

Abstract
The AOCMF Classification Group developed a hierarchical three-level craniomaxillofacial classification system with increasing level of complexity and details. The highest level 1 system distinguish four major anatomical units including the mandible (code 91), midface (code 92), skull base (code 93), and cranial vault (code 94). This tutorial presents the level 2 system for the midface unit that concentrates on the location of the fractures within defined regions in the central (upper, intermediate, and lower) and lateral (zygoma, pterygoid) midface, as well as the internal orbit and palate. The level 2 midface fracture location outlines the topographic boundaries of the anatomical regions. The common nasoorbitoethmoidal and zygoma en bloc fracture patterns, as well as the time-honored Le Fort classification are taken into account. This tutorial is organized in a sequence of sections dealing with the description of the classification system with illustrations of the topographical cranial midface regions along with rules for fracture location and coding, a series of case examples with clinical imaging and a general discussion on the design of this classification. Individual fracture mapping in these regions regarding severity, fragmentation, displacement of the fragment or bone defect is addressed in a more detailed level 3 system in the subsequent articles.
Keywords: fracture classification, midface, anatomic regions
Fractures of the midface occur in a high variety of fracture patterns and are difficult to classify appropriately to assign standardized categories of fracture classes reflecting the injury status of the patient. Requirements for a fracture classification are its clinical relevance and the ability to provide reliable and reproducible means to communicate the degree of trauma to the observer. A hierarchical classification system offers high versatility for the development, the validation process, and conclusive documentation.1 The AOCMF fracture classification system is based on different precision levels. Level 1, an elementary system for fracture location, is appropriate for all trauma surgeons to describe the affection of the midface as one of the four main anatomical units of the facial skeleton: mandible (code 91), midface (code 92), skull base (code 93), and cranial vault (code 94).
Level 2, a basic system for refined fracture location, is appropriate for all craniomaxillofacial (CMF) specialties referring to the anatomical regions and subregions of the midface, whereas the level 3 system is designed for assessing fracture morphology. The present article refers to the level 2 classification system for fractures of the midface including the orbit and takes the time-honored Le Fort (LF) classification into account. It is organized in a sequence of sections dealing with the description of the classification system with illustrations of the topographical cranial midface regions along with rules for fracture location and coding, a series of case examples with clinical imaging and a general discussion on the design of this classification. Individual fracture mapping in these regions regarding severity, fragmentation, and bone defect is addressed in a more detailed level 3 system in the subsequent articles.2 3 Regions of the adjacent skull base and cranial vault units are presented separately.4
Level 2 Midface and Orbit Fracture Classification System
The level 2 focuses on the topographic location of fractures according to anatomical regions within the midface and internal orbit (Table 1). An overview of the detailed topography and structure of the midface and internal orbit are presented in Figs. 1 and 2. Fracture lines are documented according to the involvement of the left and right sides.
Table 1. Level 2 midface and internal orbit anatomical structure mapping.
| Level 1 | Level 2 | Internal | Le Fort fracture patterns | ||||
|---|---|---|---|---|---|---|---|
| Code | Regions | Codea | Level 2 subdivisions | Orbit | I | II | III |
| 92 | Midface | Z | Zygoma/zygomatic arch | × | |||
| U | UCM (nasal skeleton) | × | × | ||||
| I | ICM | × | × | ||||
| L | LCM (maxillary bodies) | × | × | × | |||
| Pt | Pterygoid process | × | × | × | |||
| P | Palate | ||||||
| Om | Orbital medial wall | × | |||||
| Ol | Orbital lateral wall | × | |||||
| Oi | Orbital inferior wall (floor) | × | |||||
| 93 | Skull base | Os | Orbital superior wall (roof)/anterior skull base | × | |||
| Oa | Orbital apex (cone)/sphenoid bone | × | |||||
Figure 1.
