

Abstract
The left internal mammary artery is the preferred graft for treating left anterior descending coronary artery disease. Dissection is a rare but grave sequela of internal mammary artery graft angiography. The available medical literature is scant, perhaps as a result of under-reporting.
We report a case in which dissection of the internal mammary artery graft occurred during diagnostic angiography, and we discuss its management. In addition, we review the available literature and provide a retrospective analysis of the data from our own catheterization laboratory. In our single-center analysis of 542 cases of selective internal mammary artery graft angiography, we found only the single case of internal mammary artery graft dissection (0.2%) that we report here. Our review of the literature revealed 7 reported cases of internal mammary artery graft dissection, 3 of which were iatrogenic. There were no identifiable risk factors for such dissection. After treatment with angioplasty and stenting, all patients had good outcomes during follow-up.
Keywords: Aneurysm, dissecting/therapy; angioplasty, balloon, coronary; coronary artery bypass; internal mammary artery-coronary artery anastomosis/adverse effects; mammary arteries/dissection/injuries/surgery; postoperative complications; dissection; stents; treatment
Internal mammary artery (IMA) bypass grafts have proved superior to saphenous venous grafts in long-term patency.1–3 One of the dread sequelae of IMA angiography is dissection. We report a case of left IMA graft dissection and we review the medical literature. In addition, we perform a retrospective analysis of IMA graft angiographies and sequelae from our local Veterans Affairs catheterization database.
Case Report
A 58-year-old man presented with worsening angina and dyspnea of 2 weeks' duration. He had a history of 4-vessel coronary artery bypass grafting (in 1995), diabetes mellitus, stage 4 chronic kidney disease, and congestive heart failure with a left ventricular ejection fraction of 0.40 to 0.45.
Selective graft angiography with use of an IMA catheter revealed a graft to a ramus intermedius. At this point, we detected a proximal filling defect that suggested a dissection (Fig. 1). We deferred percutaneous intervention because of the patient's impaired renal function and because his non-flow-limiting lesion was asymptomatic. After 48 hours, we undertook elective intervention on this IMA graft. Using a Judkins right-5 curve guide catheter, we carefully introduced a Balance Middleweight™ guidewire (Abbott Vascular, part of Abbott Laboratories; Redwood City, Calif) into the true lumen of the left IMA. Unfortunately, the inflation (to 12 atm) of a 2 × 15-mm Apex® Flex balloon (Boston Scientific Corporation; Natick, Mass) in the proximal left IMA led to a spiral dissection (Fig. 2). We then decided to treat the entire length of the dissection with balloon angioplasty and stenting, using 4 Taxus® Liberté™ stents (Boston Scientific), distal to proximal as follows: 1 stent, 2.25 × 16-mm; 1 stent, 2.25 × 24-mm; and 2 stents, 2.25 × 20-mm each (Fig. 3). The patient was discharged from the hospital 48 hours later. His cardiac biomarkers and renal function remained stable during follow-up.
Fig. 1.
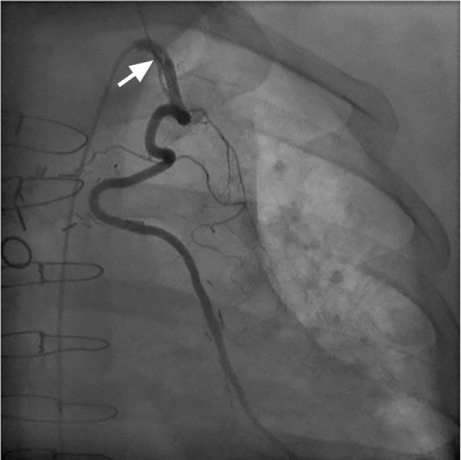
Selective angiography with use of an internal mammary artery catheter shows a filling defect (arrow) in the left IMA graft, consistent with dissection.
Fig. 2.
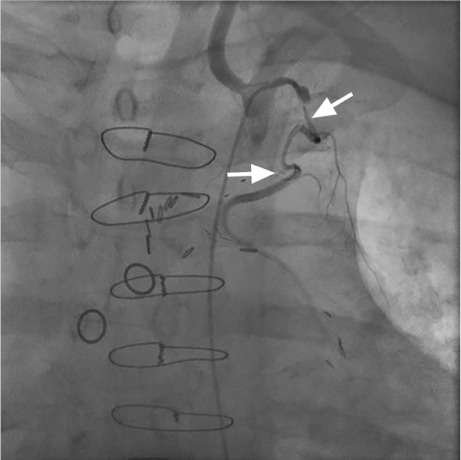
Selective angiography with use of an internal mammary artery catheter shows spiral dissection of the left IMA (arrows).
