

Abstract
The AOCMF Classification Group developed a hierarchical three-level craniomaxillofacial (CMF) fracture classification system. The fundamental level 1 distinguishes four major anatomical units including the mandible (code 91), midface (code 92), skull base (code 93) and cranial vault (code 94); level 2 relates to the location of the fractures within defined topographical regions within each units; level 3 relates to fracture morphology in these regions regarding fragmentation, displacement, and bone defects, as well as the involvement of specific anatomical structures. The resulting CMF classification system has been implemented into AO comprehensive injury automatic classifier (AOCOIAC) software allowing for fracture classification as well as clinical documentation of individual cases including a selected sample of diagnostic images. This tutorial highlights the main features of the software. In addition, a series of illustrative case examples is made available electronically for viewing and editing.
Keywords: craniomaxillofacial fractures, classification system, coding, electronic documentation system
The AOCMF Classification Group developed a hierarchical three-level craniomaxillofacial (CMF) fracture classification system.1 The level 1 and level 2 systems allows fracture location within defined regions and four major anatomical units including the mandible (code 91), midface (code 92), skull base (code 93), and cranial vault (code 94). The more detailed level 3 system considers refined fracture location according to the subregions, specifically within the condylar process, zygoma, orbit, and nose, as well as morphology defined by fragmentation, displacement and bone defects, and the involvement of specific structures. In addition, the dental status and extend of bone atrophy can be described both in the mandible and in the maxilla.
This CMF fracture classification system has been implemented into AO comprehensive injury automatic classifier software (AOCOIAC). AOCOIAC is stand-alone computer-based software with user-friendly interface to support fracture diagnosis, classification, and coding via specific modules, including the Müller-AO classification2 and AO pediatric classification3 systems for long bone fractures, as well as the newly developed comprehensive CMF fracture classification1 in its updated version 4.0.
While all the detailed features of the software are presented in a user manual, this tutorial highlights its main features, allowing fracture classification and clinical case documentation including selected imaging. A series of case examples are documented and made available electronically for viewing and editing using this software (see Note and Disclaimer at the end of this paper).
Training versus Case Documentation
The software interface is designed with a series of tabs projecting out from the left upper edge of the software window. AOCOIAC starts with a training tab only with the depiction of two skeletons providing access to available classification modules, related to adult and pediatric systems, respectively (Fig. 1). Each module is activated by clicking on the respective anatomical area, such as the adult skull for the CMF classification system. When accessing the CMF classification module via the training tab, the classification system can be tested and experienced with all its functionalities, however it is not possible to save the classification data from clinical cases. To save and document clinical cases, the user must first log-in to the built-in database using the “log-in” icon on the top-right corner of the software window. Each user must be registered within specific access rights by a designated user administrator. The database can be installed locally on a computer hard drive, or on a central server that can be accessed by working stations installed with AOCOIAC.
Figure 1.
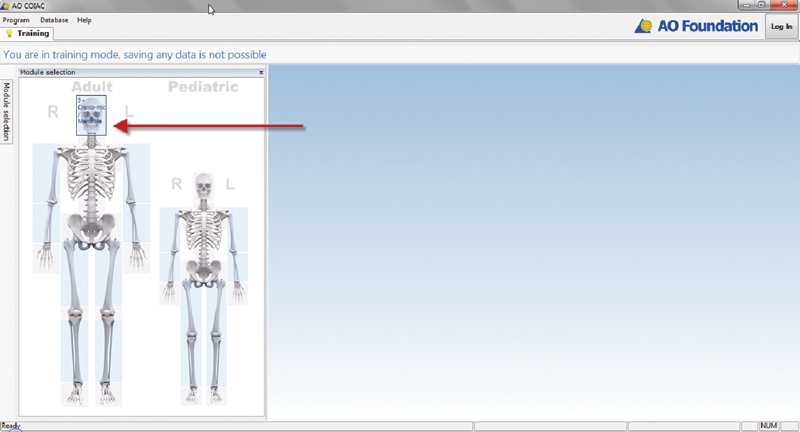
AOCOIAC entry screen. AOCOIAC, AO comprehensive injury automatic classifier software.
In the first part of this tutorial we will briefly present the functionality of the CMF classification module from the training tab, then in the second part explain how case documentation can be implemented following user log-in.
