

Abstract
Objective
Facial-type-associated variations in diagnostic features have several implications in orthodontics. For example, in hyperdivergent craniofacial types, growth imbalances are compensated by displacement of the condyle. When diagnosis and treatment planning involves centric relation (CR), detailed knowledge of the condylar position is desirable. The present study aimed to measure condylar displacement (CD) between CR and maximum intercuspation in three facial types of an asymptomatic orthodontic population.
Methods
The study was conducted in 108 patients classified into three groups of 36 individuals each (27 women and 9 men; mean age, 20.5 years), based on the following facial patterns: hyperdivergent, hypodivergent, and intermediate. To quantify CD along the horizontal and vertical axes, the condylar position was analyzed using mounted casts on a semi-adjustable articulator and a mandibular position indicator. The Student t-test was used to compare CD between the groups.
Results
Vertical displacement was found to be significantly different between the hyperdivergent and hypodivergent groups (p < 0.0002) and between the hyperdivergent and intermediate groups (p < 0.0006). The differences in horizontal displacement were not significant between the groups. In each group, vertical CD was more evident than horizontal displacement was.
Conclusions
All facial types, especially the hyperdivergent type, carried a significantly high risk of CD. Therefore, the possibility of CD should be carefully evaluated and considered in the assessment of all orthodontic cases in order to accurately assess jaw relationships and avoid possible misdiagnosis.
Keywords: Cephalometrics, Centric relation, Condylar displacement, Growth evaluation, Maximum intercuspation
INTRODUCTION
Adaptive condylar displacement (CD) refers to the shift from a seated condylar position or centric relation (CR) to a condylar position corresponding to maximum intercuspation (MI). Consequently, CD may have diagnostic and clinical implications.1,2,3,4 Orthodontists who follow the functional occlusion principles published by Roth1 accept that when the normal proportional relation of 0.75 between the posterior cranial base (sella-articulare) and ramus height (articulare-gonion) increases to a value of 1.0, the risk of an adapted intra-articular condyle shift increases, making the assessment of the mandibular position clinically pertinent.
This is, however, a controversial subject.5 Despite the consensus regarding dual bites as an alternative to surgical treatment in adults, for diagnostic and treatment purposes, evaluation of the orthopedic position of CR is the most physiologically appropriate6; in fact, it is recommended as the morphofunctional aim of any orthodontic occlusal treatment.1,7 Since CR is the most consistent and reproducible positional reference,8 accurate studies of dental and maxillomandibular relationships are dependent on CR assessment. Splint therapy allows stabilization of the condyle in CR for therapeutic or diagnostic purposes, prior to orthodontic treatment.9
In patients with a hyperdivergent facial type, CD represents a mechanism of compensation to posterior-anterior facial imbalance. Since the mandible articulates with the cranial base, vertical growth of the anterior face should ideally match posterior facial growth.10 However, if this does not occur, the condyle can rotate in the temporomandibular joint or slide vertically or antero-posteriorly in order to adjust to the imbalance.1,2,3,8,11,12 An increased joint space could lead to articular instability since the articular disc can lose its tight apposition between the condyle and cranial base and easily dysfunction.1 Previous studies have shown that posterior mandibular displacement leads to temporomandibular disorders (TMD)6 and morphological changes.13 Additionally, studies focusing on the relation between facial configuration and TMD indicate an association of hyperdivergency with TMD.14,15
The assessment of the normal condyle-fossa relationship is also debatable. In normal samples, tomographic imaging reveals a wide variability in condylar position,16,17 and intra-articular joint damage has been detected in asymptomatic patients.18 More recently, a study analyzing clinical data from magnetic resonance imaging and limited cone-beam computed tomography reported that the variability in CD is limited in normal individuals, and quantitative standards for the clinical evaluation of the condylar position were suggested.19
Since the condylar axis can be widely influenced by occlusion,2,4 it is of paramount importance to determine its displacement in three-dimensional space.20 Conventional radiological examinations do not provide accurate and valuable information in this regard;16,17 consequently, a mandibular position indicator (MPI) and other similar tools have been introduced to allow quantification of the three-dimensional displacement of the condylar axis.3,21,22
The significance and clinical relevance of identifying and integrating CD in orthodontic diagnosis and treatment planning, when it surpasses a threshold of 2 mm in the horizontal or vertical axis has been established.2,4,7 In addition, CD of significant magnitude occurs frequently in the asymptomatic population4,23 and represents an attempt to compensate for disproportions. Accurate diagnosis requires the assessment of occlusal interferences and skeletal relationships, without the influence of the neuromuscular system. Despite reasonable evidence of facial configurations being more prone to articular instability, data related to the subject is scarce and conflicting. Girardot12 reported a more significant CD in hyperdivergent facial morphologies, whereas Burke et al.24 found diminished upper articular joint spaces in the same facial type. In contrast, Hidaka et al.11 found no relationship between facial type and condylar position.