Fig. 3.

Nonselective angiography with use of an internal mammary artery catheter shows the left IMA after stent deployment.
Methods and Literature Review
Our institutional review board approved a single-center, retrospective database review of patients who had undergone IMA graft angiography in order to investigate stable angina, acute coronary syndrome, and a positive functional study. Included in the analysis were 542 patients who had undergone graft angiography from January 2003 through December 2012. Because our intent was only to determine the incidence of this problem, and because we expected a very low number, we chose not to undertake any further statistical analysis.
In addition, we performed a thorough search of PubMed®, Embase™, Web of Science™, and Scopus® to identify any case reports or studies on IMA dissection that bore the following combination of terms: (Internal Mammary Artery OR Left Internal Mammary Artery) AND (Angiography) AND (Dissection) AND (Humans).
Results
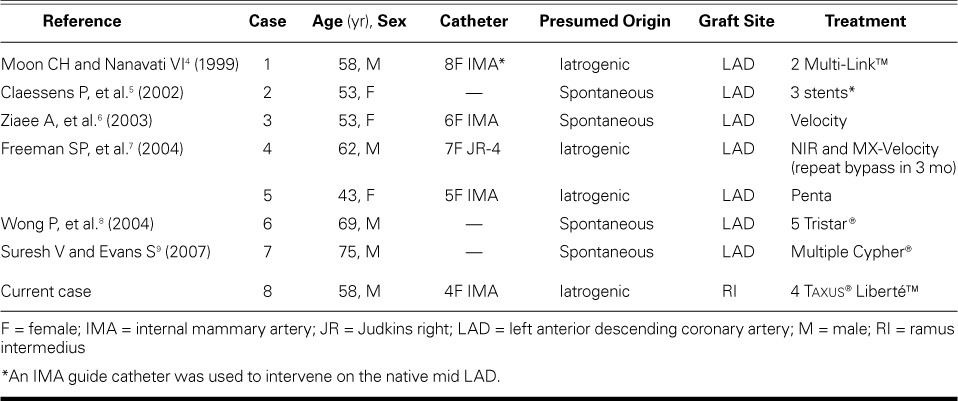
Our database review of 542 IMA angiograms revealed only one case of catheter-related IMA dissection (Table I). The literature review identified 7 cases of IMA dissection, all of which had been treated with angioplasty and stenting; only 1 patient had undergone repeat bypass surgery. Follow-up after stenting was variable and was not reported uniformly (Table II4–9).
TABLE I.
Summary of Internal Mammary Artery Catheterizations and Sequelae: Single-Center Review
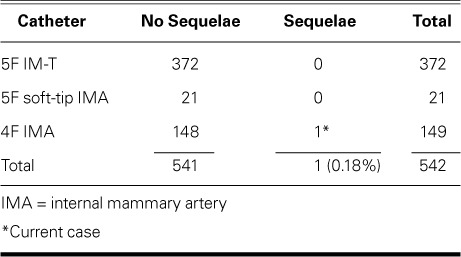
TABLE II.
Literature Review of Spontaneous/Iatrogenic Left Internal Mammary Artery Dissection and Treatment
Discussion
Our single-center retrospective study found a very low incidence of IMA dissection during routine IMA graft angiography. On the basis of our review of the medical literature, we conclude that percutaneous angioplasty and stenting can be a feasible and safe option in the treatment of IMA graft dissection.
The left IMA has become the conduit of choice for bypass of the left anterior descending coronary artery. The vessel has superior patency rates (up to 12 years2), in comparison with saphenous vein grafts. Some operators have advocated the preoperative evaluation of the left IMA to judge not only the patency but the distal caliber of the vessel for anastomosis.3,9 Not uncommonly, the IMA is a challenging vessel through which to pass a catheter, because of its 1) acute angle of origin from the left subclavian artery, 2) long and tortuous course in the anterior mediastinum, and 3) comparatively small lumen.4 Moreover, the IMA can be compromised by dissection of the subclavian artery during catheter manipulation. Catheter-induced dissection of the left IMA, first described in 1985,10 carries the potential for catastrophic consequences. Concern for ostial IMA damage led Kuntz and Baim11 to propose a standard cannulation technique for the IMA. They recommended the use of an IMA catheter, rather than the diagnostic Judkins right catheter, and the use of tapered, soft-tipped catheters. They also proposed, as a safer technique, nonselective angiography of the IMA via injection of the proximal subclavian artery—especially when the IMA has anomalous origin. Although injection of the proximal subclavian artery rarely provides adequate opacification of the IMA, a scout arteriogram of the left subclavian artery before selective cannulation of the IMA graft can guide the operator to an easier and safer selective engagement.