Craniomaxillofacial Classification Module
The CMF classification module is organized and presented to facilitate fracture coding according to any of the three levels of the classification (Fig. 2). On the top-left corner of the windows interface, the skull is presented for level 1 classification; on the left column and top row, respectively, illustrations of the mandible and cranium give access to level 2 and level 3 classifications. By clicking the mouse pointer on the desired illustrative view, a corresponding larger illustration is presented in the central window with delimitations of level 2 regions or level 3 subregions depending on the selected view. On the top row a panoramic illustration of the zygomas, orbits, and nose delimits level 3 subregions for the cranium.4 5 Similarly on the left column, an illustration of both condylar processes is used for level 3 classification of condylar process subregions (head, neck, and base).6 Fracture classification may be implemented directly on the selected illustrations or using the side table on the right side of the screen window. In the following, we will focus essentially on the illustrations, and refer to the side table as appropriate. We consider the classification of a mandibular fracture first and then highlight some specificities of classifying fractures of the cranium.
Figure 2.
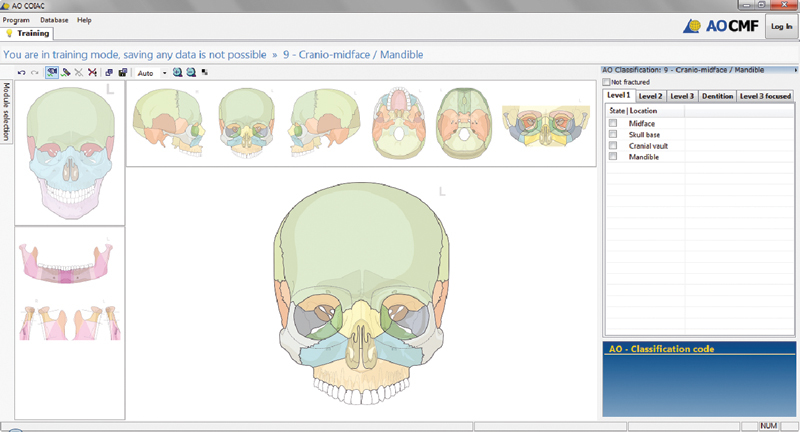
CMF classification module window in AOCOIAC. AOCOIAC, AO comprehensive injury automatic classifier software; CMF, craniomaxillofacial.
It should be noted at this stage that it is most practical to classify fractures using AOCOIAC by viewing and assessing diagnostic images at the same time on a separate computer screen. In AOCOIAC, the panoramic view of the mandible has been selected (Fig. 3). To support the classification process, the mouse pointer can be transformed into a pen by double click within the central window anywhere outside the illustration (and vice versa); the pen can be used to draw the fracture line(s) as observed on the diagnostic images. The regions or subregions corresponding to drawn lines are selected as fractured, in accordance with rules and definitions (e.g., location inside the transition zones of the mandible7). An important issue in the classification process is that when selecting one or more level 2 regions as fractured, all other regions that are not explicitly categorized as fractured are not considered as fractured. The same principle applies to the classification of level 3 subregions.
Figure 3.

Classification by fracture drawing or mouse click. (A) A fractured region (level 2) is set in blue. (B) At the level 3 classification, lack of fragmentation, minor fragmentation (or simply "fragmentation" in the cranium) and major fragmentation (in the mandible) are show in yellow, (C) orange, and (D) red, respectively. (D) Partial edentulism and mild mandibular atrophy is illustrated.
A double click with the mouse pointer on a region or subregion of interest opens up menu window tabulating level 2 and level 3 descriptors to specify the fracture in greater detail (Fig. 3). Using the menu windows, regions that are difficult to analyze or evaluate (e.g., due to lack or shortages in diagnostic imaging) can be indicated as “undetermined.”
The classification process may be restricted to the level 1 or level 2, not taking the features of fracture morphology within level 3 into account. If level 3 is applied, it is reasonable that all affected regions are classified uniformly at this level to comply with a clear and concise layout. Marking of a level 3 descriptor such as the fragmentation grade in a region or subregion, however, will automatically retroactivate the level 1 and level 2 classifications and can be used as a shortcut and timesaver in the coding process.
