

Abstract
Pancreatic carcinoma is a debilitating disease and carries a poor prognosis. It is a rare cause of upper gastrointestinal bleeding, even though pancreas, stomach, duodenum and jejunum are adjacent organs. The incidence of pancreatic adenocarcinoma directly invading the gastrointestinal tract leading to gastrointestinal hemorrhage is very low, and most of them present with melena and hematochezia. Here, we describe one unique case manifesting characteristically severe and unremitting hematemesis as an initial presentation of pancreatic adenocarcinoma. This tumor directly invaded the duodenal mucosa as a bleeding protruding tumor mass. Our MEDLINE search has confirmed that this is the first reported case with an initial manifestation of hematemesis from pancreatic adenocarcinoma in Asians. Pancreatic adenocarcinoma directly invading duodenum complicated by hemorrhage can be a rare cause of hematemesis, and clinicians should be reminded of it while they are making differential diagnosis.
Keywords: Pancreatic adenocarcinoma, Duodenum tumor, Hematemesis, Neoplasm invasiveness
INTRODUCTION
Pancreatic carcinoma is very common in developed countries. This tumor carries a poor prognosis, behaves devastatingly, and often invades the contiguous organs, which in turn results in 4 major symptoms: obstructive jaundice, duodenal obstruction, weight loss, and cancer pain[1-8]. The main symptoms usually result from external compression of duodenal serosal side or common bile duct by pancreatic carcinoma, frequently requiring palliative management clinically. However, direct invasion to gastrointestinal tract by pancreatic adenocarcinoma, while rare, has been reported[9,10]. The incidence was 2.6% in an American retrospective series, and the commonest symptoms were tarry stool passage and hematochezia[9]. Up to date, only one case manifesting hematemesis as the initial presentation of pancreatic adenocarcinoma has been reported[9]. Herein, we reported the first case in Orientals.
CASE REPORT
A 77-year-old man suffered from nausea, epigastric fullness and pain, dizziness, and body weight loss of 15 kg over a three-month period. Physical examination was otherwise unremarkable, except for moderate tenderness over the epigastrium. Abdominal sonography showed mild dilatation of the pancreatic duct and multiple hepatic masses over both lobes. Computed tomography of the abdomen disclosed a 3 cm×3 cm mass over the pancreatic head that could not be distinguished from the adjacent duodenal wall, and multiple liver metastases (Figure 1). The upper gastrointestinal endoscopy revealed a polypoid mass, protruding over the anterior wall of the duodenal bulb with partial obstruction of the duodenal lumen (Figure 2). During this examination, endoscopy-assisted contrast medium infusion was performed through the stricture segment of duodenum, which was requested by radiologists to facilitate fine needle biopsy of pancreatic tumor later. Endoscopically biopsied tissues revealed adenocarcinoma (Figure 3A). The patient next received a computed tomography-guided biopsy for pancreatic lesion which was proved to be a moderately differentiated adenocarcinoma (Figure 3B). The morphology was quite compatible with the previous endoscopic specimen. Thus, the diagnosis of pancreatic adenocarcinoma with invasion of duodenal mucosa was virtually established.
Figure 1.

A soft tissue mass (3 cm×3 cm in size) over the pancreatic head (arrow), duodenal infiltration (arrowhead), and superior mesenteric vein encasement shown by abdominal computed tomography.
Figure 2.

A soft polypoid mass protruding over the anterior wall of the duodenal bulb with partial obstruction of the second portion of the duodenum shown by upper gastrointestinal endoscopy.
Figure 3.
