

Abstract
Aortic dissection is a rare but life-threatening complication that can occur during percutaneous coronary intervention procedures. We present a case of a 55-year-old woman who underwent a right coronary angioplasty that was complicated by a proximal dissection of the ascending aorta. Urgent surgical repair of the aorta was performed and the patient was discharged in stable clinical condition.
Background
Coronary artery dissection is a recognised complication of coronary intervention. Most dissections are small, have a benign course and are detected by angiography in 20–40% of cases.1
Aortic dissection is a life-threatening condition defined by separation of layers of the aortic wall. Acute dissection of aorta complicating a coronary intervention is a rare occurrence, with incidence reported as 0.02% of coronary angioplasties.2 It is associated mostly with interventions of the right coronary artery (RCA)3–7 and occurs very rarely with interventions of the left coronary circulation.5 8 9 The appropriate management and outcome of these cases is not well established. Treatment options depend on patient stability, nature and extent of dissection, and ability to restore the coronary circulation by further interventions.5 7
Here we report a case of 55-year-old woman who developed dissection of the ascending aorta during angioplasty of the right coronary artery, and who was treated with drug eluting stents and surgery.
Case presentation
A 55-year-old Caucasian woman with a medical history of hypertension and hyperlipidaemia presented to us with recurrent episodes of substernal chest pain. The pain lasted about 5–10 min, worsened with exertional activities, radiated to the arms and was relieved with rest as well as by nitroglycerine. There was no history of palpitations, orthopnoea, fever, cough or shortness of breath. The patient was a former smoker and quit 6 years earlier.
On examination, the patient was alert, oriented and responsive. She had a regular heart rate of 64/min and a blood pressure of 118/78 mm Hg. The rest of the physical examination revealed no significant findings.
Investigations
ECG revealed inferolateral ischaemic changes. The patient was scheduled for a coronary angiography, which showed an acutely occluded RCA (figure 1). During angiography, the RCA was wired across the area of total occlusion without difficulty, after engaging the artery with a 6-French guide. Angioplasty was performed in the proximal segment with a 2.0×12 mm balloon. While performing left ventriculography, aortic insufficiency was seen. Hence, a decision was made to perform aortography, which showed an echo-dense filling on the ascending aorta (figure 2). During this time, the patient denied any chest pain, shortness of breath or dizziness. However, she did have elevated blood pressure up to 192/105 mm Hg. The rest of the vital signs were as follows: afebrile, pulse rate of 75/min, respiratory rate of 21/min and oxygen saturation of 99% on room air. CT of the chest confirmed a proximal dissection of the ascending aorta (figure 3).
Figure 1.
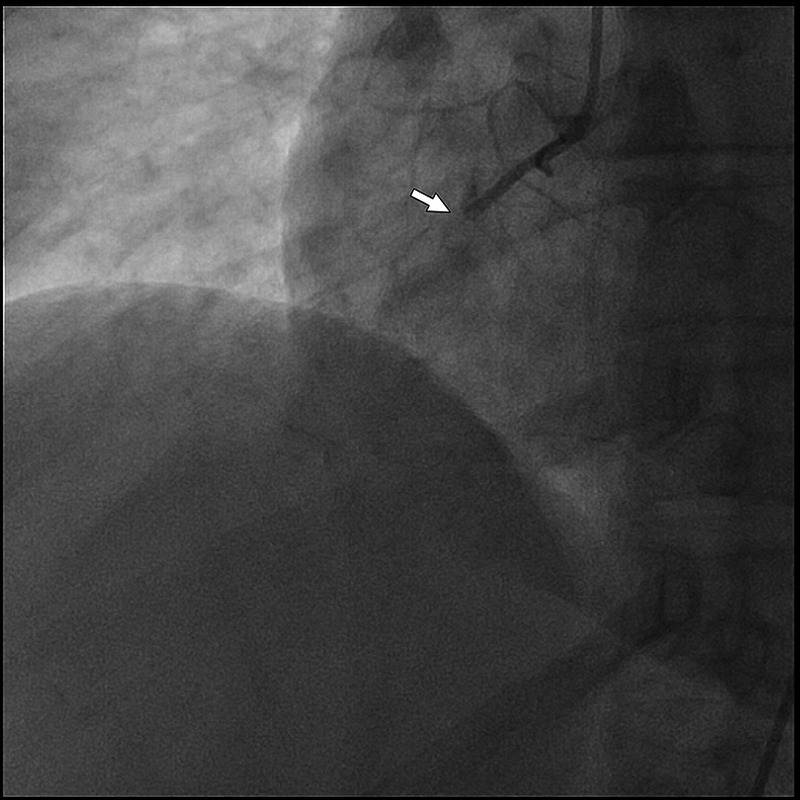
Coronary angiogram showing totally occluded proximal segment of the right coronary artery.