Therefore, the aim of this observational study was to clarify the above-mentioned conflicting findings and throw more light on the relationship between facial type and condylar position. Therefore, CD was measured in the hyperdivergent facial type and compared with those of the hypodivergent and intermediate types. The hypothesis of this study was that CD was greater and more frequent in the hyperdivergent facial type.
MATERIALS AND METHODS
The research protocol was reviewed and approved by the Ethical Committee of the Faculty of Dental Medicine of University of Porto (#20071210). The study sample comprised 108 Caucasian asymptomatic individuals, 81 women and 27 men, aged between 12 and 46.2 years, with a mean age of 20.5 years. Data used for the study included information from anamnesis and clinical examinations, lateral cephalograms in MI, study casts and clinical records for CR mounting on a SAM® 2P semi-adjustable articulator (Figure 1), and complete MPI registrations (SAM®; Präzisionstechnik GmbH, München, Germany) (Figures 2 and 3).
Figure 1.
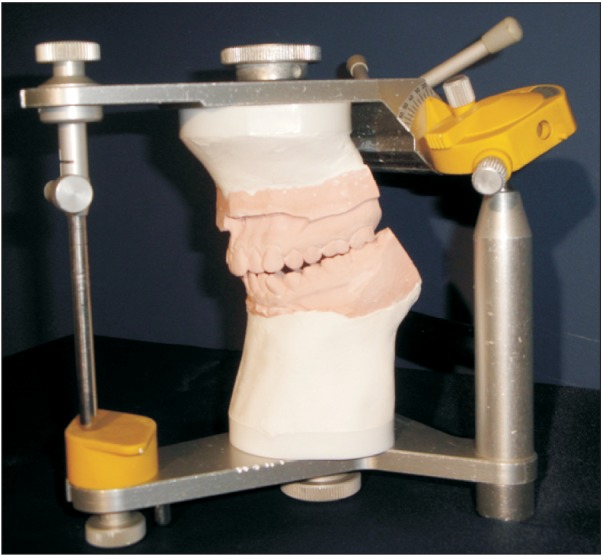
Study casts mounted in centric relation on an SAM® 2P semi-adjustable articulator.
Figure 2.
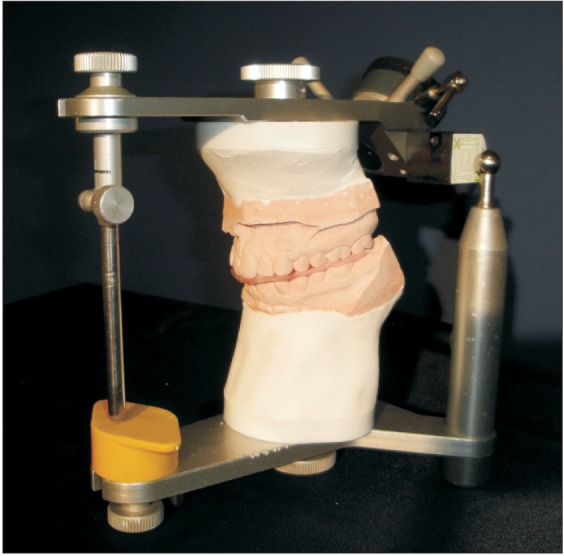
A mandibular position indicator attached to a cast of the upper arch, and maximum intercuspation wax registration interposed between the two casts in order to register the corresponding condylar position.
Figure 3.
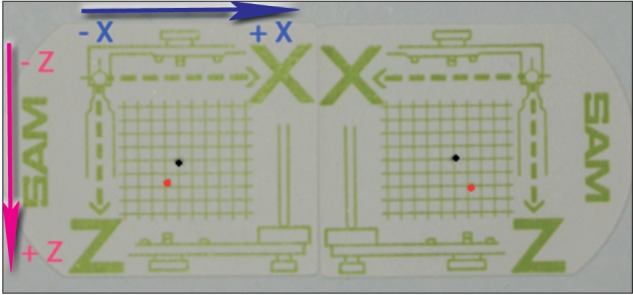
A mandibular position indicator registration: black and red dots represent right and left condylar positions corresponding to centric relation and maximum intercuspation, respectively. Axial displacements are as follows: for the right condyle, -0.9 mm in XX' and +1.8 mm in ZZ'; and for the left condyle, -1.3 mm in XX' and +2.2 mm in ZZ'.
