

Abstract
Cardiac myxoma, the most common primary heart tumor, is located mainly in the left atrium. We reported a rare case of left ventricular myxoma incidentally found on echocardiography in an asymptomatic 60-year-old male. The tumor was carefully resected without fragmentation. The patient had an uneventful recovery and was discharged home on the 4th postoperative day. Surgical resection of this type of cardiac myxoma is recommended due to the rarity of tumor location.
Keywords: left ventricular myxoma, echocardiography, resection
INTRODUCTION
Primary cardiac tumors are rare and are most commonly myxomas. The majority of myxomas are in the left atrium (75%) followed by the right atrium (20%). In rare cases, myxomas can be found in the ventricles, with 2.5% reported for myxomas in the left ventricle[1]. The most common symptoms include embolism, intracardiac obstruction and constitutional symptoms. Occasionally, patients are asymptomatic and are diagnosed unexpectedly[2]. Diagnosis is primarily made by echocardiography, or transoesophageal echocardiography (TEE), or magnetic resonance imaging (MRI), and treatment is surgical excision as soon as the diagnosis is confirmed. We presented a case of left ventricular myxoma who was successfully managed by surgical resection.
CASE REPORT
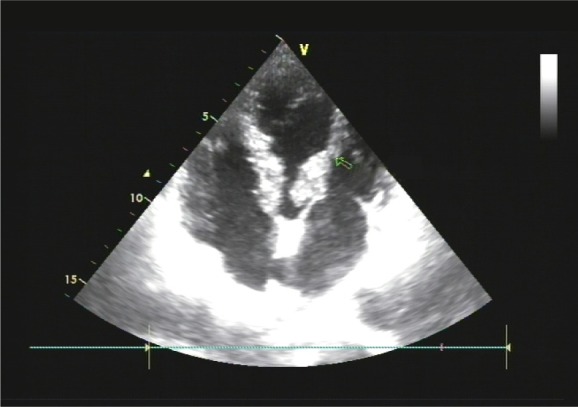
A 60-year-old male patient from Jiangsu province, China, was admitted to our hospital on January 4th, 2012. The patient underwent a routine medical examination and a myxoma was detected in the left ventricle by echocardiography. As he had a history of hepatic cirrhosis, TEE was not performed. Physical examination showed normal heart sounds without any murmur. There was no history of syncope, palpitation, or dyspnea. On reviewing the echocardiogram, the tumor was attached by a pedicle to a square centimeter insertion area at the base of the anterolateral papillary muscle, which swung back and forth in the left ventricular outflow tract (Fig. 1). Initial laboratory examination showed normal findings other than elevations in glutamic oxalacetic transaminase (98 U/L) and glutamic pyruvic transaminase (85 U/L), but the values returned to normal before surgery. CT angiography of the chest, abdomen and pelvis were obtained. The aorta extending down to the femoral vessels was found to be free from any lesions.
Fig. 1. Echocardiogram demonstrating a left ventricular mass in a 62-year old asymptomatic male patient. The arrow indicates a pedunculated mass. The arrow shows a pedicle.
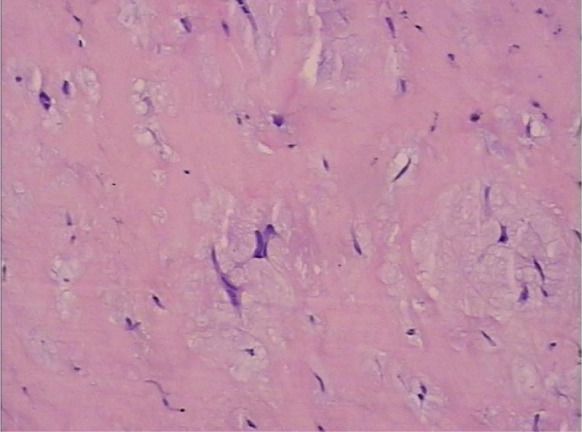
Surgical resection was performed by median sternotomy, aorto-bicaval cardiopulmonary bypass and normothermic anterograde blood cardioplegia. The protocol was approved by the local institutional board at the authors' affiliated institution and patient consent was obtained. After transverse aortotomy, a translucent fragile jelly-like myxoma became visible in the left ventricular outflow tract through the aortic cusps. The tumor adhered to the base of the anterolateral papillary muscle and was completely removed without fragmentation. The postoperative course of the patient was uneventful. Histopathologic examination is consistent with the diagnosis of a myxoma (Fig. 2). We followed up the patient for 3 months, and the patient had no recurrence of myxoma.
