.Landry SH, Smith KE, Swank PR, et al. Early maternal and child influences on children’s later independent cognitive and social functioning. Child Dev. 2000;71:358–375. doi: 10.1111/1467-8624.00150. [DOI] [PubMed] [Google Scholar]
- 43.Lezak MD, Howieson DW, Loring DW. Neuropsychological Assessment. 4 ed. New York, NY: Oxford University Press; 2004. [Google Scholar]
- 44.Gerstadt CL, Hong YJ, Diamond A. The relationship between cognition and action: performance of children 3 1/2–7 years old on a Stroop-like day-night test. Cognition. 1994;53:129–153. doi: 10.1016/0010-0277(94)90068-x. [DOI] [PubMed] [Google Scholar]
- 45.Carlson SM, Moses LJ. Individual differences in inhibitory control and children’s theory of mind. Child Dev. 2001;72:1032–1053. doi: 10.1111/1467-8624.00333. [DOI] [PubMed] [Google Scholar]
- 46.Reed MA, Pien DL, Rothbart MK. Inhibitory self-control in preschool children. Merrill-Palmer Quarterly. 1984;30:131–147. [Google Scholar]
- 47.Zelazo PD. The Dimensional Change Card Sort (DCCS): a method of assessing executive function in children. Nat Protoc. 2006;1:297–301. doi: 10.1038/nprot.2006.46. [DOI] [PubMed] [Google Scholar]
- 48.Lee K, Bull R, Ho RMH. Developmental changes in executive functioning. Child Dev. 2013:1–21. doi: 10.1111/cdev.12096. [DOI] [PubMed] [Google Scholar]
- 49.Sparrow SS, Balla DA, Cicchetti D. Vineland Adaptive Behavior Scales. Second Edition. Bloomington, MN: Pearson Assessments; 2005. [Google Scholar]
- 50.Lonigan CJ, Wagner RK, Torgeson JK, et al. Test of preschool early literacy. Austin, TX: ProEd; 2007. [Google Scholar]
- 51.Achenbach TM, Rescorla LA. Manual for ASEBA Preschool Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families; 2000. [Google Scholar]
- 52.Hayes AF, Preacher KJ. Statistical Mediation Analysis with a Multicategorical Independent Variable. 2012 doi: 10.1111/bmsp.12028. [DOI] [PubMed] [Google Scholar]
- 53.Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51 doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 54.Hayes AF. Beyond Baron and Kenny: Statistical mediation analysis in the new millenium. Communication Monographs. 2009;76:408–420. [Google Scholar]
- 55.Field A. Discovering Statistics Using IBM SPSS Statistics. 4 ed. Los Angeles: Sage Publications Inc; 2013. [Google Scholar]
- 56.Preacher KJ, Kelley K. Effect size measures for mediation models: Quantitative strategies for communicating indirect effects. Psychol Methods. 2011;16:93–115. doi: 10.1037/a0022658. [DOI] [PubMed] [Google Scholar]
- 57.Happe F, Booth R, Charlton R, et al. Executive function deficits in autism spectrum disorders and attention-deficit/hyperactivity disorder: examining profiles across domains and ages. Brain Cognit. 2006;61:25–39. doi: 10.1016/j.bandc.2006.03.004. [DOI] [PubMed] [Google Scholar]
- 58.Mulder H, Pitchford NJ, Marlow N. Inattentive Behavior is Assoicated with Poor Working Memory and Slow Processing Speed in Very Pre-term Children in Middle Childhood. Br J Educ Psychol. 2011:81. doi: 10.1348/000709910X505527. [DOI] [PubMed] [Google Scholar]
- 59.Scott MN, Taylor HG, Fristad MA, et al. Behavior disorders in extremely preterm/extremely low birth weight children in kindergarten. J Dev Behav Pediatr. 2012;33:202–213. doi: 10.1097/DBP.0b013e3182475287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Samara M, Marlow N, Wolke D, et al. Pervasive Behavior Problems at 6 Years of Age in a Total-Population Sample of Children Born at <=25 Weeks of Gestation. Pediatr. 2008;122:562–573. doi: 10.1542/peds.2007-3231. [DOI] [PubMed] [Google Scholar]
- 61.Payne JM, Hyman SL, Shores EA, et al. Assessment of executive function and attention in children with neurofibromatosis type 1: relationships between cognitive measures and real-world behavior. Child Neuropsychol. 2011;17:313–329. doi: 10.1080/09297049.2010.542746. [DOI] [PubMed] [Google Scholar]
- 62.Toplak ME, Bucciarelli SM, Jain U, et al. Executive functions: performance-based measures and the behavior rating inventory of executive function (BRIEF) in adolescents with attention deficit/hyperactivity disorder (ADHD) Child Neuropsychol. 2009;15:53–72. doi: 10.1080/09297040802070929. [DOI] [PubMed] [Google Scholar]
- 63.Mahone EM, Hoffman J. Behavior ratings of executive function among preschoolers with ADHD. Clinical Neuropsychologist. 2007;21:569–586. doi: 10.1080/13854040600762724. [DOI] [PubMed] [Google Scholar]
- 64.Silver CH. Sources of data about children’s executive functioning: Review and commentary. Child Neuropsychol. 2014;20:1–13. doi: 10.1080/09297049.2012.727793. [DOI] [PubMed] [Google Scholar]