The subjects were selected based on the clinical records of 742 consecutive first presentations at an orthodontic private practice. Based on the study criteria, we included individuals, who, during the preceding 5 years, had neither suffered facial trauma nor been subjected to orthodontic treatment. For the selection of asymptomatic individuals, the Helkimo Index25 was used, and only patients with codes Di0 or Di1 were chosen. To avoid the effect of distortions related to growth on condylar position registration,26 patients in stages 4, 5, or 6 of skeletal maturation according to the cervical vertebral maturation method27 were considered for this study. Subjects with a negative vertical CD (ΔZ < 0) on the MPI reading were excluded.8 To classify the subjects into groups based on distinct facial patterns, two matched factors of Jarabak's cephalometric analysis were used.28 Subjects with the posterior facial height (PFH; sella-gonion)/anterior facial height (AFH; nasion-menton) ratio ≤ 59% and the lower gonial angle (LGA; nasion-gonion-menton) ≥ 76° were grouped into the hyperdivergent group. The hypodivergent group comprised subjects with the PFH/AFH ≥ 65% and LGA ≤ 69°. In the third intermediate group, the PFH/AFH was 59-65% and LGA was 69°-76°. Thus, based on the skeletal facial features, 3 matched groups containing 36 individuals each, 27 women and 9 men, were generated.
A single operator with 5 years' experience was involved in all the clinical and laboratory experiments. A single arbitrary face bow and SAM® 2P articulator were used for mounting the stone casts (Velmix; Kerr® Manufacturing Co., Romulus, MI, USA) with the CR wax records (DeLar Bite Registration Wax; DeLar® Corporation, Lake Oswego, OR, USA). Horizontal and vertical CD were evaluated using a single MPI and MI wax records (Moyco® Industries Inc., Philadelphia, PA, USA).
The MI records were obtained before CR registration, by asking the patient to bite firmly with the teeth in MI. After being chilled in ice water, record accuracy was checked in the mouth. For CR registration, Roth's power centric technique8 was performed immediately after neuromuscular deprogramming with the patient relaxed and reclined at 45°. Two cotton rolls were interposed between the dental arches for a minimum of 10 minutes. CR bite registration was performed in two stages. With the softened wax, the anterior section was obtained by guiding the mandible during closure in order to avoid protrusion. The cusps responsible for premature inter-arch contact were maintained 2-mm apart. Next, the anterior wax was hardened in ice water and then interposed between the arches simultaneously with the posterior softened wax section in order to accomplish the registration. The mandible was guided during closure, and when the anterior teeth fit into the corresponding anterior wax indentations, the patient was asked to bite firmly. With this technique, as the posterior wax section was softened, muscular strength helped to adjust the vertical intra-articular condylar position.29
For wax registration of MI, the corresponding position of the condyle was registered with the MPI, and its accuracy was checked after every 5 registrations. A micrometre (Nr.H 114834; Carl Zeiss® AG, Oberkochen, Germany) was used to measure the horizontal (XX') and vertical (ZZ') CD components, and each measurement was repeated three times. The average of two close values was considered the final value.
The methodology applied in this study had been checked at the beginning of data collection, and the Lauritzen technique was used to assess the accuracy of CR records and laboratory procedures.28
To evaluate intra-operator error, the reproducibility of CR records, mounting procedures, accomplishment and measurement of MPI registrations, and cephalometric measurements were performed by the same operator during two different sessions that were one-week apart. For these procedures, 5 patients were randomly selected, and the clinical measurements were obtained twice during each session, resulting in the need for two articulator-mounting sets for each subject. During the second session, two new CR records were used to remount the mandibular cast to each previously articulator mounting. The procedure was repeated twice for each mounting set. The new MI records allowed comparisons of the MPI registrations. The results were systematized into tables for analysis.
Statistical analysis
For direct measurements, errors were analyzed using the analysis of variance test. According to the following equation, the standard error (SE) was obtained depending on the sample variance (SV):
where N refers to the sample size; Xi, dimension observed for measurement I; and x, mean value of observations.
For indirect measurements, the following equation of error propagation was applied:
where Xj refers to the dimension measured (j = 1,…, M); SEj, standard error associated with Xj; and X = F(X1, X2, … XM), dimension based on dimensions of Xj.