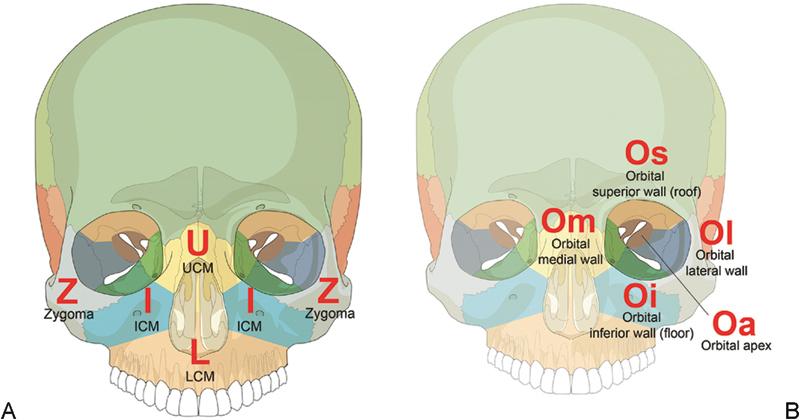
Midface (A) and orbit (B) mapping of anatomical subdivisions on the anterior skull. UCM, upper central midface–nasal skeleton including bone and nasofrontal maxilla; ICM, intermediate central midface–parapiriform maxilla and infraorbital maxilla; LCM, lower central midface–maxillary bodies including infrazygomatic maxilla; Z, zygoma/zygomatic arch.
Figure 2.
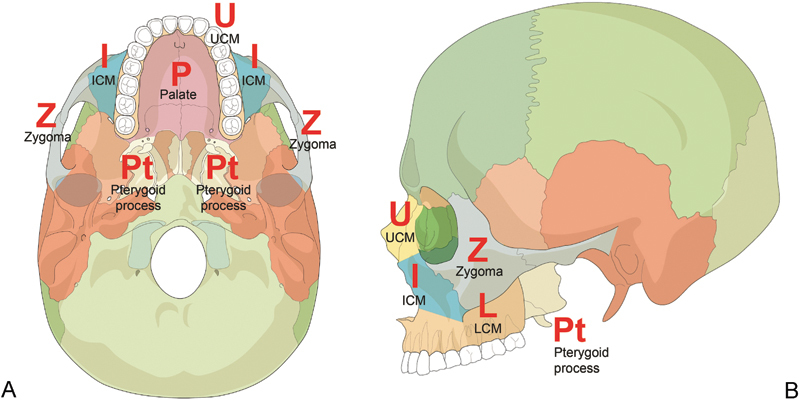
Midface mapping of anatomical subdivisions on the caudal (A) and lateral (B) skull. UCM, upper central midface–nasal skeleton including bone and nasofrontal maxilla; ICM, intermediate central midface–parapiriform maxilla and infraorbital maxilla; LCM, lower central midface–maxillary bodies including infrazygomatic maxilla; Z, zygoma/zygomatic arch.
Central Midface
The skeletal unit labeled as the midface consists of the maxillae, nasal skeleton, zygomas (including the complete arch), and the medial inferolateral circumference of the orbital rims. The midface can be distinguished into a central and lateral part in terms of vertical compartments. The precision level 2 defines the midface as the upper jaw. The facial skeleton above it ends superiorly at the level of both the frontozygomatic sutures laterally and the frontomaxillary or frontonasal sutures, medially.
The upper jaw consists of the two maxillary bodies enclosing the piriform aperture and reaching for contact with the anterior skull base via their frontal processes. The bony architecture resembles a pyramid shape and is labeled as the central midface.
The supraorbital rims and the orbital roofs make up the superior circumference of the orbit and belong to the frontal bone as part of the skull base.
The central midface (Fig. 1) is defined as a grid of three horizontal partitions stratified above each other:
UCM: Upper central midface (nasal skeleton: bone/nasofrontal maxilla).
ICM: Intermediate central midface (parapiriform maxilla/infraorbital maxilla).
LCM: Lower central midface (maxillary bodies).
Accordingly, the level 2 CMF classification may relate to the LF fracture levels (Table 1).
