

Abstract
Objectives:
To prevent accidental ingestion of implant hex dive.
Materials and Methods:
Dental floss which is used to stabilize the hex drive is tied to the operator's finger ring to overcome sudden aspiration of fallen instrument.
Results:
It showed excellent grip of the instrument during stage two uncover time and also saved operators time.
Conclusions:
Accidental aspiration or swallowing of the dental instruments during routine implant surgeries can be prevented by tying the implant instruments to the operator's ring with silk ligatures or dental floss.
Keywords: Accidental ingestion, aspiration, dental floss, foreign body, implant recovery, prevention
INTRODUCTION
Ingestion of dentures and small orthodontic appliances accounts for major share of accidental swallowing by normal adults. The aspirated or swallowed objects pass through two routes, either through food passage or air way passage.
During endodontic procedures, even though the incidence of ingestion of dental instruments is more than that of aspiration (0.12 and 0.0001, respectively), these aspirated patients require more frequent hospitalization. Fatal outcomes have not been reported.[1] In fixed prosthodontic practice, aspiration of single full veneer crowns and temporaries is common problem during cementation.[2]
Dental implant procedure comprises two surgical phases. In the first stage of implant placement, osteotomy is done at the implant receptor site and the implant is placed into the receptor bed and the cover screw placed. Then the flap is stabilized with sutures and is allowed to osseointegrate for the next 3-6 months. During the second stage of surgery, the cover screw is removed and an abutment or transfer coping is attached with the help of implant hex drive. It is the responsibility of the operator to see that none of the working instruments fall into the patient's throat, especially when the working area is the posterior maxillary arch. This can be achieved by various isolation procedures like using rubber dam, cotton gauge, or silk ligatures like dental floss.[3,4,5] Literature reports describe mainly the treatment options for preventing ingestion of sharp and blunt objects during routine dental procedures, but not the prevention of swallowing or aspiration of components used during implant placement.[6] In this article, a new simplified procedure is described to secure the implant hex drive using dental floss.
MATERIALS AND METHODS
Implant hex drive (Tapered Screw-Vent Surgical Kit; Zimmer, Carlsbad, CA, United States) is tied with a dental floss (Thermoseal floss; ICPA, Gujarat, India) through the access hole or channel provided by the manufacturer. The practitioner must have a gold or silver ring worn on one of his gloved fingers that has to be sterilized before wearing, to which the other end of the floss is now tied [Figure 1a and 1b]. The hex drive is ready to be placed in the receptor site for stage two uncover. This is usually done by manual reverse torque [Figure 2a]. During the procedure, if there is any accidental fall of the implant hex drive, the practitioner pulls his hand away from the patient's mouth as an immediate response and the implant hex drive comes out along with the tied floss even before entering the esophagus or trachea or even before touching the soft palate that triggers the gag reflex[7] [Figure 2b].
Figure 1.
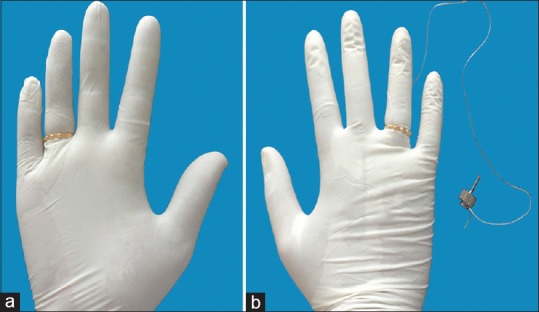
(a) Gold ring in position on the operator's hand. (b) Intact hex drive to operator's hand by using dental floss
Figure 2.
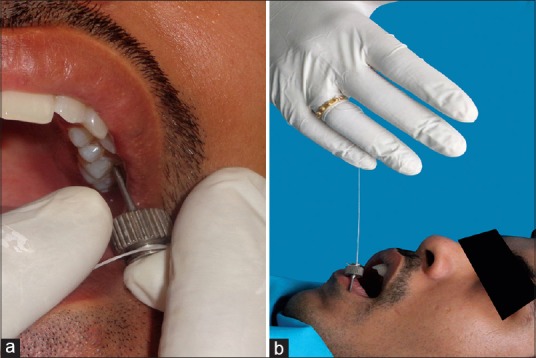
(a) Tying the hex drive manually to remove the implant cover screw by using dental floss. (b) Easy removal of the fallen instrument from the patient's mouth
DISCUSSION
During the dental implant procedure, ingestion of any instrument leads to serious complications. To prevent such accidental ingestions, standard practice guidelines need to be followed such as the use of gauze throat screens or floss ligatures.[8]
When any instrument is ingested, the clinical signs and symptoms are evident with immediate reactions like dysphasia, abdominal pain, retrosternal discomfort, and pain. In implant procedures, usually application of rubber dam is not followed, which causes frequent ingestion of dental implant objects without the knowledge of the patient or the operator and even without any clinical signs. So, for preventing these conditions, it is always better to count the instruments before the start of procedures and recount at the end of the procedures.