To determine the direction and magnitude of any condylar shift, an initial descriptive study of data was performed, which was followed by a comparative study. A Student t-test, with 0.05 level of confidence, was used to analyze the differences in CD along the vertical and horizontal planes among the three groups.
RESULTS
Analysis of the measurement errors of the different assessments showed an error margin < 4.5%, which is considered acceptable.28
No negative vertical CD (ΔZ < 0) on the MPI readings was registered. In the total sample (n = 216 condyles, Table 1), horizontal displacement CD-XX' ≥ 2 mm and CD-XX' ≤ -2 mm occurred in 14/216 condyles (6.49%), whereas vertical displacement CD-ZZ' ≥ 2 mm occurred in 60/216 condyles (27.77%). Therefore, CD-XX' ≤ -2 mm occurred in hyperdivergent and intermediate groups in 2.78% and 4.17% of cases, respectively, whereas CD-XX' ≥ 2 mm was more frequent in the hypodivergent group (8.33%). The most frequent displacements were observed in a posterior direction in the hyperdivergent and intermediate groups. Along the ZZ' axis, the frequency of CD-ZZ' ≥ 2 mm was high in all the groups, with registered values of 34.72%, 23.61%, and 25.0%, respectively, in the hyperdivergent, hypodivergent, and intermediate groups.
Table 1.
Number and percentage of condyles (72 condyles per group) displaced along the horizontal (XX') and vertical (ZZ') axes
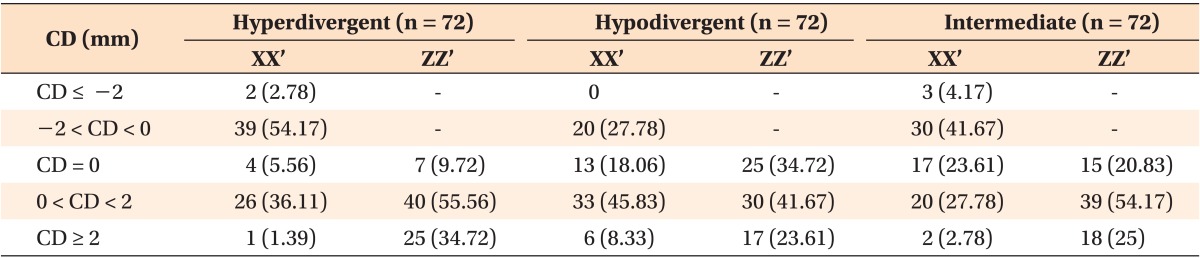
Values are presented as number (%).
CD, Condylar displacement.
The values of horizontal displacement ranged from -3.5 mm to 4 mm, whereas vertical displacement ranged from 0 to 4.1 mm (Table 2).
Table 2.
Mean values (SD) and minimum and maximum (mm) horizontal (XX') and vertical (ZZ') displacements in the three groups

SD, Standard deviation.
*lXX'l (SD) means considering absolute values.
To assess the effective magnitude of CD, the displacements along the XX' axis were summed, and the absolute values were considered (Table 3). A comparison of the magnitude of CD among the three groups showed more extensive CD in the hyperdivergent group (118.7 mm) along the ZZ' axis and in the hypodivergent group (67.53 mm) along the XX' axis. The magnitude of horizontal displacement was approximately similar in all the groups, varying from 53.5 mm in the intermediate to 67.53 mm in the hypodivergent group. Results of the t-test showed that vertical displacement was statistically different between hyperdivergent and hypodivergent groups (p < 0.0002) and hyperdivergent and intermediate groups (p < 0.0005). No significant difference in horizontal displacement was noted between the groups (p < 0.071).
Table 3.
