

Sir,
Brain metastases account for over 50% of the brain tumors, lung being the most common source. Location of the metastases in the brain depend upon the blood supply, the region that is richly perfused also bears the brunt of higher incidence of metastases; metastasis to the pineal region is rather rare. In fact, metastasis to the pineal region has been estimated to account for only 0.4% of all intracranial metastatic tumors.[1] A review of the literature revealed that the most common site of primary origin of a pineal metastasis is the lung and histologically, small cell lung carcinoma is the most frequent type of cancer. Most cases of pineal metastases are asymptomatic, and are diagnosed during autopsy. Therefore, the clinical characteristics of, and therapeutic approach for, metastatic pineal region tumors have not been well discussed in the literature. Herein, we present a rare case of lung adenocarcinoma presenting with Parinaud's syndrome as the first manifestation secondary to Pineal metastasis, along with the clinical features of this unusual lesion from the view point of differential diagnosis and therapeutic approach.
A 68-year-old female presented to us with chief complaints of headache and vomiting from last 1 month. Headache was generalized, more severe in morning and was associated with vomiting. On examination, patient was thin built, conscious, oriented, and her vitals were normal. Her higher mental functions were normal. She had near light dissociation, restricted upgaze, and convergence retraction nystagmus. Fundus examination revealed bilateral papilledema. Rest of cranial nerve examination and neurological examination was normal. Computed tomography (CT) brain was done which showed a contrast enhancing mixed density lesion in the posterior third ventricle with gross hydrocephalus suggestive of pineal region tumor [Figure 1]. Magnetic resonance imaging (MRI) brain with Gadolinium confirmed the location and the lesion [Figures 2 and 3]. Since the patient had signs of raised intracranial pressure (ICP) due to hydrocephalus, ventriculoperitoneal (VP) shunt was done and cerebrospinal fluid (CSF) subjected to examination. CSF did not reveal any malignant cell and all the tumor markers were undetectable Alpha-Fetoprotein (AFP; human chorionic gonadotropin, (HCG) and placental/germ cell alkaline phosphatase, PLAP). Chest X-ray revealed a suspicious lesion in right upper lobe for which CT scan of thorax was done. It showed a well-defined solid lesion in right upper lobe suggestive of a lung carcinoma [Figure 4]. Considering the age and built of the patient a CT-guided biopsy from the lung lesion was done; biopsy was suggestive of adenocarcinoma. The patient was referred to Radio-oncology unit for further treatment.
Figure 1.
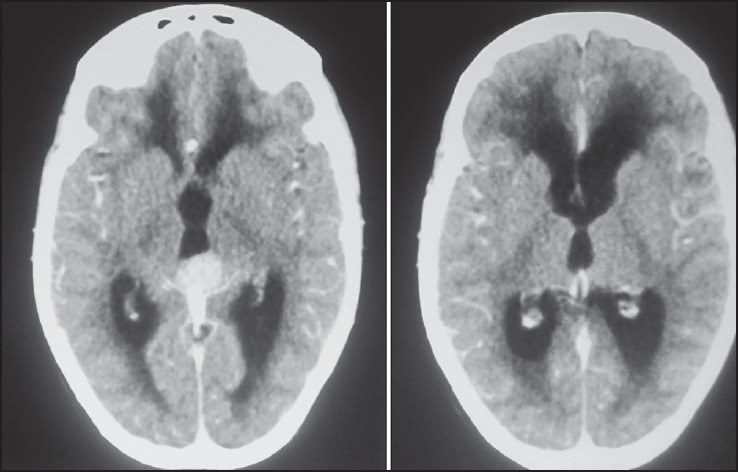
CT brain with contrast axial film showing pineal tumor which is enhancing brightly with hydrocephalus with signifiant periventricular ooze
Figure 2.