Upper Central Midface
The UCM consists of the upper extensions of the frontomaxillary processes that frame the anterior medial orbits and the two nasal bones. In essence, its boundaries match with the bony nasal skeleton. The horizontal intersection between the UCM and ICM is the continuation of a line drawn medially from the lower end of the lateral margin of the lacrimal fossa. This line runs anterior medially to the initial point of the nasomaxillary suture line. The nasal septum and the vomer are not considered in the level 2 classification system, but in the level 3 system.2
Intermediate Central Midface
The ICM is synonymous with the infraorbital portion of the maxilla encompassing the maxillary antrum and the middle nasal meatus. It extends from the piriform aperture to the zygomaticomaxillary suture. Superomedially the border is identical with the lower border of the UCM. The superior limit of the ICM is the infraorbital margin (rim). Superolaterally the ICM is bounded by the zygomaticomaxillary suture line (Figs. 1A and 2).
The lower horizontal demarcation of the ICM begins at the convergence of the maxillary buttress into the nasal cavity at the level of the most lateral margin from the pyriform aperture. From this point, it takes a course toward the foot of the zygomaticomaxillary crest and upper margin of the maxillary tuberosity (inferior orbital fissure and pterygomaxillary junction (Fig. 1A).
Lower Central Midface
The LCM is defined as the solid body of the maxilla plus the alveolar process, and includes the maxillary tuberosity area extending to the inferior orbital fissure and the sphenopalatine foramen. Superiorly, the horizontal limiting line is identical with the aforementioned lower horizontal demarcation line of the ICM, corresponding to the LF I level (Figs. 1A and 2).
The posterior aspect of the LCM comprises the entire maxillary tuberosity region to the inferior orbital fissure. The posterior border of the LCM extends to the pterygomaxillary fissure (Fig. 3).
Figure 3.
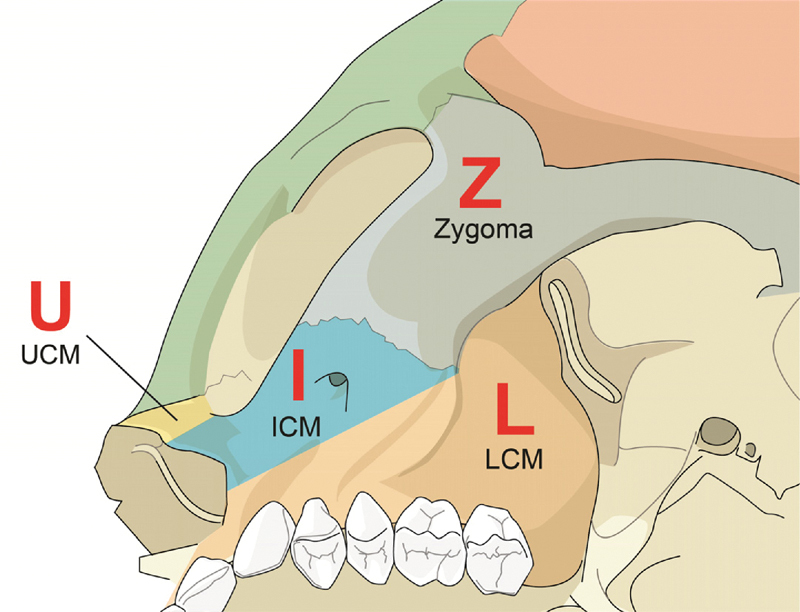
Lower central midface extension in the maxillary tuberosity region. UCM, upper central midface; ICM, intermediate central midface; LCM, lower central midface; Z, zygoma/zygomatic arch.
Zygoma/Zygomatic Arch
The zygoma and the zygomatic arch constitute the lateral midface (Fig. 2B). Both structures appear in combination in the scheme and their overall configuration can be clearly delineated by the anatomic suture lines. These bounding lines are used with two exceptions:
The posterior border of the zygomatic arch passes through the temporal bony base of the glenoid fossa. As a result, the full zygomatic arch length is added up to the schematic unit (Figs. 2 and 4).
The orbital surface of the zygoma (lateral orbital flange) is a constituent of the lateral internal orbit (or the anterior portion of the lateral orbital wall) and must be recorded as such.
Figure 4.