Summation of displacements along the horizontal (XX') and vertical (ZZ') axes (mm), and the corresponding mean values in the three groups
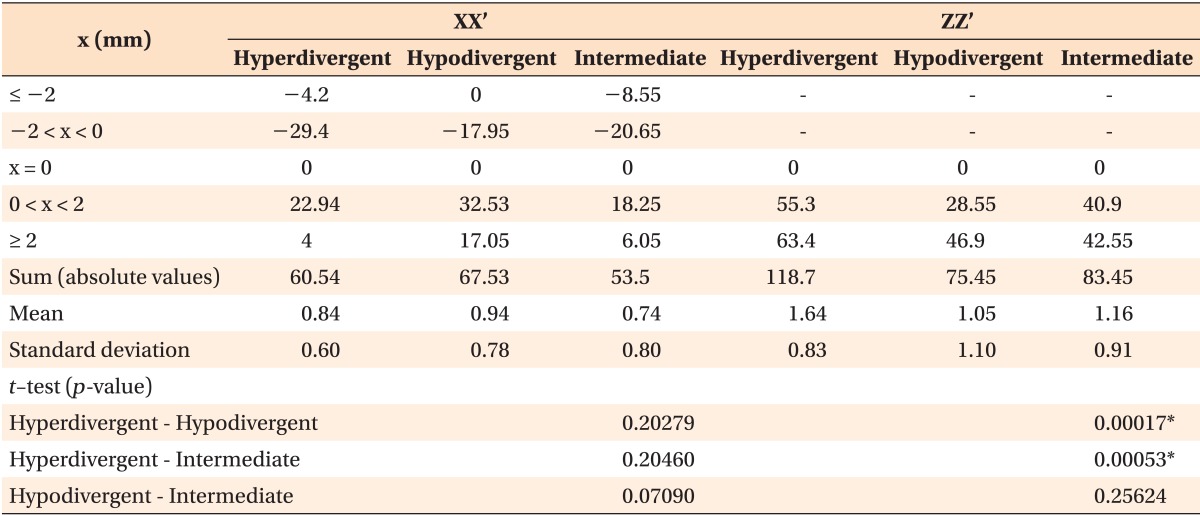
x, Horizontal condyle displacement.
*p ≤ 0.05.
DISCUSSION
Taking into account the obvious differences between the facial groups, the anatomo-physiological features of hyperdivergent facial types may be the reason that condyle function is prone to articular instability. This study aimed to test the hypothesis that CD was greater and more frequent in the hyperdivergent facial type. The three groups examined in this study represented individuals with clear hyperdivergent (dolicofacial) features, hypodivergent (brachifacial) features, and with intermediate qualities. The intermediate group included mesofacial subjects and individuals with dolicofacial or brachifacial tendencies.
The clinically significant CD threshold of 2 mm has diagnostic importance,2,4,7 leading to clinical implications.3 In fact, it is recommended to use this information to convert cephalometric tracings when displacements of ≥ 2 mm are found along at least one of the axes. A smaller magnitude of CD yields none or no significant changes in traditional cephalometric measurements.2 In the 216 condyles analyzed in this study, CD ≥ 2 mm was found in approximately 30% of the cases (CD-ZZ' ≥ 2 mm in 27.77, CD-XX' ≥ 2 mm, and CD-XX' ≤ -2 in 6.49; Table 1). In general, these results are in agreement with those of previous studies, although some discrepancies in frequencies were found.2,4,11,12,23,26 These differences may be related to the criteria used for sample selection, neuromuscular deprogramming methodology, or CR recording techniques. The use of hard anterior stops for CR bite registration can duplicate the frequency of CD ≥ 2 mm.4,23
It was suggested that a more efficient deprogramming technique could result in a higher frequency of CD in the three groups. Ideally, complete deprogramming should be performed before CR registration; however, it is not practical in daily orthodontic practice, and the method of interposition of cotton rolls for 10 minutes was used in this study. Therefore, the registrations obtained represent the most superior and anterior positions of the condyles in the joint the clinician was able to take during the moment of clinical procedure in the asymptomatic patients. However, differences in the effective CR position can be noted in some cases.
Posterior displacement was slightly more frequent (43.52%) than anterior displacement (40.74%). The higher frequency of posterior condylar shift is consistent with previous studies and is related to posterior occlusal prematurity guiding the mandible in this direction.2,3,11,12,23
The analysis of CD and its comparison between the three groups showed that CD was more frequent in the hyperdivergent group, corroborating the initial hypothesis. This group, considering the number of condyles with CD ≥ 2 mm, presented a frequency of vertical displacement of 34.72%, which is higher than the 28.8% reported by Girardot.12 With respect to the absolute values of horizontal displacement, the hyperdivergent group registered 4.17% in contrast to 24.2% reported by Girardot. The great majority of XX' displacements were between -2 and 2 mm. Therefore, in the hyperdivergent group, 54.17% of displacements occurred in the posterior direction with magnitudes between -2 and 0 mm. In contrast, Hidaka et al.11 found vertical and horizontal CD ≥ 2 mm of 14% and 2%, respectively. However, their study sample was inherently different from that of our study.
