

Abstract
Background:
Eunuchs are considered as the most vulnerable, frustrated, and insecure community. The accessibility to medical and dental facilities for the eunuchs is nearly nonexistent. Due to these reasons, they might be at a high risk of developing severe dental problems like tooth loss.
Aim:
The present cross-sectional study aimed to evaluate the dental prosthetic status and prosthetic needs among eunuchs residing in Bhopal city, Madhya Pradesh, India.
Subjects and Methods:
On the basis of convenient nonprobability snowball sampling technique, all the self-identified eunuchs residing in the city of Bhopal along with a matched control consisting of cross section of the general population residing in the same locality was examined to evaluate the prosthetic status and prosthetic needs of the population. All the obtained data were entered into a personal computer on Microsoft excel sheet and analyzed using the software; Statistical Package for Social Science version 20. Data comparison was done by applying Chi-square test.
Results:
A total of 639 subjects comprised of 207 eunuchs, 218 males and 214 females. Among all participants, 2.8% (18/639) were having prosthesis. The overall prosthetic status among males was 3.2% (7/218) followed by 2.9% (6/207) eunuchs and 2.3% (5/214) females. However, need for multi-unit and combination of one and more unit prosthesis for upper and lower jaws was higher in males compared to females and eunuchs, but the difference was not statistically significant.
Conclusion:
The findings of this study clearly demonstrate a high unmet need for prosthetic care among the population surveyed.
Keywords: Eunuchs, Prosthetic needs, Prosthetic status, Trans genders
Introduction
Oral health is always an inseparable part of general health and awareness plays a vital role in determining the oral health of the individual. Tooth loss especially, complete loss or edentulism, is equivalent to the dental death.[1] Much like the fact that decline in activities of daily living[2] is a final common pathway for a broad range of decrements in general health, tooth loss constitutes a final common pathway for most dental diseases and conditions. This tooth loss can lead to substantial impacts on quality-of-life.[3]
Tooth loss is mainly attributed to dental caries and periodontal diseases, but psychosocial factors as well as age, gender, lifestyle (dietary habit, smoking, alcohol intake, etc.) and oral health behavior may modify the progression of these disorders.[4]
Similarly, the loss of teeth also reflects the attitudes of the patients, the dentists in a society, the availability and accessibility of dental care as well as the prevailing philosophies of care.[5] It have been suggested by several authors that the loss of teeth could be a disturbing emotional experience for many people.[6,7,8] Some people associate the loss of teeth with growing old, which may be emotionally depressing.
Naturally, in an effort to prevent or ameliorate some of these decrements in oral health-related quality-of-life, dentists frequently recommend removable or fixed prosthetic treatment for tooth loss. Restoration of missing teeth by appropriate prosthetic treatment is important for the rehabilitation of oral function, chewing ability, esthetic, and maintenance of oral and general health.[9]
In order to promote the oral health, we need to know the prosthetic status and a prosthetic need of the population. Socioeconomically disadvantaged groups rate their oral health poorer than more advantaged groups and report more tooth loss and more problems with their teeth, mouth or dentures.[10] Eunuchs (transgenders) are one of the highly stigmatized, poverty-stricken, special vulnerable groups in India where special attention is required to improve the overall oral health scenario of the country.
The word “Eunuch” is derived from the Greek word meaning “keeper of the bed.”[11] These transgender communities historically exist in many cultural contexts, known as bakla in the Philippines, xaniths in Oman, serrers among the Pokot people of Kenya, and kinnars, jogappas, jogtas, or shiv-shaktis in South Asia.[12]
In India, eunuchs are also called as “Hijra,” which actually refers to third gender or “male-to-female” transgender people, most see themselves as neither men nor women.[11] Many Hijra come from other sexually ambiguous backgrounds: They may be born inter-sexed, be born male or female and fail to develop fully at puberty.[11,12] According to Telegraph report, India has an estimated 1.5 million eunuchs.[13] However, the census data on them does not exist, so to make an accurate enumeration is impossible as they continue to persist as a marginalized and secretive community.[12] They generally live together by forming a group called as “Gharana” (familial house to which they owe allegiance) which is headed by a Guru (most senior member), and other members are as “Chelas” (followers).[13] Their sources of livelihood mainly include performing at marriage and birth celebrations, badhai (ritual performing) basti/mangti (begging) for alms and prostitution.[11]
They are considered as the most vulnerable, frustrated, and insecure community of the country.[12,13] They are denied general, oral health and psychological assistance[12] and the accessibility to medical and dental facilities for the eunuchs is nearly nonexistent.