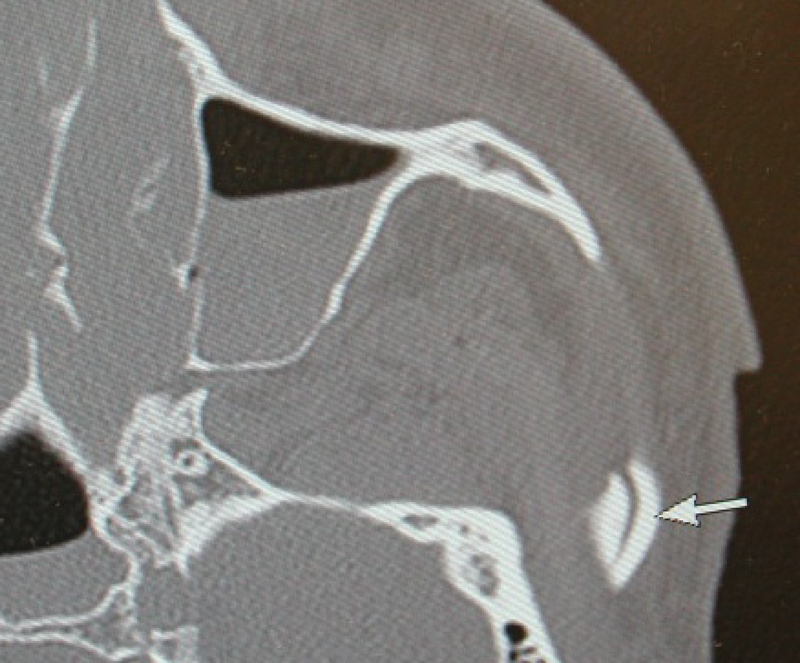
Fracture of the origin of the zygomatic arch. CT scan axial view showing a fracture of the origin of the zygomatic arch, passing through the temporal bony base of the glenoid fossa (arrow) that is added to the zygomatic region.
Note: The posterior thin portion of the lateral orbital wall is part of the greater wing of the sphenoid.
Pterygoid Process
Anatomically, the sphenoid is one of the most complex cranial bony structures and backs up the skull base and midface (Fig. 2). The pterygoid process (retrotuberic bone formation) and the orbital apex (dorsal internal orbit) are regarded independently as separate anatomical regions of the sphenoid bone.
For the sake of simplification, the remaining sphenoid bone partitions and the temporal bone have been combined into one large region in the scheme.4
The choanae, the vertical constituents of the palatine bone and the pterygoid plates are recognized as a single entity, ending upwards at the lower surface of the sphenoid body and interiorly with the pterygomaxillary fissure.
Palate
The palate is regarded as a special region and combines the palatine process of the maxilla and the horizontal plate of the palatine bone (Fig. 2).
Internal Orbit
The orbital walls are assessed independently from the bones that they originate from (geometric concept). In the anterior section of the orbital cavity and the so-called midorbit (middle section of the orbital cavity),3 the four walls make up a quadrangular-shaped coronal cross-section. In the three-dimensional view, this configuration is pyramidal in shape, the base of which is located over the anterior orbital entrance. To its posterior end the orbital floor blends into the medial wall resulting in the triangular-shaped coronal cross-section of the apex region.
The internal orbit is composed of four walls and the apex (Fig. 1B):
Orbital superior wall or roof (superior wall formed by the orbital surface of the frontal bone). In the level 2 scheme it is considered independently from the rest of the frontal bone.
Orbital lateral wall (formed by lateral flange of the zygoma and the thin part of the greater wing of the sphenoid around the suture).
Orbital medial wall (formed by the lacrimal and the ethmoid bone).
Orbital inferior wall or floor (inferior wall formed by the orbital surface of the maxilla).
The orbital apex represents the posterior section of the internal orbit and starts where the rectangular coronal cross-section becomes more triangular in shape. The transition into the cone usually begins behind the posterior end of the inferior orbital fissure. The orbital canal is included in the orbital cone.
The demarcation line between the orbital rims and the internal orbital walls is determined by the anterior opening of the orbital cavity. All structures around the orbit projecting to the external bony surface in a strictly frontal view are regarded as orbital rims. The internal orbit begins just behind these structures.