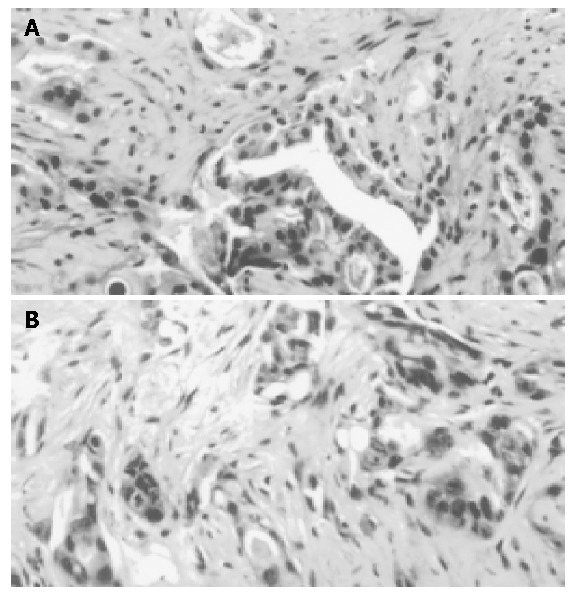
Morphology of adenocarcinoma and pancreatic lesion. A: Biopsy of the duodenal tumor via upper gastrointestinal endoscopy revealed a picture of adenocarcinoma cells in an acinar pattern; B: Biopsy of the pancreatic head tumor via computed tomography-guidance showed moderately differentiated adenocarcinoma cells infiltrating into the collagenous stroma (hematoxylin and eosin stain; magnification ×200).
Unfortunately, hematemesis and tarry stool developed six days after admission. Intravenous fluid resuscitation and blood transfusion with packed red cells were administered. An urgent upper gastrointestinal endoscopy observed a tumor invasion with blood oozing over the anterior wall of the first and second portions of the duodenum. Local epinephrine injection was then employed, and bleeding was temporarily stopped. Approximately three weeks after the episode of upper gastrointestinal bleeding, obstructive jaundice and cholangitis developed. He then received palliative percutaneous transhepatic drainage to relieve obstructive jaundice. In addition, palliative radiotherapy and adjuvant chemotherapy with 5-fluorouracil and gemcitabine were administered for one week. However, finally the patient expired six weeks later due to cachexia, sepsis and multiple organ failure.
DISCUSSION
Pancreatic carcinoma is becoming more and more prevalent in Asia. It has been the tenth leading cause of death from cancer in Taiwan in 2002[11]. The one-year survival rate is reported to be about 8%. The clinical course is poor, and the median survival time is about 3-5 mo. About 80% of patients with pancreatic cancer, at the time of diagnosis, were far advanced and unresectable[12]. Regarding palliative therapeutic strategy in advanced pancreatic carcinoma, gemcitabine is a strongly recommended drug of choice by an updated study[1]. We also applied this promising drug to our patient. However, the patient still expired due to a poor general condition and relentless disease progress six weeks after diagnosis eventually.
Pancreatic malignancy may have a variety of presentations. The most common clinical manifestations are jaundice, pruritus, abdominal pain, body weight loss, anorexia, and nausea[3,13,14]. Obstructive symptoms, either obstructive jaundice or duodenal obstruction, are not rare manifestations of pancreatic carcinoma while massive gastrointestinal hemorrhage is seldom encountered[3,9,10,13,14]. By summarization from literature, there are three mechanisms for the pathogenesis, either by gastric variceal bleeding secondary to splenic vein occlusion[15-17], a fistula from the blood vessel to duodenum (namely wirsungorrhage)[18,19], or direct tumor bleeding via the pancreatic duct (namely hemosuccus)[20,21]. However, in our case, the pancreatic tumor extending to the duodenum was evident from the abdominal CT image, where the patient experienced massive hematemesis. In addition, the pathologic results from both the biopsies of the pancreatic tumor and the duodenal intraluminal protruding mass were quite compatible. Therefore, the diagnosis of pancreatic adenocarcinoma directly invading the duodenum, complicated by upper GI bleeding, was confirmed. In contrast to the clear elucidation of pancreatic parenchymal neoplasms manifesting hematemesis[20-23], pancreatic ductal carcinoma presenting with upper gastrointestinal bleeding has been rarely reported, and common symptoms are melena and hematochezia. To the best of our knowledge, there has been only one case of pancreatic adenocarcinoma presenting with hematemesis reported[9]. These two patients’ clinical manifestations are shown in Table 1. One of them (our case) presented with a polypoid mass from tumor infiltration of duodenal mucosa, while the other failed to have positive finding from upper gastrointestinal endoscopy due to its deep location in the third portion of duodenum.