Due to these reasons, they might be at a high risk of developing severe dental problems like tooth loss. However, there have been no studies evaluating the prosthetic status and treatment needs of eunuchs. A sincere effort has been made to collect baseline information to formulate policy, to plan, to monitor and evaluate oral health services for eunuch population. Thus, the present study was undertaken with an aim to evaluate the dental prosthetic status and prosthetic needs among eunuchs residing in Bhopal city, Madhya Pradesh, India.
Subjects and Methods
A cross-sectional study following the Strengthening the reporting of observational studies in epidemiology[14] guidelines was conducted among the eunuchs of Bhopal city, Madhya Pradesh, India.
Ethical clearance
The detailed proposed study protocol was submitted and approved by the ethical committee of Peoples University, Bhopal.
Informed consent
A brief study protocol was explained and written informed consent was taken from each study subject before the oral examination.
Source of data
The study subjects consisted of self-identified eunuchs residing in the Bhopal city. A matched control is consisting of cross-section of the general population residing in the same locality where these eunuchs live was also examined.
Sampling design and sample selection
Based on convenient nonprobability snowball sampling technique, all the self-identified eunuchs residing in the city of Bhopal who were present at the time of examination and who full filled the selection criteria were examined. Based on interviews with local informants, four prominent localities of the city where most of the eunuchs reside were identified. These areas were Mangalwara, Budhwara, Patra, and Ahamadpur kala. All the identified areas were visited and eunuchs residing in these areas were contacted. The eunuchs who consented to become part of the study guided us to the similar samples they knew about. The subjects were explored until saturation occurs, and no new cases were identified.
A cross-section of the general population (males and females) residing in the same locality where these eunuchs live was also examined. All the eligible males and females were matched with eunuchs for pertinent variables such as age, sex, and geographical distribution.
Selection criteria
Inclusion criteria
Eunuchs: All the self-identified eunuchs available during the study period were considered for the study
The matched controls with the eunuchs for certain pertinent variables like age, sex and geographical distribution
Participants who gave informed consent to participate at the time of study.
Exclusion criteria
Participants with a history of medication for any systemic illness (medically compromised patients)
Participants not willing to participate in the study
Participants affected with mental retardation, physically and mentally handicapped, orthopedic defects, etc.
Sample size
A total of 639 subjects comprised of 207 eunuchs, 218 males and 214 females residing in the city of Bhopal, Madhya Pradesh India were examined.
Schedule of the survey
A survey was systematically scheduled to cover all the identified areas of the Bhopal city. The survey period extended for a period of 3 months from April to June 2013.
Method of collection of data
Information on demographic characteristics such as age, sex, occupation and socioeconomic status (SES) (modified Kuppuswamy's scale 2012) were collected, which was based on the primary objective of the study.
Clinical examination
World Health Organization (WHO) oral health assessment proforma (1997)[15] was used to collect the information on prosthetic status and treatment needs. The clinical examination through the survey was carried out by the principal investigator. The investigator read, understood and standardized his method of operation so as to minimize error and have reproducible data. A recording clerk was trained to assist in the recording procedure throughout the survey. Clinical examinations were carried out in the living environments; these included Deras (for eunuchs), private and rented out rooms (for controls) where subjects reside.
Clinical examination was performed by using a plane mouth mirror and CPI probe under adequate natural light. An examination of the oral cavity for the loss of teeth was made on every subject. The examination was performed in the following sequence.
Evaluation of prosthetic status
The presence of the prosthesis was recorded for each jaw. The codes and criteria were as following:
0- No prosthesis
1- Bridge
2- More than one bridge
3- Partial denture
4- Both bridge (s) and partial denture (s)
5- Full removable denture
9- Not Recorded.