All level 3 classification features can be chosen interactively by use of the illustrations, with one exception: the direction of displacement for condylar process fractures; this information can only be recorded via the entry table on the right side of the screen window.
The user can switch the colored background regions in the illustration into black and white for better viewing of the marked fractures and their features. When a region or a subregion is set as fractured, it will be colored in blue (Fig. 3). At the level 3 classification, lack of fragmentation, minor fragmentation (or simply “fragmentation” in the cranium) and major fragmentation (in the mandible) are show in yellow, orange, and red, respectively. Bone loss is shown with additional stripes.
The dentition status can be determined by selecting (i.e., by double click) the concerned tooth or teeth. A classification window allows determining preinjury edentulism or tooth injuries (loss, fracture, or loosening). In case of edentulism, the level of mandibular or maxillary atrophy can be set within the classification dialogue window of the concerned region. This item remains disabled in case of full dentition.
Common fracture patterns in the midface including Le Fort (LF) types I, II, and III, zygoma en bloc (ZEB) and nasoorbitoethmoidal (NOE) can be specified within the classification menu windows of the involved regions. The regions involved in any specified pattern are highlighted in purple such as in bilateral LF patterns (Fig. 4). NOE and ZEB patterns are also illustrated within the detailed panoramic view of the midface.
Figure 4.
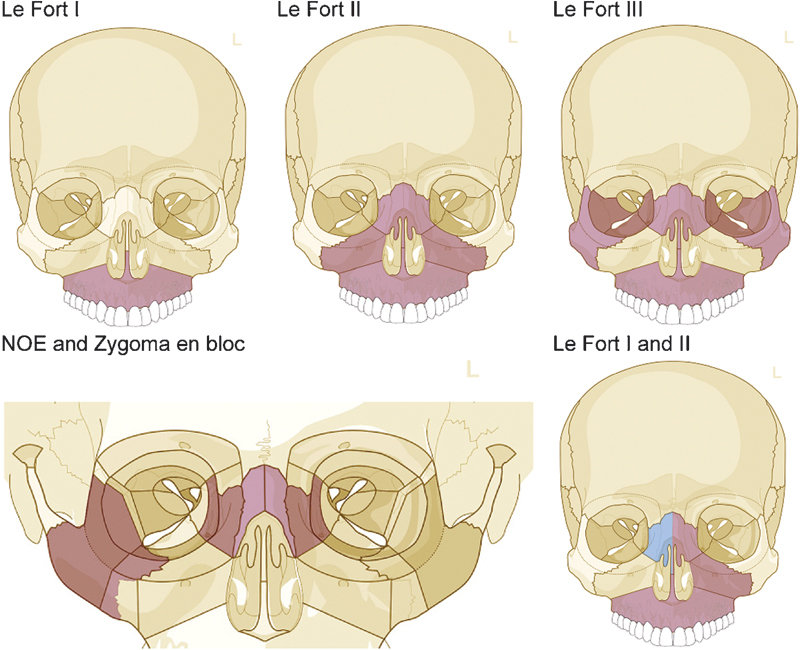
Common midface fracture patterns available for classification.
After completion of the classification, the fracture code is presented within the bottom-right screen window (Fig. 5A). The codes can be copied to the computer clipboard following double click of the mouse over them. The related illustrations, including drawn fracture lines, can be copied or saved electronically for use in publications and presentations. Direct access to the AOCMF Surgery Reference portal (Fig. 5B) at a remaining basic level of the classification is provided by selecting the icon “AO Surg. Ref.” on the right of the fracture code.
Figure 5.
