

CONSULTATIONS are the cornerstone of veterinary practice, and while the length scheduled for consultations varies, 10 minute appointments are a frequent feature in first opinion practice. Previous research has suggested that consultations are complex (Robinson and others 2014) and often exceed 10 minutes in length (Shaw and others 2008, Everitt and others 2013), raising concerns as to whether a 10 minute appointment is sufficient to address all health concerns. In medicine, consultation length is positively correlated with the number of problems discussed (Flocke and others 2001) and longer consultations are associated with improved detection and management of certain conditions (Freeman and others 2002). It is unclear whether the same is true in veterinary medicine. The aim of this study was to determine the average consultation length in a sample of small animal consultations and to describe factors that may affect consultation length.
Data collection took place over two weeks in two practices (one week at each) operating 10 minute appointment systems, as part of data gathered for a larger project (Robinson and others 2014). Consultation length was recorded using a stopwatch during direct observation of small animal consultations. Timing started when the client entered the consultation room and stopped as they left. The time spent out of the room by the veterinary surgeon was included provided the client remained in the room. Time spent reading or writing clinical notes prior to or following the consultation, talking to the client in the waiting room, or preparing medications or samples once the client had left was not included (Everitt and others 2013). A previously developed data collection tool (Robinson and others 2014) was utilised to record the number of animals presented, number of problems discussed and the consultation type (preventive medicine or specific health problem). Descriptive statistics (median and interquartile range (IQR)) were carried out using IBM SPSS V.21. The Mann-Whitney U test was used to compare binary and numerical (non-parametric) variables, such as comparing consultation length between consultation types. A Spearman's rank correlation coefficient was used to compare number of problems discussed and consultation length, with a 95% CI calculated manually (Petrie and Watson 2006). Statistical significance was set at P=0.05. Ethical approval was obtained from the ethics committee at the School of Veterinary Medicine and Science, The University of Nottingham.
Data were recorded for 182 consultations involving 203 animals. These consisted of 55 consultations conducted by three veterinary surgeons in practice 1 and 127 consultations conducted by six veterinary surgeons in practice 2. Consultation length ranged from 51 seconds to 36 minutes 45 seconds with a median of 9 minutes 49 seconds (IQR 7 minutes 16 seconds–13 minutes 48 seconds). Length exceeded the 10 minutes allocated in 48.4 per cent of consultations (n=88). Consultations involving one animal (n=166) had a median length of 9 minutes 34 seconds (IQR 7 minutes 8 seconds–13 minutes 19 seconds) and 45.8 per cent (n=76) exceeded 10 minutes. Consultations involving multiple animals (n=16; two to five animals per consultation) had a median length of 14 minutes 39 seconds (IQR 10 minutes 3 seconds–19 minutes 40 seconds) and 75.0 per cent (n=12) exceeded 10 minutes. Consultations involving multiple animals were significantly longer than those involving one animal (P=0.001). Consultation length appeared to gradually increase as number of problems discussed increased (Fig 1), with weak positive correlation seen (Spearman's ρ: 0.373 (95% CI 0.240 to 0.491); P<0.001). Removing outliers made little difference to the correlation coefficient (Spearman's ρ: 0.376; P<0.001). Of the 43 consultations involving discussion of one problem only, 34.9 per cent (n=15) exceeded 10 minutes. Preventive medicine consultations (n=75) had a median length of 9 minutes 35 seconds (IQR 7 minutes 50 seconds–14 minutes 0 seconds) and 48.0 per cent (n=36) exceeded 10 minutes. Consultations for a specific health problem (n=107) had a median length of 9 minutes 56 seconds (IQR 7 minutes 9 seconds –13 minutes 42 seconds) and 48.6 per cent (n=52) exceeded 10 minutes. There was no significant difference in consultation length between these two types of consultation (P=0.709).