In the hyperdivergent and intermediate groups, high frequencies were recorded in the posterior direction (56.95 and 45.84%, respectively); in contrast, in the hypodivergent group, the higher frequency was in anterior direction (54.16%). The frequencies of posterior, anterior, and vertical displacements in the intermediate group were midway between the other two groups. These findings may be related to the differences in facial configurations, i.e., the distinct patterns of muscle activity and behavior facing fulcrums. In fact, in the hypodivergent biotype, the elevator muscles are stronger and aligned vertically across the first molars, being positioned more anteriorly than those in the hyperdivergent group. This leads to the exertion of more force in the anterior direction.
The magnitude of means (absolute values) along XX' was 0.84 mm, 0.94 mm, and 0.74 mm; along ZZ', it was 1.65 mm, 1.05 mm, and 1.61 mm, respectively, in the hyperdivergent, hypodivergent, and intermediate groups (Table 2). Girardot12 found mean values of 1.21 mm for hyperdivergent and 0.66 mm for hypodivergent along XX' and 1.7 mm for hyperdivergent and 1.2 mm for hypodivergent along ZZ'. The mean values that closely matched those of our study were those related to the vertical plane and may be related to the method used to record CR. The hard anterior stop used in Roth's power centric technique supports the generation of a more seated condylar position, as it is the internal strength of the masticatory muscles that positions and vertically seats the condyles in the fossae.3,8,29 Therefore, the registration of the vertical axis shift is less dependent on individual operator technique. Previous studies,4,23 with deprogrammed subjects, found greater vertical displacements and established that more efficient deprogramming procedures can allow assessment of greater CD mean values, particularly along the vertical axis.26 However, other studies contradicted these results. Burke et al.24 studied the association of condyle features of Class II preadolescent patients with facial configurations and found correlations between diminished superior joint spaces and vertical patterns. These differences may be related to intrinsic variations in the samples and to a lack of functional examination of the subjects. In fact, the neuromuscular system can display two kinds of responses to occlusal fulcrums. One displaces the condyle in the joint to achieve maximal occlusal contact, whereas the other is the appearance of an anterior open bite, characterized by only posterior teeth contacts, with the CD being reduced in this situation. Moreover, Hidaka et al.11 did not find any relation between facial patterns and CD. Their evaluation was performed using the mandibular plane angle and disregarded the individual's skeletal maturity and functional examination, which are factors that can strongly compromise condylar shifts.
In this study, greater vertical displacement was observed in the hyperdivergent group: CD was found to be 1.57 and 1.42 times greater than that in the hypodivergent and intermediate groups (Table 3). Horizontal displacements were closer and varied from 53.5 mm to 75.45 mm. In all the groups, the magnitude of vertical shifts was always higher than that of the horizontal shifts, which is in agreement with the findings of previous studies.2,4,11,12,23,26 This finding shows that, although CD is frequent in all three facial groups, a higher risk of shift is observed in the hyperdivergent group, which is in agreement with Girardot's results.12 It is important to note that both studies reported significant differences in CD along the ZZ' axis (present study: hyperdivergent-hypodivergent groups, p < 0.0002 and hyperdivergent-intermediate groups, p < 0.0005; Girardot study: hyperdivergent-hypodivergent groups, p < 0.008), but for horizontal displacements only Girardot, reported this finding (hyperdivergent-hypodivergent groups, p < 0.0001). In the present study, for XX' axis displacements, no significant differences were observed, but a trend could be suggested between the hyperdivergent and intermediate groups (p < 0.071).
Although referring to asymptomatic samples, both studies indicate that the physical features of the hyperdivergent group predispose it to a higher risk of developing TMD.14,15 However, it is important to note that the transverse shift was not considered, despite being recognized as an etiologic factor of TMD.30 Therefore, this potential relationship needs to be investigated further.
The results of this study suggest that orthodontic treatment planning related to the CR must involve assessment of the condyle shift. However, it is not possible to quantify displacement clinically, directly in the mouth4,8,23 or by using MI hand-assembled casts. When detected, occlusal discrepancy provides no information regarding the nature of CD.4,17 This study especially emphasizes on the vertical component of CD, which is even more difficult to detect. The MPI instrumentation procedure permits easy and accurate3,8,21,22 quantification of CD and allows taking this data into account when planning treatment, introducing diagnostic clinical implications, and reducing misdiagnosis.2,4
In contrast with MI hand-assembled casts, articulator-mounted cast analysis can display cases with different features and with a distinctly difficult level of treatment. The discrepancy can be altered not only in the sagittal plane, with differences in overjet and molar relationship, but also in the transverse and vertical planes.2,4 The analysis of the initial occlusal contacts can support differential diagnosis of skeletal and dentoalveolar openbite or crossbite. When approaching transversal problem the consideration of interocclusal type of contacts, the cuspid to cuspid or cuspid to inclined slope contact, can help to discard the skeletal nature of malocclusion. Additionally, simulation of a true hinge axis (vertical mandibular autorotation) can provide information regarding features of the Class II malocclusion. In case of a vertical Class II malocclusion, overjet can be corrected when posterior occlusal interferences are eliminated; however, in case of a sagittal Class II malocclusion, overjet remains, and a different treatment plan is required. The method described in this study can reveal important information with regard to vertical malocclusion, which is not provided by other diagnostic techniques, causing frequent failure in occluso-functional orthodontic treatment.