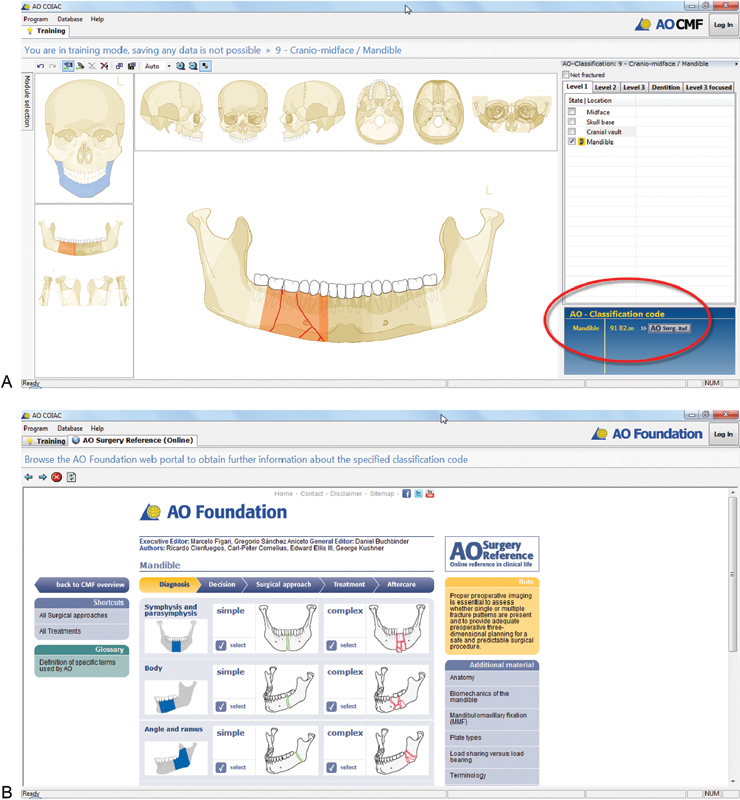
Fracture classification coding and link to surgery reference. (A) After completion of the classification, the fracture code is presented within the bottom-right screen window. (B) Direct access to the AOCMF Surgery Reference portal is provided by selecting the icon on the right of the fracture code.
Documentation Database
The log-in button on the top-right corner of the screen provides access to a database for password-protected case documentation. After log-in, two new tabs are made available, namely, the searching and patients tabs (Fig. 6).
Figure 6.
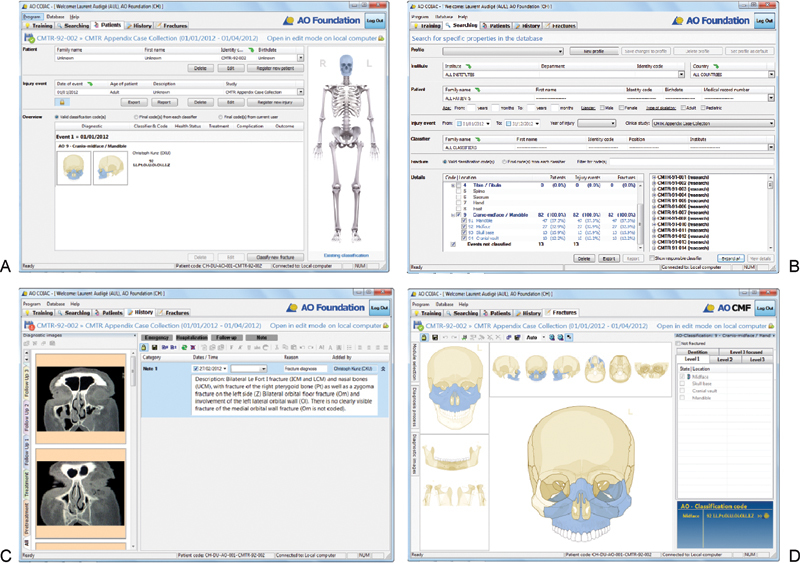
AOCOIAC software screen shots. AOCOIAC, AO comprehensive injury automatic classifier software. (A) Patient tab. (B) Searching tab. (C) History tab. (D) Fracture tab.
The patient tab (Fig. 6A) is used to select individual records, based on patient and injury event data, or enter new records. A window allows visualization of the fracture diagnosis and coding made by each classifier.
The searching tab (Fig. 6B) allows displaying the number of documented cases, which can be filtered according to several parameters. Such parameters include for instance the institute, classifier name, patient age or gender, event date or year, participation into a clinical study, or all or part of classification codes. A window presents basic frequency statistics on the number of patients, events, and fractures per location (level 1 system). Upon selecting the filters, the statistic details window is updated, and the list of related cases is presented within the bottom-right window. This list can be expended for all or any case to present the related event(s) and fracture code(s), which can be selected for direct opening within the patient and fracture tab, respectively. Filtered cases and selected classification modules within the statistic details window can be deleted from the database (only with appropriate rights) or exported as binary file for sharing by other AOCOIAC users, or as text-delimited files for further data management and analyses. An option for case pseudonymization is available at the time of export.