Fracture Patterns
The classification system allows specifying common fracture patterns in the midface including LF types I, II, and III, zygoma en bloc (ZEB) and nasoorbitoethmoidal (NOE). LF and ZEB patterns can be specified unilaterally or bilaterally. These patterns involve the following regions:
LF I: LCM and pterygoid process
LF II: LCM, pterygoid process, ICM, and UCM
LF III: LCM, pterygoid process, zygoma, lateral, inferior and medial orbital walls, and UCM
ZEB: Zygoma, lateral and inferior orbital walls
NOE: Medial orbital walls both sides, and UCM
While the NOE pattern is central, both LF and ZEB patterns can be specified separately on either or both sides. On any side the LF I, II, and III patterns are exclusive, that is, they cannot be combined. The NOE pattern can be combined with ZEB and/or LF I patterns. The ZEB pattern can be combined with LF II or LF I (with or without NOE) patterns.
Fracture Coding, Imaging, and Topographical Distribution
According to the general scheme of the AO/OTA classification system,5 CMF fractures are assigned with the one digit code 9; in this CMF scheme, fractures of the midface, skull base, and cranial vault are identified with the two digit codes 92, 93, and 94, respectively.1
In coding midface fractures according to their topography in the level 2 system, each region is identified by a letter as described in Table 1 and in the figures.
The letters specifying the involved regions are added after the initial two-digit code 92. The regions are coded in the order from the patient's right side to the patient's left side. In the overall fracture code, the small letter “m” (abbreviation for “middle”), or the letter “U” if the upper midface region is fractured, marks the limit between the two sides. Hence, letters specified before and after the “m” or “U” refer to the patient's right and left side, respectively. In the code, a point “.” is inserted in between region letters, which in this context does not indicate whether the fractures are confined or not within the involved regions, as opposed to the mandibular system.6
Fracture patterns are indicated in addition between brackets after this code using the letters LF, ZEB or NOE. Again the small letter “m” (abbreviation for “middle”), or the letters “NOE” if the NOE pattern is specified, marks the limit between the two sides. LF and ZEB patterns can be indicated both sides.
Case Examples
This coding system allows description of most relevant fracture patterns as illustrated in the case examples, such as LF fracture patterns as well as the differentiation between unilateral or bilateral fracture patterns. In a series of three case examples, we illustrate the coding of a fracture of the upper central midface (Fig. 5); a bilateral LF I (LCM), LF II (ICM), nasal bone fractures (UCM), and a zygoma fracture on the left side (Fig. 6); a zygoma fracture with lateral orbital wall involvement (Fig. 7); and a fracture of the origin of the zygomatic arch (Fig. 4). A range of additional fracture patterns are presented in a special case appendix7 as electronic supplement to this issue of the Journal at www.aocmf.org/classification.
Figure 5.
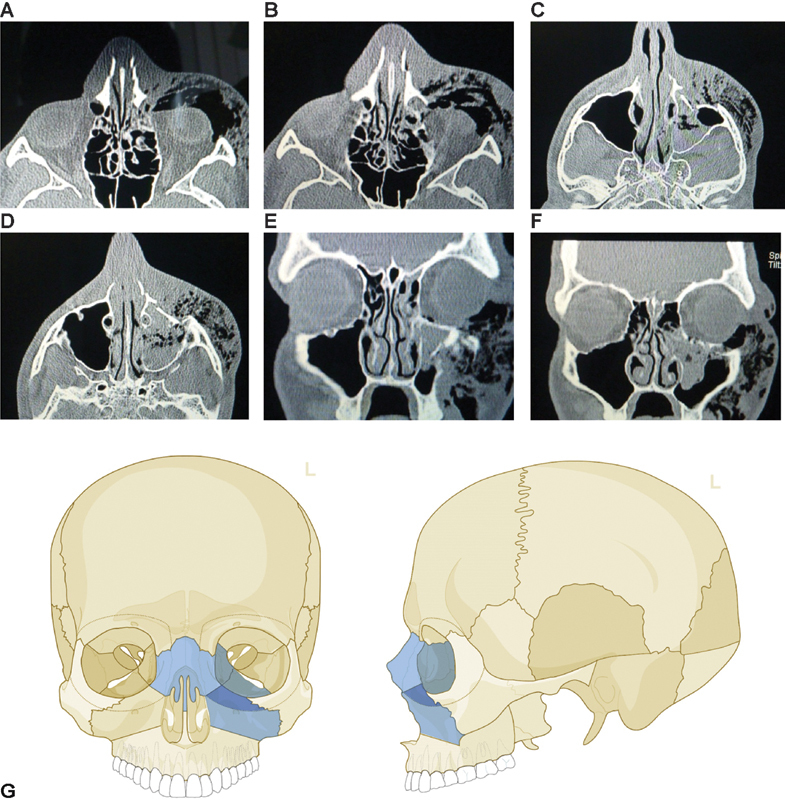
Fracture of the upper central midface. Imaging: CT scan axial view (A–D) and coronal view (E, F). Description: Nasoorbitoethmoidal (NOE) fracture with involvement of nasal bones bilaterally (UCM), medial orbital and inferior orbital rim left side (UCM and ICM), the anterior medial wall (Om) and the orbital floor (Oi) are fractured. (G) Level 2 Code: 92 U.Omi.Ii. This case example CMTR-92-001 is made available electronically for viewing using the AOCOIAC software at www.aocmf.org/classification.