Evaluation of prosthetic needs
The recording was made for each jaw for the need of the prosthesis, according to following codes:
0- No prosthesis needed
1- Need for one unit prosthesis (one tooth replacement)
2- Need for multi-unit prosthesis (more than one tooth replacement)
3- Need for a combination of one-and/or multi-unit prosthesis
4- Need for full prosthesis (replacement of all teeth)
9- Not recorded.
Statistical analysis
All the obtained data were entered into a personal computer on Microsoft excel sheet and analyzed using the software; Statistical Package for Social Science (SPSS; IBM, USA) version 20. Data comparison was carried outt by applying Chi-square test. The statistically significant level was fixed at P < 0.05.
Results
A total of 639 subjects were distributed into 3 groups that are, 34.1% (218/639) males, 33.5% (214/639) females, and 32.4% (207/639) eunuchs. The difference was not statistically significant [Graph 1].
Graph 1.
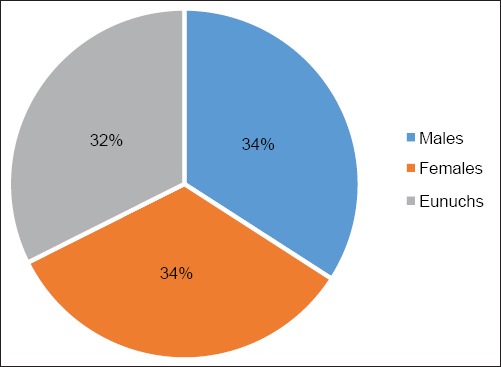
Distribution of subjects according to gender
The mean age of the study participants were 38.17 (12.4) for males, 38.14 (12.3) for females and 36.86 (12.5) for eunuchs. The difference between mean ages was not statistically significant. Among all the study participants, the highest number of subjects, that is, 45.7% (292/639) were in the age group of <34 years while, 3.4% (24/639) of the study participants belonged to age group above 65 years. The difference was not statistically significant (P = 0.40, 95% CI) [Graph 2].
Graph 2.
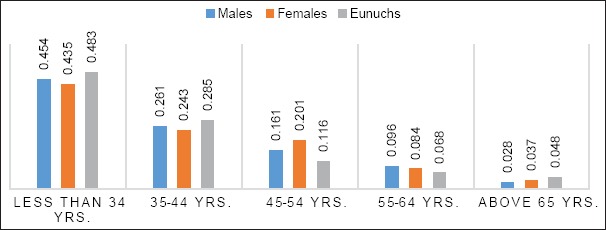
Distribution of subjects according to age groups
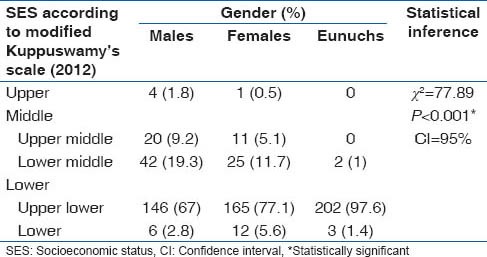
Majority of the study participants belonged to upper lower socioeconomic group which comprised of 97.6% (202/207) eunuchs, 77.1% (165/214) females and 67% (146/218) males. The difference in distribution of SES among genders was statistically significant (P < 0.001, 95% CI) [Table 1].
Table 1.
The distribution of gender according to SES
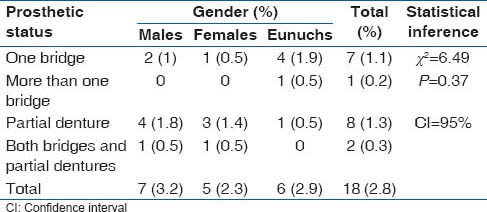
Among 639 participants, 2.8% (18/639) were having prosthesis. The overall prosthetic status among males was 3.2% (7/218) followed by 2.9% (6/207) eunuchs and 2.3% (5/214) females. The difference was not statistically significant (P = 0.37, 95% CI) [Table 2].
Table 2.