Overall, since a significant magnitude of CD occurs in all the three asymptomatic groups and since it is not possible to predict the condylar position, it is crucial to mount models in CR as a routine diagnostic procedure.2,4 Our study clearly shows that in patients with a hyperdivergent facial pattern, the risk of misdiagnosing an orthodontic case is approximately 30%, when condylar position in not assessed.
CONCLUSION
The findings of this study show that the hyperdivergent group has a significantly greater CD along the vertical axis than do the two other groups. No differences were found in horizontal displacement between the groups. Therefore, if CD is not considered during the assessment of orthodontic cases, the risk of misdiagnosis is high for all facial types, being significantly higher in patients with the hyperdivergent facial type.
Footnotes
The authors report no commercial, proprietary, or financial interest in the products or companies described in this article.
References
- 1.Roth RH. Functional occlusion for the orthodontist. J Clin Orthod. 1981;15:32–40. 44-51 contd. [PubMed] [Google Scholar]
- 2.Shildkraut M, Wood DP, Hunter WS. The CR-CO discrepancy and its effect on cephalometric measurements. Angle Orthod. 1994;64:333–342. doi: 10.1043/0003-3219(1994)064<0333:TCDAIE>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Crawford SD. Condylar axis position, as determined by the occlusion and measured by the CPI instrument, and signs and symptoms of temporomandibular dysfunction. Angle Orthod. 1999;69:103–115. doi: 10.1043/0003-3219(1999)069<0103:CAPADB>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 4.Cordray FE. Three-dimensional analysis of models articulated in the seated condylar position from a deprogrammed asymptomatic population: a prospective study. Part 1. Am J Orthod Dentofacial Orthop. 2006;129:619–630. doi: 10.1016/j.ajodo.2004.10.015. [DOI] [PubMed] [Google Scholar]
- 5.Rinchuse DJ, Kandasamy S. Myths of orthodontic gnathology. Am J Orthod Dentofacial Orthop. 2009;136:322–330. doi: 10.1016/j.ajodo.2008.04.021. [DOI] [PubMed] [Google Scholar]
- 6.Isberg AM, Isacsson G. Tissue reactions of the temporomandibular joint following retrusive guidance of the mandible. Cranio. 1986;4:143–148. doi: 10.1080/08869634.1986.11678139. [DOI] [PubMed] [Google Scholar]
- 7.Slavicek R. Clinical and instrumental functional analysis and treatment planning. Part 4. Instrumental analysis of mandibular casts using the mandibular position indicator. J Clin Orthod. 1988;22:566–575. [PubMed] [Google Scholar]
- 8.Wood DP, Elliott RW. Reproducibility of the centric relation bite registration technique. Angle Orthod. 1994;64:211–220. doi: 10.1043/0003-3219(1994)064<0211:ROTCRB>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Beard CC, Clayton JA. Effects of occlusal splint therapy on TMJ dysfunction. J Prosthet Dent. 1980;44:324–335. doi: 10.1016/0022-3913(80)90021-9. [DOI] [PubMed] [Google Scholar]
- 10.Isaacson JR, Isaacson RJ, Speidel TM, Worms FW. Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod. 1971;41:219–229. doi: 10.1043/0003-3219(1971)041<0219:EVIVFG>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Hidaka O, Adachi S, Takada K. The difference in condylar position between centric relation and centric occlusion in pretreatment Japanese orthodontic patients. Angle Orthod. 2002;72:295–301. doi: 10.1043/0003-3219(2002)072<0295:TDICPB>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Girardot RA., Jr Comparison of condylar position in hyperdivergent and hypodivergent facial skeletal types. Angle Orthod. 2001;71:240–246. doi: 10.1043/0003-3219(2001)071<0240:COCPIH>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Desai S, Johnson DL, Howes RI, Rohrer MD. Changes in the rabbit temporomandibular joint associated with posterior displacement of the mandible. Int J Prosthodont. 1996;9:46–57. [PubMed] [Google Scholar]