Figure 6.
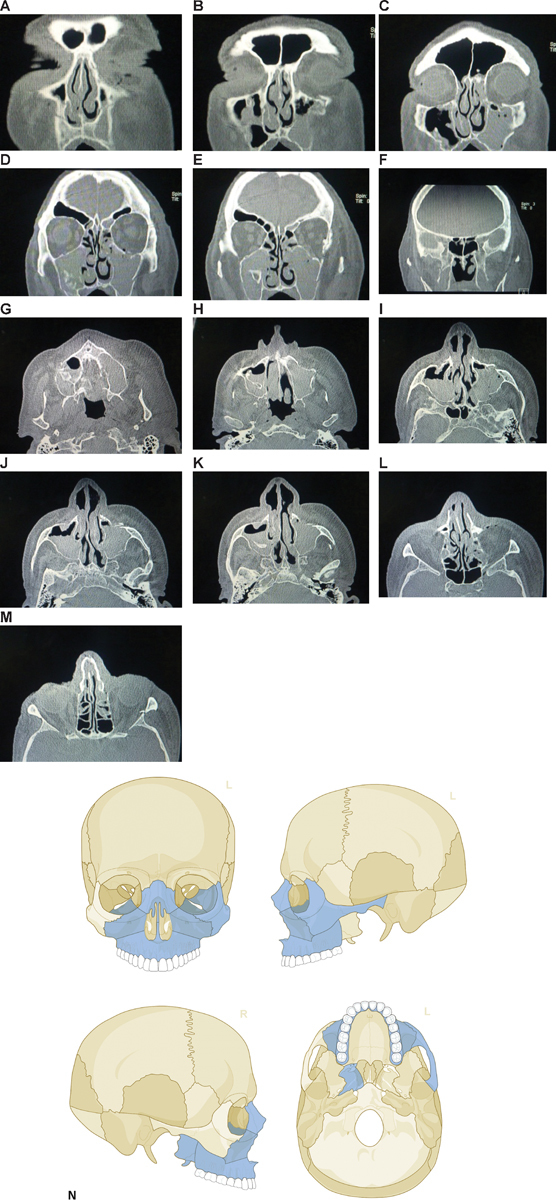
Bilateral Le Fort I fracture associated with nasal bones and zygoma fracture on the left side. Imaging: CT scan coronal view (A–F) and axial view (G–M). Description: Bilateral Le Fort I fracture (ICM and LCM) and nasal bones (UCM), with fracture of the right pterygoid bone (Pt) as well as a zygoma fracture on the left side (Z) bilateral orbital floor fracture (Om) and involvement of the left lateral orbital wall (Ol). There is no clearly visible fracture of the medial orbital wall fracture (Om is not coded).(N) Level 2 Code: 92 I.L.Pt.Oi.U.Oil.L.I.Z. This case example CMTR-92-002 is made available electronically for viewing using the AOCOIAC software at www.aocmf.org/classification.
Figure 7.