After registering or opening a patient and one associated injury event, two new tabs are made available, namely, the history and fractures tabs.
The history tab (Fig. 6C) allows documentation of hospitalization and clinical examination data using text notes, as well as a representative selection from the diagnostic (e.g., radiograph or computed tomography scans) imaging.
The fractures tab (Fig. 6D) allows access to the CMF classification module for any new classification by selecting the cranium on the presented skeleton. The process of classification using the fracture tab is similar to that presented above using the training tab; however it is possible then to save the generated diagnoses and codes in the case documentation database. In addition, the same injury may be classified by multiple users and all codes are saved. The code generated last by any user is considered the valid code (e.g., in the context of a fracture register). In the patient tab, an overview window provides the registered fracture codes and associated classifiers. When opening a case that was already classified, the fractures tab can open directly to the classification without presenting the skeleton. This shortcut can be obtained by double clicking on the related icon within the overview window of the patients tab.
Case Examples
All tutorial articles in this issue are illustrated by case examples that were formatted by means of the actual AOCOIAC CMF module (version 4.0). Graphical representations of the classified cases are shown along with selected diagnosis images and descriptive text. Additional cases typically seen in clinical practice, ranging from simple nonfragmented fracture confined in a single region to complex panfacial trauma, were selected for presentation in an electronic appendix available from the Journal Web site. The whole series of cases are also made available in AOCOIAC binary format for direct import into the software (www.aocmf.org/classification), such as presented in Fig. 7 (mandibular fracture) and in Fig. 8 (midface/zygomatic fracture).
Figure 7.
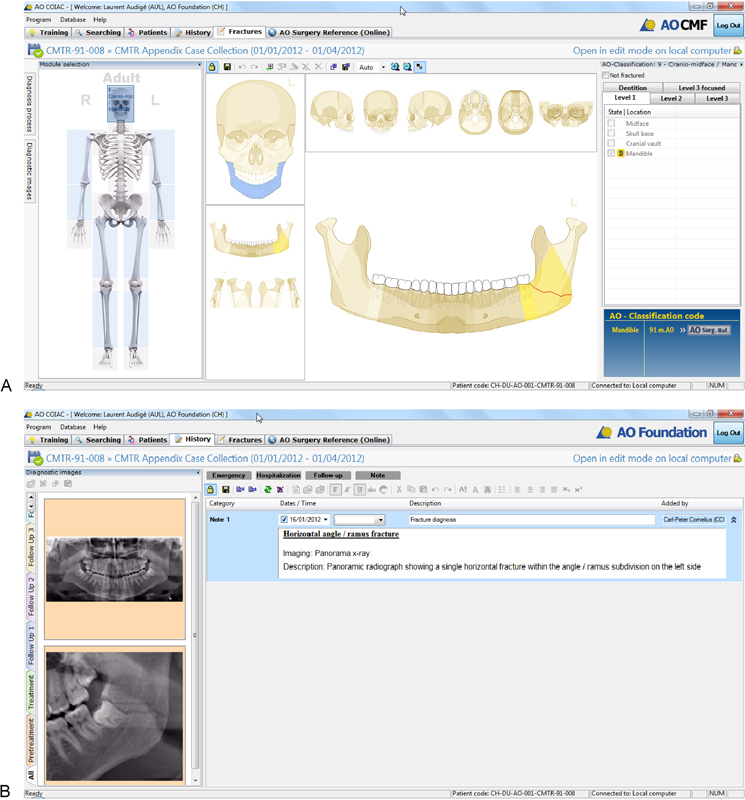
Mandibular fracture documentation. (A) After registering patient and trauma event using the patient tab, fracture classification is implemented via the fracture tab. (B) Case images and clinical history are documented using the history tab.
Figure 8.