Fig. 2. Histopathologic examination confirms the diagnosis of myxoma (H&E, ×100).
DISCUSSION
Primary cardiac tumours are extremely rare. In autopsy series, the incidence of primary cardiac tumors is 0.0017% and 0.19%. Nearly 75% of them are benign and most of the benign heart tumors are myxomas[3]. In spite of the benign histological character of these tumors, they can lead to unfavorable consequences. These tumors could aggravate preexisting complications or could even lead to sudden death due to their fragmentatibility or valve obstruction[3],[4],[5]. The growth rate of myxomas has been cited as reaching 0.15 cm per month[2]. Surgical treatment should be performed as soon as the diagnosis is confirmed even through there were no signs of embolism and obstruction.
The selection of surgical incision for left ventricular myxoma depends on its location. In this case, the myxoma adhered to the base of the anterolateral papillary muscle and moved freely in the left ventricular outflow tract. Therefore, we made the aortic incision and could see the myxoma easily. Robert et al. chose a transmitral procedure and found that the mitral valve and its chordae tendineae could not be preserved at its location[3]. Arruda et al. removed a left ventricular myxoma with a 4-cm incision in the left ventricular lateral wall[5]. However, in our opinion, it is better to avoid ventriculotomy due to its potential complications. Furthermore, if necessary, exploration via the right atrium and atrial septum may be performed, so aorto-bicaval cardiopulmonary bypass is better. Careful handling of the cardiac structures and tumor during its removal reduces the possibility of fragmentation and the occurrence of embolic phenomenon during the surgery. The resection of the base of the tumor implantation should be performed with good safety margin to avoid recurrence. Most importantly, care should be taken not to injure the valve, chordae tendineae and papillary muscle.
In conclusion, left ventricular myxoma can be diagnosed readily by echocardiography and should be resected as early as possible. Tumor resection is safe with appropriate incision and careful handling.
References
- 1.Mohammed Hassan, J. Michael Smith. Robotic assisted excision of a left ventricular myxoma. Interact Cardiovasc Thorac Surg. 2012;14:113–4. doi: 10.1093/icvts/ivr021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rendón F, Agosti J, Llorente A, Rodrigo D, Montes K. Intramural cardiac myxoma in left ventricular wall: an unusual location. Asian Cardiovasc Thorac Ann. 2002;10:170–2. doi: 10.1177/021849230201000220. [DOI] [PubMed] [Google Scholar]
- 3.Jens Robert, Martin Brack, Stephan Hottinger, Alexander Kadner, Hans-Rudolf Baur. A rare case of left ventricular cardiac myxoma with obstruction of the left ventricular outflow tract andatypical involvement of the mitral valve. Eur J Echocardiogr. 2009;10:593–5. doi: 10.1093/ejechocard/jep031. [DOI] [PubMed] [Google Scholar]
- 4.Enrico Natale, Giovanni Minardi, Giovanni Casali, Giovanni Pulignano, Francesco Musumeci. Left ventricular myxoma originating from the interventricular septum and obstructing the left ventricular outflow tract. Eur J Echocardiogr. 2008;9:84–5. doi: 10.1016/j.euje.2007.01.007. [DOI] [PubMed] [Google Scholar]
- 5.Arruda MV, Braile DM, Joaquim MR, Soares MJ, Alves RH. Resection of left ventricular myxoma after embolic stroke. Rev Bras Cir Cardiovasc. 2008;23:578–80. doi: 10.1590/s0102-76382008000400022. [DOI] [PubMed] [Google Scholar]