Percutaneous transluminal coronary angioplasty and stenting are standard therapies for acute coronary artery dissection. Gruberg and colleagues12 have evaluated the outcomes after percutaneous revascularization of IMA grafts and have shown that lesions treated with stents were usually ostial, whereas lesions treated with angioplasty alone tended to be located at the distal anastomosis. The authors suggest that stenting might be the best approach to treating distal lesions as well.
Footnotes
From: Section of Cardiovascular Medicine, Department of Internal Medicine, University of Oklahoma Health Sciences Center & Veterans Affairs Medical Center, Oklahoma City, Oklahoma 73104
References
- 1.Barner HB, Standeven JW, Reese J. Twelve-year experience with internal mammary artery for coronary artery bypass. J Thorac Cardiovasc Surg. 1985;90(5):668–75. [PubMed] [Google Scholar]
- 2.Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med. 1986;314(1):1–6. doi: 10.1056/NEJM198601023140101. [DOI] [PubMed] [Google Scholar]
- 3.Bourassa MG, Fisher LD, Campeau L, Gillespie MJ, McConney M, Lesperance J. Long-term fate of bypass grafts: the Coronary Artery Surgery Study (CASS) and Montreal Heart Institute experiences. Circulation. 1985;72(6 Pt 2):V71–8. [PubMed] [Google Scholar]
- 4.Moon CH, Nanavati VI. Multi-stent approach in the treatment of acute dissection of the left internal mammary artery. J Invasive Cardiol. 1999;11(4):248–50. [PubMed] [Google Scholar]
- 5.Claessens P, Willaert W, Claessens M, Bloemen H, Coosemans M, van Eeuwijk J, Vanderheyden M. Symptomatic atraumatic dissection of a left internal mammary artery graft five years after coronary artery bypass graft surgery. Can J Cardiol. 2002;18(7):759–61. [PubMed] [Google Scholar]
- 6.Ziaee A, Puri S, Kern MJ. Stenting for spontaneous left internal mammary artery dissection: a case report. Catheter Cardiovasc Interv. 2003;60(3):389–91. doi: 10.1002/ccd.10666. [DOI] [PubMed] [Google Scholar]
- 7.Freeman SP, Liston MJ, Lips DL, Vacek JL. Catheter-induced left internal mammary artery dissection: a report of two cases and review of the literature. J Interv Cardiol. 2004;17(2):117–21. doi: 10.1111/j.1540-8183.2004.00255.x. [DOI] [PubMed] [Google Scholar]
- 8.Wong P, Rubenstein M, Inglessis I, Pomerantzev E, Ferrell M, Leinbach R. Spontaneous spiral dissection of a LIMA-LAD bypass graft: a case report. J Interv Cardiol. 2004;17(4):211–3. doi: 10.1111/j.1540-8183.2004.02085.x. [DOI] [PubMed] [Google Scholar]
- 9.Suresh V, Evans S. Successful stenting of stenotic lesion and spontaneous dissection of left internal mammary artery graft. Heart. 2007;93(1):44. doi: 10.1136/hrt.2006.087551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Farooqi S, Jain AC, O'Keefe M. Catheter-induced left internal mammary artery bypass graft dissection. Cathet Cardiovasc Diagn. 1985;11(6):597–601. doi: 10.1002/ccd.1810110608. [DOI] [PubMed] [Google Scholar]
- 11.Kuntz RE, Baim DS. Internal mammary angiography: a review of technical issues and newer methods. Cathet Cardiovasc Diagn. 1990;20(1):10–6. doi: 10.1002/ccd.1810200104. [DOI] [PubMed] [Google Scholar]
- 12.Gruberg L, Dangas G, Mehran R, Hong MK, Waksman R, Mintz GS et al. Percutaneous revascularization of the internal mammary artery graft: short- and long-term outcomes. J Am Coll Cardiol. 2000;35(4):944–8. doi: 10.1016/s0735-1097(99)00652-x. [DOI] [PubMed] [Google Scholar]