- 14.Ahn SJ, Baek SH, Kim TW, Nahm DS. Discrimination of internal derangement of temporomandibular joint by lateral cephalometric analysis. Am J Orthod Dentofacial Orthop. 2006;130:331–339. doi: 10.1016/j.ajodo.2005.02.019. [DOI] [PubMed] [Google Scholar]
- 15.Hwang CJ, Sung SJ, Kim SJ. Lateral cephalometric characteristics of malocclusion patients with temporomandibular joint disorder symptoms. Am J Orthod Dentofacial Orthop. 2006;129:497–503. doi: 10.1016/j.ajodo.2004.12.019. [DOI] [PubMed] [Google Scholar]
- 16.Pullinger AG, Hollender L, Solberg WK, Petersson A. A tomographic study of mandibular condyle position in an asymptomatic population. J Prosthet Dent. 1985;53:706–713. doi: 10.1016/0022-3913(85)90029-0. [DOI] [PubMed] [Google Scholar]
- 17.Hatcher DC, Blom RJ, Baker CG. Temporomandibular joint spatial relationships: osseous and soft tissues. J Prosthet Dent. 1986;56:344–353. doi: 10.1016/0022-3913(86)90018-1. [DOI] [PubMed] [Google Scholar]
- 18.Ribeiro RF, Tallents RH, Katzberg RW, Murphy WC, Moss ME, Magalhaes AC, et al. The prevalence of disc displacement in symptomatic and asymptomatic volunteers aged 6 to 25 years. J Orofac Pain. 1997;11:37–47. [PubMed] [Google Scholar]
- 19.Ikeda K, Kawamura A. Assessment of optimal condylar position with limited cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2009;135:495–501. doi: 10.1016/j.ajodo.2007.05.021. [DOI] [PubMed] [Google Scholar]
- 20.Cordray FE. The importance of the seated condylar position in orthodontic correction. Quintessence Int. 2002;33:284–293. [PubMed] [Google Scholar]
- 21.Alexander SR, Moore RN, DuBois LM. Mandibular condyle position: comparison of articulator mountings and magnetic resonance imaging. Am J Orthod Dentofacial Orthop. 1993;104:230–239. doi: 10.1016/S0889-5406(05)81724-X. [DOI] [PubMed] [Google Scholar]
- 22.Levine D, Gosink BB. Ultrasound shows changes in postmenopausal pelvis. Diagn Imaging (San Franc) 1992;14:96–101. [PubMed] [Google Scholar]
- 23.Karl PJ, Foley TF. The use of a deprogramming appliance to obtain centric relation records. Angle Orthod. 1999;69:117–124. doi: 10.1043/0003-3219(1999)069<0117:TUOADA>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Burke G, Major P, Glover K, Prasad N. Correlations between condylar characteristics and facial morphology in Class II preadolescent patients. Am J Orthod Dentofacial Orthop. 1998;114:328–336. doi: 10.1016/s0889-5406(98)70216-1. [DOI] [PubMed] [Google Scholar]
- 25.Helkimo M. Epidemiological surveys of dysfunction of the masticatory system. Oral Sci Rev. 1976;7:54–69. [PubMed] [Google Scholar]
- 26.Fantini SM, Paiva JB, Rino Neto J, Dominguez GC, Abrão J, Vigoritto JW. Increase of condylar displacement between centric relation and maximal habitual intercuspation after occlusal splint therapy. Braz Oral Res. 2005;19:176–182. doi: 10.1590/s1806-83242005000300004. [DOI] [PubMed] [Google Scholar]
- 27.Baccetti T, Franchi L, McNamara JA., Jr The Cervical Vertebra Maturation (CVM) method for the assessment of the optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005;11:119–129. [Google Scholar]
- 28.Ramalhão MJ. Deslocamento condilar nos tipos faciais hiperdivergentes [Thesis] Porto: University of Porto; 2009. [Google Scholar]
- 29.Wood DP, Floreani KJ, Galil KA, Teteruck WR. The effect of incisal bite force on condylar seating. Angle Orthod. 1994;64:53–61. doi: 10.1043/0003-3219(1994)064<0053:TEOIBF>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 30.McNamara JA, Jr, Seligman DA, Okeson JP. Occlusion, Orthodontic treatment, and temporomandibular disorders: a review. J Orofac Pain. 1995;9:73–90. [PubMed] [Google Scholar]