Table 1.
Clinical features of patients with pancreatic adenocarcinoma directly invading the duodenum complicated by upper gastrointestinal bleeding.
| Our patient | Lee et al1 | |
| Age (yr) | 78 | 83 |
| Sex | Male | Female |
| Clinical manifestation | Massive gastrointestinal bleeding (hematemesis) | Persistent gastrointestinal bleeding (hematemesis) |
| Endoscopic finding | Polypoid mass | Normal |
| Location of tumor invasion | The first and second portions of duodenum | The third portion of duodenum |
| Treatment | Radiotherapy, chemotherapy | Not mentioned |
| Survival duration | Six weeks | Not mentioned |
Reference 9.
The pancreatic tumor was located in the retroperitoneal space, and was somewhat difficult to approach by fine needle biopsy. Using the assistant method of endoscopy-assisted contrast medium infusion through the constrictive segment of duodenum to define the accurate tumor location, we successfully obtained tumor tissue from the pancreas.
In conclusion, pancreatic carcinoma may present with a varying spectrum of gastrointestinal bleeding, including hematemesis, which is easily overlooked by clinicians. Prompt endoscopic examination, including judicious scrutiny of the first and second portions of the duodenum, together with tissue biopsy may provide imperative information for early detection and enable selection of appropriate treatment.
Footnotes
Edited by Wang XL Proofread by Zhu LH
References
- 1.Storniolo AM, Enas NH, Brown CA, Voi M, Rothenberg ML, Schilsky R. An investigational new drug treatment program for patients with gemcitabine: results for over 3000 patients with pancreatic carcinoma. Cancer. 1999;85:1261–1268. [PubMed] [Google Scholar]
- 2.Mu DQ, Peng SY, Wang GF. Risk factors influencing recurrence following resection of pancreatic head cancer. World J Gastroenterol. 2004;10:906–909. doi: 10.3748/wjg.v10.i6.906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Selch MT, Parker RG. Results in the management of locally unresectable pancreatic carcinoma. Am J Clin Oncol. 1986;9:139–145. doi: 10.1097/00000421-198604000-00008. [DOI] [PubMed] [Google Scholar]
- 4.Bungay K, Dennistone S, Hunt PS. Duodenal obstruction and carcinoma of the head of pancreas. Med J Aust. 1980;2:150–151. doi: 10.5694/j.1326-5377.1980.tb76948.x. [DOI] [PubMed] [Google Scholar]
- 5.Lichtenstein DR, Carr-Locke DL. Endoscopic palliation for unresectable pancreatic carcinoma. Surg Clin North Am. 1995;75:969–988. doi: 10.1016/s0039-6109(16)46740-x. [DOI] [PubMed] [Google Scholar]
- 6.Bakkevold KE, Kambestad B. Palliation of pancreatic cancer. A prospective multicentre study. Eur J Surg Oncol. 1995;21:176–182. doi: 10.1016/s0748-7983(95)90402-6. [DOI] [PubMed] [Google Scholar]
- 7.Egrari S, O'Connell TX. Role of prophylactic gastroenterostomy for unresectable pancreatic carcinoma. Am Surg. 1995;61:862–864. [PubMed] [Google Scholar]
- 8.Scott-Mackie P, Morgan R, Farrugia M, Glynos M, Adam A. The role of metallic stents in malignant duodenal obstruction. Br J Radiol. 1997;70:252–255. doi: 10.1259/bjr.70.831.9166049. [DOI] [PubMed] [Google Scholar]
- 9.Lee P, Sutherland D, Feller ER. Massive gastrointestinal bleeding as the initial manifestation of pancreatic carcinoma. Int J Pancreatol. 1994;15:223–227. doi: 10.1007/BF02924198. [DOI] [PubMed] [Google Scholar]