Complete prevention of ingestion or aspiration of any small dental object is not possible. Accidental ingestion of dental instruments may sometimes cause serious complications if not retrieved. Implant treatment has high success rates, yet severe complications may arise if proper knowledge of managing the situation is lacking.[9,10] The technique described above gives us an advantage of preventing the accidental aspiration or swallowing during implant surgical procedures. This technique decreases the search time for holding the dental floss which is usually placed with free end on to the outside of oral cavity.
When the patient aspirates or swallows any dental instrument during the operative procedure, the dentist gets into a panic to search for the other end of the floss that hangs out from the patient's mouth. To hold it tightly and remove it with ease becomes a problem, as searching and holding the floss and removing it wastes time. By then, the patient completely swallows the instrument. The diagnostic method employed to locate the aspirated or ingested metal objects is serial X-ray evaluation. Radiographs help to localize the site, obstruction, progression, and passage of the swallowed object. If the object is radiolucent, it is better to go for computed tomography (CT) scan as the ideal modality of evaluation.[11] Managing of the floss to remove the hex drive immediately from the oral cavity even reduces the operator's confusion for searching the free end of the floss. It is advised to use a gold or silver ring because they are autoclavable, reusable, and are corrosive resistant, thus preventing contamination to the patient, practitioner, as well as to the dental instruments.
Finally, if an accidental event occurs, it is better for the operator to remain calm and composed, and then reassuring the patient is the most important. Immediate pain followed by vomiting should alert the operator for possible impaction or perforation. It requires immediate evaluation and intervention. If ingestion happens, it is better to go for thorough clinical and radiological evaluation.
Endoscopy has proved to be the best and safe and effective mode of management of swallowed objects. Hence, while referring a patient for further management, it is advisable to send the replica of swallowed object so that the treating doctor will have an idea of the size, shape, and contour of the swallowed object. This helps the doctor to choose appropriate instrument for removal. Laxatives are of no proven use and may actually increase the chances of perforation.[12]
CONCLUSION
Accidental aspiration or swallowing of the dental instruments during routine implant surgeries can be prevented by tying the implant instruments and the operator's ring with silk ligatures or floss, so as to quickly recover them if they fall from the working position into the patient's mouth.
ACKNOWLEDGMENT
Financial interests, direct or indirect, for any of the authors do not exist for this article. Sources of outside support of the project are none for this article.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Susini G, Pommel L, Camps J. Accidental ingestion and aspiration of root canal instruments and other dental items in a French population. Int Endod J. 2007;40:585–9. doi: 10.1111/j.1365-2591.2007.01249.x. [DOI] [PubMed] [Google Scholar]
- 2.Kürkciyan I, Frossard M, Kettenbach J, Meron G, Sterz F, Röggla M, et al. Conservative management of foreign bodies in the gastrointestinal tract. Z Gastroenterol. 1996;34:173–7. [PubMed] [Google Scholar]
- 3.Adell R, Eriksson B, Lekholm U, Brånemark PI, Jemt T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants. 1990;5:347–59. [PubMed] [Google Scholar]
- 4.Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10:387–416. doi: 10.1016/s0300-9785(81)80077-4. [DOI] [PubMed] [Google Scholar]
- 5.Bergermann M, Donald PJ, aWengen DF. Screwdriver aspiration. A complication of dental implant placement. Int J Oral Maxillofac Surg. 1992;21:339–41. doi: 10.1016/s0901-5027(05)80757-x. [DOI] [PubMed] [Google Scholar]
- 6.Dhandapani RG, Kumar S, O’Donnell ME, McNaboe T, Cranley B, Blake G. Dental root canal treatment complicated by foreign body ingestion: A case report. Cases J. 2009;2:117. doi: 10.1186/1757-1626-2-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zitzmann NU, Elsasser S, Fried R, Marinello CP. Foreign body ingestion and aspiration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:657–60. doi: 10.1016/s1079-2104(99)70004-1. [DOI] [PubMed] [Google Scholar]
- 8.Tiwana KK, Morton T, Tiwana PS. Aspiration and ingestion in dental practice: A 10-year institutional review. J Am Dent Assoc. 2004;135:1287–91. doi: 10.14219/jada.archive.2004.0404. [DOI] [PubMed] [Google Scholar]
- 9.Buser D, von Arx T, ten Bruggenkate C, Weingart D. Basic surgical principles with ITI implants. Clin Oral Implants Res. 2000;11(Suppl 1):59–68. doi: 10.1034/j.1600-0501.2000.011s1059.x. [DOI] [PubMed] [Google Scholar]
- 10.Wennström JL, Ekestubbe A, Gröndahl K, Karlsson S, Lindhe J. Implant supported single-tooth restorations: A 5-year prospective study. J Clin Periodontol. 2005;32:567–74. doi: 10.1111/j.1600-051X.2005.00715.x. [DOI] [PubMed] [Google Scholar]
- 11.Chung YS, Chung YW, Moon SY, Yoon SM, Kim MJ, Kim KO, et al. Toothpick impaction with sigmoid colon pseudodiverticulum formation successfully treated with colonoscopy. World J Gastroenterol. 2008;14:948–50. doi: 10.3748/wjg.14.948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Henderson CT, Engel J, Schlesinger P. Foreign body ingestion: Review and suggested guidelines for management. Endoscopy. 1987;19:68–71. doi: 10.1055/s-2007-1018238. [DOI] [PubMed] [Google Scholar]