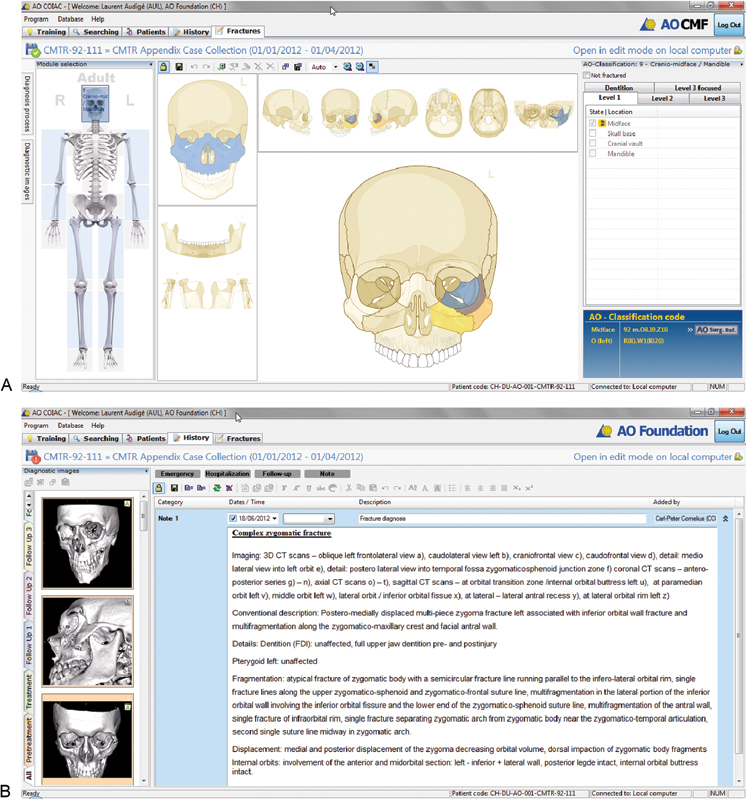
Midface/zygomatic fracture documentation. (A) After registering patient and trauma event using the patient tab, fracture classification is implemented via the fracture tab. (B) Case images and clinical history are documented using the history tab (B).
Discussion
The AOCOIAC is a unique software solution for classification and documentation of fractures using the new AO CMF classification system. At the initiation of this development, participating surgeons recognized the need for electronic software support for the systematic and standardized diagnosis process of complex facial injuries. The precursor of AOCOIAC was Buitrago craniofacial fracture automatic classifier software.8 This software included initially only the mandible and was used to generate a fracture classification code without database for documentation. It was extended to include the cranium, at the initiation of the CMF classification project1 and was used for the evaluation of a CMF injury severity score in relation to clinical findings.9
Only few other authors previously presented option for comprehensive assessment of CMF fractures. Catapano et al10 proposed a comprehensive method for panfacial fracture documentation and severity scaling. In their system, the fracture pattern is recorded by coding separately 41 anatomical regions according to one of the four categories: 0 = no fracture, 1 = single undisplaced or minimally (≤2 mm) displaced fracture, 2 = single displaced (> 2 mm) fracture or comminuted fracture, and 3 = bone loss. A graphical scheme is used to support the diagnosis process; however it was not to our knowledge transferred into a software solution. Recently Ahmad et al11 proposed a new scoring system for craniofacial fractures that was incorporated into a database system to support documentation.
The AOCOIAC is the most advanced software solution available to classify and document fractures of the CMF skeleton. It is a tool to initiate systematic documentation and evaluation of CMF fractures. We encourage all CMF surgeons to adopt it and participate in its further development.
Technical Requirements
AOCOIAC can be installed either locally for single users (A) or as server-client installation for use in the clinical setting by multiple users (B).
-
Minimal configuration: AOCOIAC with local database (client/server installation)
Windows XP 32 bit (with IE7 - incl. all updates or higher), Windows Vista 32/64 bit, Windows 7 32/64 bit , Windows 8 32/64 bit
Intel Core 2 Duo, 2GHz
2 GB RAM
XGA (1024 × 768) True Color (24/32 Bit) 128 MB RAM
Free hard disk space 5 GB (in accordance with your requirements)
TCP/IP protocol support, Setup requires administration rights.
-
AOCOIAC for server database access (client installation)
Windows XP 32 bit (with IE7 incl. all updates), Windows Vista 32/64 bit, Windows 7 32/64 bit , Windows 8 32/64 bit
Intel Pentium 4, 2GHz
512 MB RAM
XGA (1024 × 768) True Color (24/32 Bit) 128 MB RAM
Free hard disk space 200 MB
TCP/IP protocol support, Setup requires administration rights
-
Note for Macintosh, Linux, Solaris users
This software AO COIAC can be run using a ×86 and AMD64/Intel64 virtualization software (virtual machine) such as using the freely available “VirtualBox” (www.virtualbox.org).