The distribution of gender according to prosthetic status
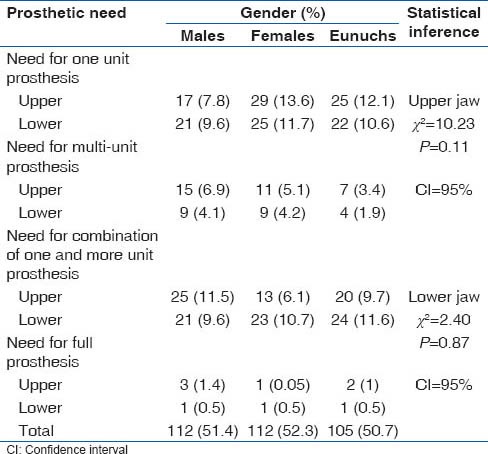
Very few subjects were in need of full prosthesis. However, the need for single unit prosthesis was highest that is, 21.8% (139/639). The need for one unit prosthesis was highest among females while, eunuchs and males were required more multiunit prosthesis. The difference in the prosthetic need among gender was not statistically significant [Table 3].
Table 3.
The distribution of gender according to prosthetic need
Discussion
The current cross-sectional, epidemiological survey was conducted to evaluate the prosthetic status and prosthetic needs of Eunuchs (Hijra) residing in Bhopal city, Madhya Pradesh, India. This was the first of its kind, unique, a pioneering study that revealed the oral health related information of eunuch/Hijra (third gender) community. The oral examination was conducted using WHO oral health assessment proforma 1997. A total of 639 subjects comprising of 207 eunuchs, 218 males and 214 females were recruited in the study. The mean age of the study subjects was 37.7 years and no significant difference was observed in the distribution of age among gender.
A different sampling technique, that is, “snowball sampling” was adopted for this study. As eunuch (Hijra) community is highly secretive and hidden community, very little is known about them. Such kind of “Hidden populations” have two characteristics: First no sampling frame exists, so the size and boundaries of the population are unknown; and second, there exist strong privacy concerns, because membership involves stigmatized or illegal behavior, leading individuals to refuse to co-operate or give unreliable answers to protect their privacy.[16] Traditional methods, such as household surveys cannot produce reliable samples, and they are inefficient, because most hidden populations like eunuchs are rare. Accessing such populations is difficult because standard probability sampling methods produce low response rates and responses that lack candor.[17] Due to these reasons snowball sampling was the best method available for our study. However, snowball sampling design has some limitations, there might be a chance that samples obtained in our study tend to be biased toward the most cooperative subjects who agree to participate. Similarly, it is based on convenience sampling procedure so, our analysis was limited to proportions of the sample and was not generalizable.
In the present study, only 2.8% of the subjects had prosthesis in upper or lower arch. These findings are lesser than findings reported by Bharadwaj et al.[18] where 10.3% had prosthesis in either upper or lower arch. The reason for this difference in prosthetic status between the present and past study may be due to the reason that our study population comprised of adults with low SES. Similar reason was observed by Bharadwaj et al.[18] The social pressure of maintaining the esthetics and function may be the driving force that influences the subjects in the upper class to get their missing teeth replaced.[19] In addition to this, the attitude and awareness toward dental care, and the cost of dental treatment might also be the significant factor that determines the prosthetic status of a person.[20] It was also observed that there was a minimal variation between the sexes regarding the status for maxillary and mandibular arches. However, the difference was not statistically significant. This is in accordance with the findings of Mersel et al.[21] and Shroff.[22]
The estimation of treatment need is an important stage in oral health care planning. Prosthetic needs of our study were high. Almost 51.5% of the subjects were in need of either fixed, removable or combined prosthodontic treatment, and there was no statistically significant difference among gender. These findings are lower than those observed by Shah et al.[23] where 72% subjects needed at least one kind of prosthodontics treatment. The reason for this great difference in prosthetic needs may be due to the reason that our majority of study population was comprised of adults with >54 years of age.
In the current study, the need for single-unit prostheses (21.75%) was more than other prostheses that was in contrast with the study by Shenoy and Hegde[24] in Mangalore where the need for multi-unit prostheses was more than the need for 1-unit prostheses. The need for one unit prosthesis was highest among females while, eunuchs and males were required more multi-unit prosthesis. This indicates a higher prevalence of multiple tooth loss among eunuchs and males. However, the greatest need observed in oldest age group may be due to teeth missing from periodontal disease whereas for the youngest age group it may be due to teeth missing from dental caries.