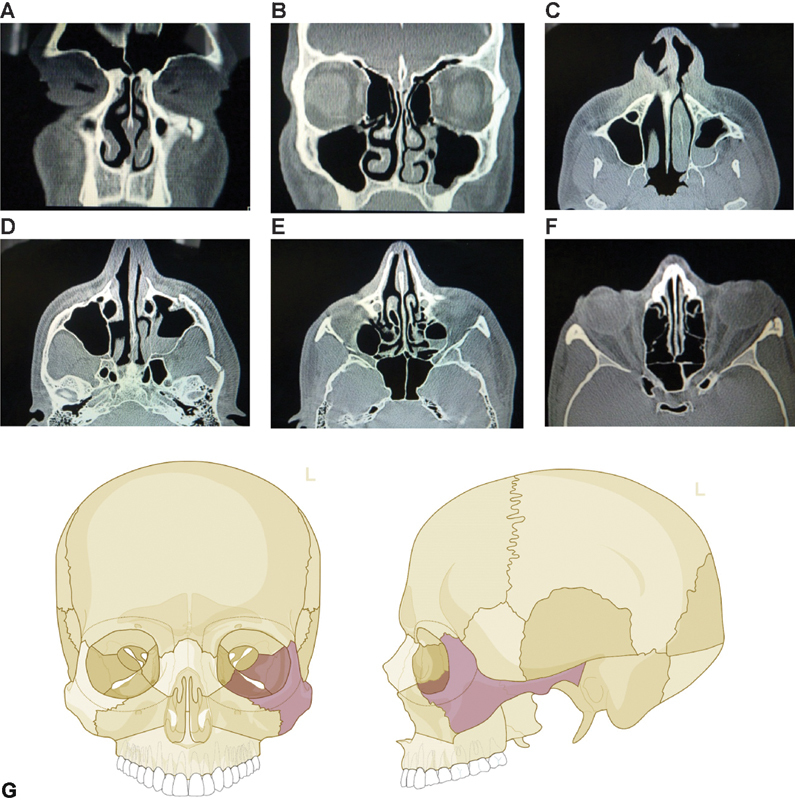
Zygoma fracture on the left side. Imaging: CT scan coronal view (A, B) and axial view (C–F). Description: En bloc zygoma fracture on the left side, fracture of the arch with intermediate fragment (Z); the lateral orbital wall (Ol) is slightly displaced. (G) Level 2 Code: 92 m.Oil.Z (m.ZEB). Orbit (left): R(li).W1(li). This case example CMTR-92-003 is made available electronically for viewing using the AOCOIAC software at www.aocmf.org/classification.
This level 2 CMF classification for the midface can be accomplished on the basis of digital volume tomography (cone beam computed tomography [CT] with adequate volume) and/or CT scans. Buitrago-Téllez et al8 provided more detailed information and discussion about imaging issues in this coding process.
Discussion
The classical facture patterns as described by Le Fort in 1901,9 10 11 based on anatomic lines of weakness, are rarely encountered in clinical practice. In addition, the classification does not address many of the important issues such as segmental fractures, the degree of comminution, and/or bone loss. Fractures of the zygoma and the wide range of orbital fractures remain unconsidered. Manson12 elaborated on the LF classification to take these issues into account, including dentoalveolar fractures as well as sagittal (vertical) fracture lines of the palatal bone. However, due to its simplicity the LF classification provided reliable and reproducible means for communication, beneath the therapeutical relevance, which is a basic requirement for a classification system. Many authors have identified the midface regions and have proposed sequences for reconstruction.13 14 15 16 17 However, there is no analysis so far of the clinical relevance of any of these treatment algorithms.
The CMF classification system presented is based on the description of clearly visible fracture lines, confirmed on the images. Previous knowledge of typical fracture patterns and common combination of fracture lines may guideline the diagnostic process of experienced clinicians, however, fractures that cannot be substantiated morphologically must not be recorded. This issue should provide a consistent assessment independent from the observers' clinical experience. However, the conciseness of the classification depends on the quality of the imaging.
Conclusion
The AOCMF classification system offers a structured midface fracture assessment tool, which is simple enough for daily routine, however, allows description of multiple fractures. The occurrence of complex fractures is well portrayed in the coding. A pure topographical classification system is not suitable to portray the diversity and the overall complexities of a midface trauma. Nevertheless, the allocation of a fracture to an anatomic region or site is deemed the initial step before more refined ways of analysis and orderly documentation as offered in the subsequent level 3 articles.2 3
Acknowledgments
This CMF classification project was funded by the AO Foundation and its AOCMF Specialty. Illustrations were prepared by AO Education (Publishing) by Jecca Reichmuth and her colleagues. The authors are grateful to all surgeons, as listed by Audigé et al,1 who participated in the successive classification sessions and provided their fruitful support in the development and validation of this midface fracture classification system.