Figure 2.
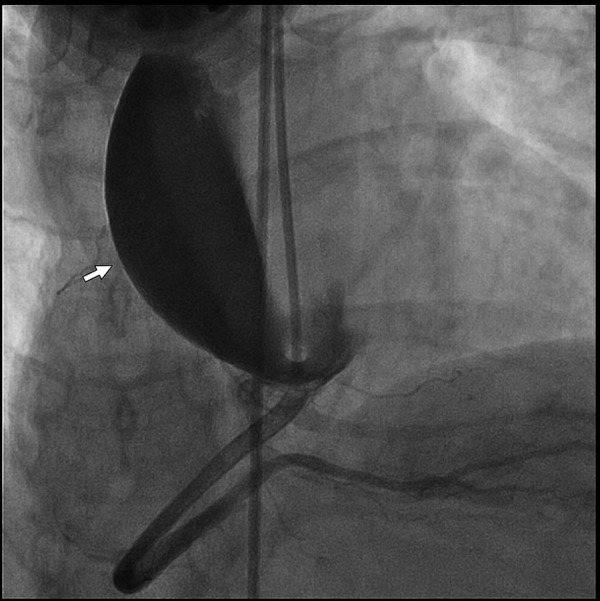
Post-stenting right coronary angiogram showing large iatrogenic aortic dissection that spans from the right coronary sinus to the aortic arch.
Figure 3.
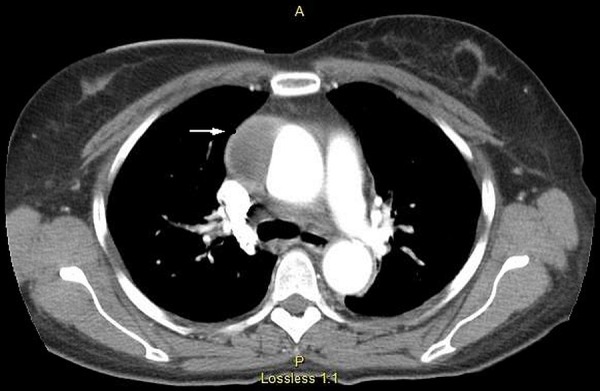
CT of the chest showing aortic dissection of the ascending aorta with false lumen (as shown by the arrow).
Treatment
Three drug-eluting stents were placed immediately in the RCA and urgent proximal aortic root repair was undertaken.
Outcome and follow-up
The postoperative course was uneventful. The patient was transferred out of the intensive care unit on the third postoperative day. The rest of the hospitalisation was also uneventful and she was sent home on the seventh postoperative day in stable clinical condition. Although a follow-up was recommended in 2 weeks following discharge at the outpatient clinic, the patient did not show up and has been lost to follow-up since then.
Discussion
Aortic dissection is an extremely rare complication of coronary intervention. The origin of this dissection may be in the aortic root or coronary ostium.10 The precise mechanism remains unknown and it is suspected to occur due to forceful use of a catheter or guide wire, vigorous injection of dye or underlying degeneration of the aortic wall.8 11 12 Aortic dissection is more common during interventions of the RCA than left coronary artery and may be due to its comparatively thin wall, tortuous anatomy and small size.13 14
Propagation of the aortic dissection may occur in an anterograde or a retrograde fashion leading to complications such as myocardial infarction, aortic valve insufficiency, haemopericardium or cardiac tamponade.15 Continuous monitoring for early recognition and prompt management of these complications is crucial.
Treatment should be tailored depending on clinical and haemodynamic stability of the patient. Conservative treatment is sufficient in cases limited to aortic sinus of valsalva.16 Localised dissections can be managed with implantation of stents distal to the dissection and near the ostium, thus sealing the entry port.7 8 They can be followed up with ECG and CT scan after restoration of coronary blood flow by stenting.5 7 Surgery is the option if stenting fails, or if the patient is haemodynamically unstable or there is extensive dissection.2 4 7 In a review of nine cases by Dunning et al,2 limited aortic involvements were successfully managed with stenting while dissections larger than 4 cm required surgical intervention. Emergency surgeries are associated with high risk because the patients are unstable. Moreover, aortic root replacement or replacement of the ascending aorta with coronary artery bypass grafting may have to be performed in an emergent situation, which increases the risk further.7
In our case, aortic root dissection was noted during coronary angioplasty and it propagated to involve the ascending aorta. Consequently, three drug-eluting stents were placed and the aortic dissection was corrected by surgery.
Learning points.
Aortic dissection, although rare compared to coronary artery dissection, can occur as a complication of coronary intervention.