Hence, it can be concluded that most of the prosthetic needs of the study population were unmet with prosthetic needs (51.5%) being approximately seventeen and half folds greater than the prosthetic status (2.8%). The lack of social pressure and attitude to maintain the teeth in good health may be the factors responsible for the lack of utilization as well as lack of awareness on the provision of reimbursement for dental care among the subjects in the lower classes. This highlights the fact that the lower SES people may not utilize the services even if the cost barrier is removed.[25,26] SES adds a new dimension to the entire process of program planning. As an expression of attitudes, community groups, particularly the underprivileged like eunuchs, have clear feelings about the priorities in the health care field and the way the healthcare is rendered.[27]
Conclusion
The findings of this study clearly demonstrate a high unmet need for prosthetic care among the population surveyed. To improve the oral health status, it is necessary to provide oral health education and importance of prosthetic treatment. Centers for free dental treatment should be set up for socially deprived communities like eunuchs, who need prosthetic treatment but cannot afford the treatment. However, further studies with less biased sampling techniques like respondent-driven sampling are needed at a large scale to collect the baseline oral health data and to plan prosthetic services for eunuchs.
Acknowledgments
The present study was self-funded by the authors. Furthermore, we the authors of this study; thank all the eunuchs who took part in this study for their co-operation.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Patil VV, Shigli K, Hebbal M, Agrawal N. Tooth loss, prosthetic status and treatment needs among industrial workers in Belgaum, Karnataka, India. J Oral Sci. 2012;54:285–92. doi: 10.2334/josnusd.54.285. [DOI] [PubMed] [Google Scholar]
- 2.Jiang Y, Okoro CA, Oh J, Fuller DL. Sociodemographic and health-related risk factors associated with tooth loss among adults in Rhode Island. Prev Chronic Dis. 2013;10:E45. doi: 10.5888/pcd10.110285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hanioka T, Ojima M, Tanaka K, Matsuo K, Sato F, Tanaka H. Causal assessment of smoking and tooth loss: A systematic review of observational studies. BMC Public Health. 2011;11:221. doi: 10.1186/1471-2458-11-221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shigli K, Hebbal M, Angadi GS. Prosthetic status and treatment needs among patients attending the prosthodontic department in a dental institute in India. Eur J Prosthodont Restor Dent. 2009;17:85–9. [PubMed] [Google Scholar]
- 5.Arora M, Schwarz E, Sivaneswaran S, Banks E. Cigarette smoking and tooth loss in a cohort of older Australians: The 45 and up study. J Am Dent Assoc. 2010;141:1242–9. doi: 10.14219/jada.archive.2010.0052. [DOI] [PubMed] [Google Scholar]
- 6.Pihlgren K, Forsberg H, Sjödin L, Lundgren P, Wänman A. Changes in tooth mortality between 1990 and 2002 among adults in Västerbotten County, Sweden: Influence of socioeconomic factors, general health, smoking, and dental care habits on tooth mortality. Swed Dent J. 2011;35:77–88. [PubMed] [Google Scholar]
- 7.Mundt T, Schwahn C, Mack F, Polzer I, Samietz S, Kocher T, et al. Risk indicators for missing teeth in working-age Pomeranians – an evaluation of high-risk populations. J Public Health Dent. 2007;67:243–9. doi: 10.1111/j.1752-7325.2007.00041.x. [DOI] [PubMed] [Google Scholar]
- 8.Chatrchaiwiwatana S. Factors affecting tooth loss among rural Khon Kaen adults: Analysis of two data sets. Public Health. 2007;121:106–12. doi: 10.1016/j.puhe.2006.06.010. [DOI] [PubMed] [Google Scholar]
- 9.Walter MH, Wolf BH, Rieger C, Boening KW. Prosthetic treatment need in a representative German sample. J Oral Rehabil. 2001;28:708–16. doi: 10.1046/j.1365-2842.2001.00773.x. [DOI] [PubMed] [Google Scholar]
- 10.Sanders AE, Spencer AJ. Social inequality in perceived oral health among adults in Australia. Aust N Z J Public Health. 2004;28:159–66. doi: 10.1111/j.1467-842x.2004.tb00930.x. [DOI] [PubMed] [Google Scholar]
- 11.Rehan N, Chaudhary I, Shah SK. Socio-sexual behaviour of hijras of Lahore. J Pak Med Assoc. 2009;59:380–4. [PubMed] [Google Scholar]
- 12.Nanda S. 2nd ed. Belmont, CA: Wadsworth Publishing; 1999. Neither Man Nor Woman: The Hijra of India; p. 196. [Google Scholar]
- 13.Eunuchs of India – Deprived of Human Rights. [Last cited on 2011 Sep 22]. Available from: http://www.humanrightsdefence.org/eunuchs-of-indiadeprived-of-human-rights.html .