References
- 1.Audigé L, Cornelius C P, Di Ieva A, Prein J. CMF Classification Group . The first AO classification system for fractures of the craniomaxillofaxial skeleton: rationale, methodological background, developmental process and objectives. Craniomaxillofac Trauma Reconstr. 2014;7 01:S6–S14. doi: 10.1055/s-0034-1389556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cornelius C P, Audigé L, Kunz C. et al. The comprehensive AOCMF classification system: midface fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S68–S91. doi: 10.1055/s-0034-1389561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kunz C, Cornelius C P, Audigé L. et al. The comprehensive AOCMF classification system: orbital fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S92–S102. doi: 10.1055/s-0034-1389562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Di Ieva A, Audigé L, Kellman R M. et al. The comprehensive AOCMF classification system: skull base and cranial vault fractures level 2 and 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S103–S113. doi: 10.1055/s-0034-1389563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Marsh J L Slongo T F Agel J et al. Fracture and dislocation classification compendium - 2007: Orthopaedic Trauma Association classification, database and outcomes committee J Orthop Trauma 200721(10, Suppl)S1–S133. [DOI] [PubMed] [Google Scholar]
- 6.Cornelius C P, Audigé L, Kunz C. et al. The comprehensive AOCMF classification system: mandible fractures - level 2 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S15–S30. doi: 10.1055/s-0034-1389557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cornelius C P, Kunz C, Neff A. et al. The comprehensive AOCMF classification system: fracture case collection, diagnostic imaging work up, AOCOIAC icongraphy and coding. Craniomaxillofac Trauma Reconstr. 2014;7 01:S131–S135. doi: 10.1055/s-0034-1393722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Buitrago-Téllez C H, Cornelius C P, Prein J. et al. The comprehensive AOCMF classification system: radiological issues and systematic approach. Craniomaxillofac Trauma Reconstr. 2014;7 01:S123–S130. doi: 10.1055/s-0034-1389565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Le Fort R. Étude expérimentale sur les fractures de la machoire supérieure (Part I) Rev Chir. 1901;23:208–227. [Google Scholar]
- 10.Le Fort R. Étude expérimentale sur les fractures de la machoire supérieure (Part II) Rev Chir. 1901;23:360–379. [Google Scholar]
- 11.Le Fort R. Étude expérimentale sur les fractures de la machoire supérieure (Part III) Rev Chir. 1901;23:479–507. [Google Scholar]
- 12.Manson P N. Some thoughts on the classification and treatment of Le Fort fractures. Ann Plast Surg. 1986;17(5):356–363. doi: 10.1097/00000637-198611000-00003. [DOI] [PubMed] [Google Scholar]
- 13.Gruss J S, Mackinnon S E. Complex maxillary fractures: role of buttress reconstruction and immediate bone grafts. Plast Reconstr Surg. 1986;78(1):9–22. [PubMed] [Google Scholar]
- 14.Kelly K J, Manson P N, Vander Kolk C A. et al. Sequencing LeFort fracture treatment (Organization of treatment for a panfacial fracture) J Craniofac Surg. 1990;1(4):168–178. doi: 10.1097/00001665-199001040-00003. [DOI] [PubMed] [Google Scholar]
- 15.Gruss J S, Bubak P J, Egbert M A. Craniofacial fractures. An algorithm to optimize results. Clin Plast Surg. 1992;19(1):195–206. [PubMed] [Google Scholar]
- 16.Rohrich R J, Shewmake K B. Evolving concepts of craniomaxillofacial fracture management. Clin Plast Surg. 1992;19(1):1–10. [PubMed] [Google Scholar]
- 17.Manson P N Markowitz B Mirvis S et al. Toward CT-based facial fracture treatment Plast Reconstr Surg 1990852202–212., discussion 213–214 [PubMed] [Google Scholar]