FIG 1:
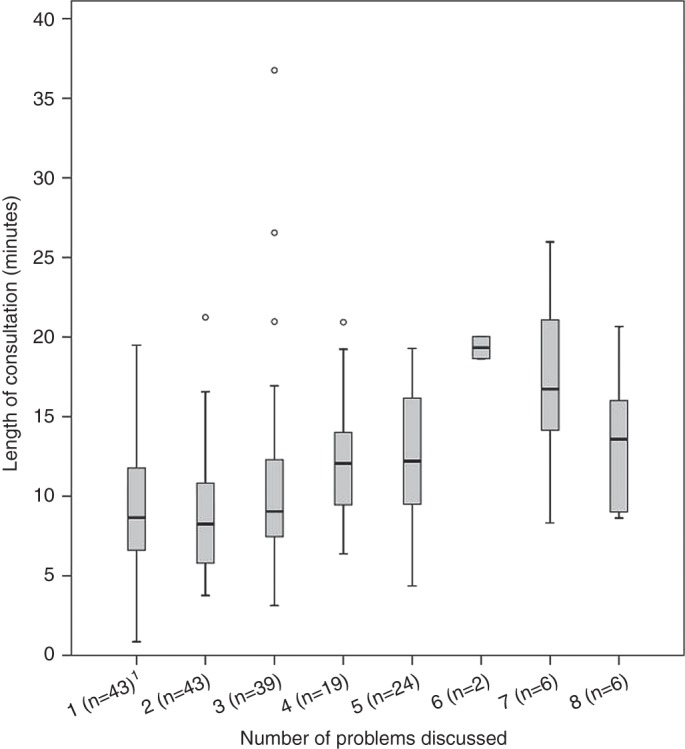
Box and whisker plots comparing consultation length (minutes) and number of problems discussed (n=182 consultations). Medians (central horizontal line), interquartile ranges (extent of the box) and ranges (whiskers) are shown. Outliers are shown as separate data points. 1Number of consultations timed is shown in brackets next to each problem number
Median consultation length was shorter than in previous studies (Shaw and others 2008, Everitt and others 2013) however many still exceeded the time allocated. This suggests that a 10-minute consultation may not be of sufficient length, particularly as not all tasks associated with a consultation were included in the timing.
The weak but positive correlation between consultation length and problem number mirrors findings in medicine (Flocke and others 2001). Limiting consultations to one problem has been attempted in medicine but there is disagreement as to whether this is good practice or not (Fullerton 2008). As many consultations involving one problem still exceeded the time allocated, allowing only one problem to be discussed may be ineffectual at limiting veterinary consultation length. Consultations for a specific health problem were not longer than those for preventive medicine, which is consistent with previous findings (Shaw and others 2008, Everitt and others 2013). However multiple animals may be more likely to be presented in preventive medicine consultations, making a simple comparison between consultation types difficult. The complexities of preventive medicine consultations shall be considered in a separate paper.
Further work could describe other factors in relation to consultation length; Everitt and others (2013) found that first consultations tended to be longer than revisits. If consultation length can be predicted based on minimal information, tailored appointments could supersede standard appointments. Alternatively, 15-minute or 20-minute appointments could be trialled. Monitoring the effects of this could help to determine whether consultation length is associated with improved patient care, owner satisfaction and financial benefits for the practice. Further involvement of veterinary nurses in consultations is another potential solution. In the USA, veterinary technicians' skills in client education, history-taking and clinical examination are already being utilised to provide a longer, more thorough consultation (Tracey 2011).
The small convenience sample is a limitation of this study, and it is unclear whether this sample is representative of first opinion practice in the UK. Recruiting more practices, including those operating different appointment systems, may shed further light on the factors associated with consultation length. Timing at the consultation level, rather than individual patient level, is a further limitation; accounting for this could allow the effect of patient characteristics, for example species and age, to be considered.
Acknowledgments
The authors thank the sentinel practices, their clients and patients for their involvement in the study. This study was supported by an unrestricted grant from Novartis Animal Health and The University of Nottingham.
References
- Everitt S., Pilnick A., Waring J., Cobb M. (2013) The structure of the small animal consultation. Journal of Small Animal Practice 54, 453–458 [DOI] [PubMed] [Google Scholar]
- Flocke S. A., Frank S. H., Wenger D. A. (2001) Addressing multiple problems in the family practice office visit. The Journal of Family Practice 50, 211–216 [PubMed] [Google Scholar]
- Freeman G. K., Horder J. P., Howie J. G., Hungin A. P., Hill A. P., Shah N. C., Wilson A. (2002) Evolving general practice consultation in Britain: issues of length and context. BMJ, 324, 880–882 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fullerton M. (2008) Understanding and improving on 1 problem per visit. Canadian Medical Association Journal 179(7), 623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petrie A., Watson P. (2006) Linear correlation and regression. In Statistics for Veterinary and Animal Science. 2nd edn. Oxford: Blackwell. pp 121–140 [Google Scholar]
- Robinson N. J., Brennan M.L., Cobb M., Dean R. S. (2014) Capturing the complexity of first opinion small animal consultations using direct observation. Veterinary Record. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaw J. R., Adams C. L., Bonnett B. N., Larson S., Roter D. L. (2008) Veterinarian-client-patient communication during wellness appointments versus appointments related to a health problem in companion animal practice. Javma-Journal of the American Veterinary Medical Association 233, 1576–1586 [DOI] [PubMed] [Google Scholar]
- Tracey S. (2011) 9 steps to a perfect veterinary appointment. Veterinary Economics (online article). http://veterinarybusiness.dvm360.com/vetec/Veterinary+business/9-steps-to-a-perfect-veterinary-appointment/ArticleStandard/Article/detail/710159. Accessed July 14 2014 [Google Scholar]