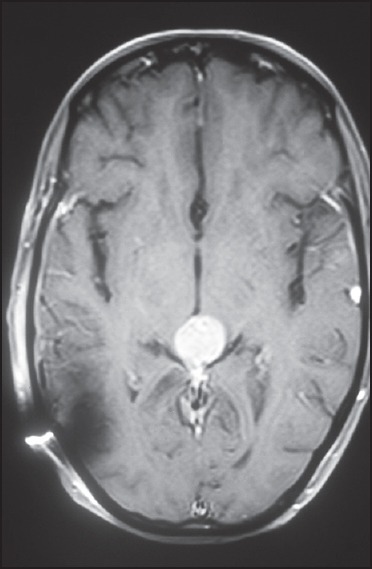
MRI brain with contrast, axial film showing well enhancing tumor in pineal region
Figure 3.
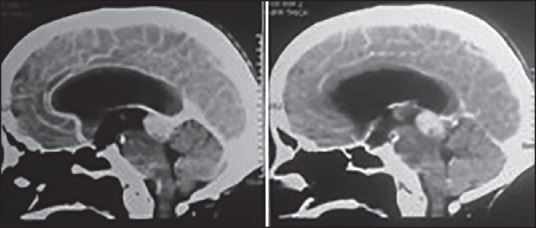
CT brain with contrast saggital view showing pineal metastatic lesion
Figure 4.
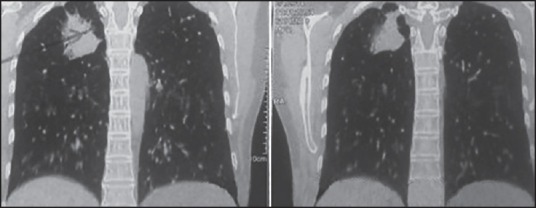
HRCT chest showing right sided lung malignancy
Although the brain is a common site of metastasis from lung cancer, it is rare to encounter patients presenting with symptoms attributable to an isolated metastatic pineal region tumor even before the diagnosis of the primary lung cancer. Pineal metastases used to be identified on autopsy as majority of them remained asymptomatic or were masked by the features of either a primary or by associated brain metastases.[1,2] Since the advent and widespread use of MRI Brain, more number of asymptomatic pineal region metastases has been reported. The most frequently reported histological type of lung cancer metastasizing to the pineal region is small cell carcinoma, in this case report the patient had adenocarcinoma; the metastasis of this histological type to the pineal region is rare.[1] The solitary metastasis to the pineal region poses a diagnostic dilemma, whether it is a solitary metastases or a pineal tumor itself. Most patients with primary pineal tumors are reported to be younger than 30 years old, and metastasis should be considered in older patients. In patients with a known history of malignancy, approximately 90% of all supratentorial lesions represent metastases.[2]
The prognosis of pineal region metastasis is extremely poor, and most such metastases are diagnosed by autopsy. Therefore, it is important to obtain improvement of the symptoms caused by pineal lesion tumors and confirm the histological diagnosis as soon as possible. Options include Tumor debulking in stable patients, Endoscopic biopsy and CSF diversion, or VP shunt with biopsy of primary in medically frail patients. Debulking of the pineal tumor is not without risks and cannot be justified if life expectancy of the patient is less than 6 months surgical interventions, including ventricular drainage, Endoscopy and ventriculoperitoneal shunting are useful for alleviating symptoms due to hydrocephalus. Endoscopy offers additional benefit that a biopsy can be taken simultaneously. But it requires an expertise, has a significant failure rate, can take significant amount of time and is not readily available at many centers. In such scenario, VP shunt offers an effective mean of initial treatment and CSF examination. Serum markers can further aid in diagnosing a primary pineal tumor. In addition a biopsy from accessible lesion in the lung can confirm the diagnosis without subjecting the patient to a major surgical intervention.
The pineal region is an uncommon site for intracranial metastasis, and metastasis to the pineal region without other brain metastases is rare. Any lesion in the pineal gland merits work up for metastases.
References
- 1.Nemoto K, Aoshiba K, Itoh M, Semba S, Tsuji T, Adachi H, et al. Isolated pineal region metastasis from lung adenocarcinoma with obstructive hydrocephalus: A case report. J Med Case Rep. 2013;7:71. doi: 10.1186/1752-1947-7-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Voorhies RM, Sunaresan N, Thaler HT. The single supratentorial lesion. An evaluation of preoperative diagnostic tests. J Neurosurg. 1980;53:364–8. doi: 10.3171/jns.1980.53.3.0364. [DOI] [PubMed] [Google Scholar]