A Windows license is required.
Acknowledgments
This CMF classification project was funded by the AO Foundation and its AOCMF Specialty. Illustrations were prepared by AO Education (publishing) by Jecca Reichmuth and her colleagues. The programming of AOCOIAC was performed by Dirk Sauter (Ingenieurbüro Marschelke, Reichenau, Germany). The authors are grateful to all surgeons, as listed by Audigé et al,1 who participated in the successive classification sessions and provided their fruitful support in the development and validation of this fracture classification system.
Note and Disclaimer
An electronic copy of the AOCOIAC software and its user manuals can be obtained at the following Web site: www.aofoundation.org/aocoiac. While the developers thrived to make this software as user-friendly and useful as possible, they cannot guarantee it is problem-free and will work adequately on all computers. The user manual should be read carefully before installation and use. The AO Foundation cannot take responsibility for any damages or inconveniences that may occur by using the available most current software version. All case examples presented in this special issue of the Journal are made available in AOCOIAC binary format for direct import into the software, and can be downloaded at the following Web site: www.aocmf.org/classification. For use of the AOCOIAC software, its manuals, and all case examples, the AO Foundation terms, conditions, and disclaimers apply (https://www.aofoundation.org/Structure/the-ao-foundation/Pages/legal.aspx).
References
- 1.Audigé L, Cornelius C P, Di Ieva A, Prein J. CMF Classification Group . The first AO classification system for fractures of the craniomaxillofaxial skeleton: rationale, methodological background, developmental process and objectives. Craniomaxillofac Trauma Reconstr. 2014;7 01:S6–S14. doi: 10.1055/s-0034-1389556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Müller M, Narzarian S. Berlin: Springer; 1990. The Comprehensive Classification of Fractures of Long Bones. [Google Scholar]
- 3.Slongo T Audigé L The comprehensive AOCMF classification system: midface fractures - level 3 tutorial J Orthop Trauma 200721(10, Suppl):S135–S160. [DOI] [PubMed] [Google Scholar]
- 4.Cornelius C P, Audigé L, Kunz C. et al. The comprehensive AOCMF classification system: midface fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S68–S91. doi: 10.1055/s-0034-1389561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kunz C, Audigé L, Cornelius C P. et al. The comprehensive AOCMF classification system: orbital fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S92–S102. doi: 10.1055/s-0034-1389562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Neff A, Cornelius C P, Rasse M. et al. The comprehensive AOCMF classification system: condylar process fractures - level 3 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S44–S58. doi: 10.1055/s-0034-1389559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cornelius C P, Audigé L, Kunz C. et al. The comprehensive AOCMF classification system: mandible fractures - level 2 tutorial. Craniomaxillofac Trauma Reconstr. 2014;7 01:S15–S30. doi: 10.1055/s-0034-1389557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Buitrago-Téllez C H, Audigé L, Strong B. et al. A comprehensive classification of mandibular fractures: a preliminary agreement validation study. Int J Oral Maxillofac Surg. 2008;37(12):1080–1088. doi: 10.1016/j.ijom.2008.06.008. [DOI] [PubMed] [Google Scholar]
- 9.Bächli H, Leiggener C, Gawelin P. et al. Skull base and maxillofacial fractures: two centre study with correlation of clinical findings with a comprehensive craniofacial classification system. J Craniomaxillofac Surg. 2009;37(6):305–311. doi: 10.1016/j.jcms.2009.01.008. [DOI] [PubMed] [Google Scholar]
- 10.Catapano J, Fialkov J A, Binhammer P A. et al. A new system for severity scoring of facial fractures: development and validation. J Craniofac Surg. 2010;21(4):1098–1103. doi: 10.1097/SCS.0b013e3181e1b3c1. [DOI] [PubMed] [Google Scholar]
- 11.Ahmad Z, Nouraei R, Holmes S. Towards a classification system for complex craniofacial fractures. Br J Oral Maxillofac Surg. 2012;50(6):490–494. doi: 10.1016/j.bjoms.2011.09.018. [DOI] [PubMed] [Google Scholar]