It may occur due to forceful use of a catheter or guide wire, vigorous injection of dye or underlying degeneration of the aortic wall. The right coronary artery is more commonly affected than left coronary artery due to its comparatively thin wall, tortuous anatomy and small size.
Treatment depends on clinical and haemodynamic stability of the patient. Localised dissections may be managed conservatively. Other options are stenting and surgery, employed mainly in extensive dissection or unstable patients.
Footnotes
Contributors: SG and PD wrote the first draft. IH gathered clinical information and imaging. SA supervised the project and critically reviewed the final draft.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Hermans WRM, Foley DP, Rensing BJ et al. Usefulness of quantitative and qualitative angiographic lesion morphology, and clinical characteristics in predicting major adverse cardiac events during and after native coronary balloon angioplasty. Am J Cardiol 1993;72:14–20. [DOI] [PubMed] [Google Scholar]
- 2.Dunning DW, Kahn JK, Hawkins ET et al. Iatrogenic coronary artery dissections extending into and involving the aortic root. Catheter Cardiovasc Interv 2000;51:387–93. [DOI] [PubMed] [Google Scholar]
- 3.Moles VP, Chappuis F, Simonet F et al. Aortic dissection as complication of percutaneous transluminal coronary angioplasty. Cathet Cardiovasc Diagn 1992;26:8–11. [DOI] [PubMed] [Google Scholar]
- 4.Ochi M, Yamauchi S, Yajima T et al. Aortic dissection extending from the left coronary artery during percutaneous coronary angioplasty. Ann Thorac Surg 1996;62:1180–2. [DOI] [PubMed] [Google Scholar]
- 5.Perez-Castellano N, Garcia-Fernandez MA, Garcia EJ et al. Dissection of the aortic sinus of Valsalva complicating coronary catheterization: cause, mechanism, evolution, and management. Cathet Cardiovasc Diagn 1998;43:273–9. [DOI] [PubMed] [Google Scholar]
- 6.Varma V, Nanda NC, Soto B et al. Transesophageal echocardiographic demonstration of proximal right coronary artery dissection extending into the aortic root. Am Heart J 1992;123(4 Pt 1):1055–7. [DOI] [PubMed] [Google Scholar]
- 7.Yip HK, Wu CJ, Yeh KH et al. Unusual complication of retrograde dissection to the coronary sinus of Valsalva during percutaneous revascularization: a single-center experience and literature review. Chest 2001;119:493–501. [DOI] [PubMed] [Google Scholar]
- 8.Seifein HB, Missri JC, Warner MF. Coronary stenting for aortocoronary dissection following balloon angioplasty. Cathet Cardiovasc Diagn 1996;38:222–5. [DOI] [PubMed] [Google Scholar]
- 9.Wyman RM, Safian RD, Portway V et al. Current complications of diagnostic and therapeutic cardiac catheterization. J Am Coll Cardiol 1988;12:1400–6. [DOI] [PubMed] [Google Scholar]
- 10.Bae JH, Kim KB, Kim KS et al. A case of aortocoronary dissection as a complication during a percutaneous transluminal coronary angioplasty (PTCA). Int J Cardiol 1998;66:237–40. [DOI] [PubMed] [Google Scholar]
- 11.Kwan T, Elsakr A, Feit A et al. Combined dissection of the right coronary artery and right coronary cusp during coronary angiography. Cathet Cardiovasc Diagn 1995;35:328–30. [DOI] [PubMed] [Google Scholar]
- 12.Hung MY, Hung MJ, Degertekin M et al. How should I treat a retrograde dissection of the aortic sinus of Valsalva during a percutaneous coronary intervention? Euro Intervention 2012;8:520–7. [DOI] [PubMed] [Google Scholar]
- 13.Abdou SM, Wu CJ. Treatment of aortocoronary dissection complicating anomalous origin right coronary artery and chronic total intervention with intravascular ultrasound guided stenting. Catheter Cardiovasc Interv 2011;78:914–19. [DOI] [PubMed] [Google Scholar]
- 14.Doyle B, Juergens CP. Conservative management of ascending aortic dissection caused by percutaneous coronary intervention. J Invasive Cardiol 2004;16:92–4. [PubMed] [Google Scholar]
- 15.Uyan C, Arinc H, Gunduz H et al. Dissection of the ascending thoracic aorta as a complication of percutaneous coronary intervention. Vasc Health Risk Manag 2008;4:253–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Park IW, Min PK, Cho DK et al. Successful endovascular treatment of iatrogenic coronary artery dissection extending into the entire ascending aorta. Can J Cardiol 2008;24:857–9. [DOI] [PMC free article] [PubMed] [Google Scholar]