- 10.Sharon P, Stalnikovicz R, Rachmilewitz D. Endoscopic diagnosis of duodenal neoplasms causing upper gastrointestinal bleeding. J Clin Gastroenterol. 1982;4:35–38. doi: 10.1097/00004836-198202000-00006. [DOI] [PubMed] [Google Scholar]
- 11.Department of Health, Executive Yuan, Republic of China, General Health Statistic, 2002. Leading causes of death from cancers, Taiwan area, 2002, Health and Vital Statistics [Google Scholar]
- 12.Tepper JE, Noyes D, Krall JM, Sause WT, Wolkov HB, Dobelbower RR, Thomson J, Owens J, Hanks GE. Intraoperative radiation therapy of pancreatic carcinoma: a report of RTOG-8505. Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys. 1991;21:1145–1149. doi: 10.1016/0360-3016(91)90269-a. [DOI] [PubMed] [Google Scholar]
- 13.Lillemoe KD, Pitt HA. Palliation. Surgical and otherwise. Cancer. 1996;78:605–614. doi: 10.1002/(SICI)1097-0142(19960801)78:3<605::AID-CNCR41>3.0.CO;2-#. [DOI] [PubMed] [Google Scholar]
- 14.Lillemoe KD. Palliative therapy for pancreatic cancer. Surg Oncol Clin N Am. 1998;7:199–216. [PubMed] [Google Scholar]
- 15.Ferguson JM, Palmer KR, Garden OJ, Redhead DN. Transhepatic venous angioplasty and stenting: a treatment option in bleeding from gastric varices secondary to pancreatic carcinoma. HPB Surg. 1997;10:173–175. doi: 10.1155/1997/18272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McDermott VG, England RE, Newman GE. Case report: bleeding gastric varices secondary to splenic vein thrombosis successfully treated by splenic artery embolization. Br J Radiol. 1995;68:928–930. doi: 10.1259/0007-1285-68-812-928. [DOI] [PubMed] [Google Scholar]
- 17.Mullan FJ, McKelvey ST. Pancreatic carcinoma presenting as bleeding from segmental gastric varices: pitfalls in diagnosis. Postgrad Med J. 1990;66:401–403. doi: 10.1136/pgmj.66.775.401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Thorstad BL, Keller FS. Fistula from the superior mesenteric artery to duodenum: a rare cause of death from pancreatic carcinoma. Gastrointest Radiol. 1987;12:200–202. doi: 10.1007/BF01885141. [DOI] [PubMed] [Google Scholar]
- 19.Ghaphery AD, Gupta R, Currie RA. Carcinoma of the head of the pancreas with aortoduodenal fistula. Am J Surg. 1966;111:580–583. doi: 10.1016/0002-9610(66)90289-3. [DOI] [PubMed] [Google Scholar]
- 20.Clay RP, Farnell MB, Lancaster JR, Weiland LH, Gostout CJ. Hemosuccus pancreaticus. An unusual cause of upper gastrointestinal bleeding. Ann Surg. 1985;202:75–79. doi: 10.1097/00000658-198507000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Baruch Y, Levy Y, Goldsher D, Munichor M, Eidelman S. Massive haematemesis--presenting symptoms of cystadenocarcinoma of the pancreas. Postgrad Med J. 1989;65:42–44. doi: 10.1136/pgmj.65.759.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Goldenberg AM, Present DH, Bauer J, Gordon R. Islet cell tumor presenting as massive upper gastrointestinal bleeding in pregnancy. Am J Gastroenterol. 1988;83:873–875. [PubMed] [Google Scholar]
- 23.Sacks MI. Pancreatic tumor with repeated gastrointestinal hemorrhage and steatorrhea. Isr J Med Sci. 1965;1:141–148. [PubMed] [Google Scholar]