- 14.STROBE-Strengthening the reporting of observational studies in epidemiology. [Last cited on 2013 Mar 13]. Available from: http://www.strobe-statement.org/?id=available-checklists .
- 15.World Health Organization. 4th ed. Ch. 5. New Delhi, India: AITBS Publishers and Distributors; 1997. Oral Health Survey, Basic Methods; pp. 47–51. [Google Scholar]
- 16.Heckathorn DD. Respondent-driven sampling: A new approach to the study of hidden populations. Soc Probl. 1997;44:174–99. [Google Scholar]
- 17.Goodman LA. Snowball sampling. Ann Math Stat. 1961;32:148–70. [Google Scholar]
- 18.Bhardwaj VK, Veeresha KL, Sharma KR. Impact of socioeconomic status on decayed, missing, filled teeth (DMFT) among state government employees in Shimla City, Himachal Pradesh. Journal of Cranio Maxillary Dis. 2012;1:74–8. [Google Scholar]
- 19.Kida IA, Astrøm AN, Strand GV, Masalu JR. Clinical and socio-behavioral correlates of tooth loss: A study of older adults in Tanzania. BMC Oral Health. 2006;6:5. doi: 10.1186/1472-6831-6-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kapp JM, Boren SA, Yun S, LeMaster J. Diabetes and tooth loss in a national sample of dentate adults reporting annual dental visits. Prev Chronic Dis. 2007;4:A59. [PMC free article] [PubMed] [Google Scholar]
- 21.Mersel A, Anaise JZ, Shem-Tov A. Prosthetic needs and demands for services of a group of elderly people in Israel. Community Dent Oral Epidemiol. 1984;12:315–8. doi: 10.1111/j.1600-0528.1984.tb01462.x. [DOI] [PubMed] [Google Scholar]
- 22.Shroff BC. Edentulousness in India. National workshop on “Oral health goal”. Ind Dent Assoc. 1984;23:17–20. [Google Scholar]
- 23.Shah N, Parkash H, Sunderam KR. Edentulousness, denture wear and denture needs of Indian elderly – a community-based study. J Oral Rehabil. 2004;31:467–76. doi: 10.1111/j.1365-2842.2004.01260.x. [DOI] [PubMed] [Google Scholar]
- 24.Shenoy RP, Hegde V. Dental prosthetic status and prosthetic need of the institutionalized elderly living in geriatric homes in mangalore: A pilot study. ISRN Dent 2011. 2011:987126. doi: 10.5402/2011/987126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cunha-Cruz J, Nadanovsky P, Faerstein E, Lopes CS. Routine dental visits are associated with tooth retention in Brazilian adults: The Pró-Saúde study. J Public Health Dent. 2004;64:216–22. doi: 10.1111/j.1752-7325.2004.tb02756.x. [DOI] [PubMed] [Google Scholar]
- 26.Gerritsen AE, Allen PF, Witter DJ, Bronkhorst EM, Creugers NH. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual Life Outcomes. 2010;8:126. doi: 10.1186/1477-7525-8-126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Turrell G, Sanders AE, Slade GD, Spencer AJ, Marcenes W. The independent contribution of neighborhood disadvantage and individual-level socioeconomic position to self-reported oral health: A multilevel analysis. Community Dent Oral Epidemiol. 2007;35:195–206. doi: 10.1111/j.1600-0528.2006.00311.x. [DOI] [PubMed] [Google Scholar]