

Abstract
Aim:
To systematically review articles on canal centering ability of endodontic rotary cutting Nickel-Titanium (Ni-Ti) instruments and subject results to meta-analysis.
Materials and Methods:
A comprehensive search was initiated on canal centering ability of different rotary cutting Ni-Ti files such as Protaper, Hero Shaper, K3, Mtwo, Race, Wave One by selecting articles published in peer reviewed journals during 1991-2013 using “Pub Med” database. Inclusion and exclusion criteria were established. A data was created by tabulating: Author name, publication year, sample size, number of experimental groups, methods to evaluate canal centering ability, instrument cross section, taper, tip design, rake angle, mean and standard deviation. The data generated was subjected to meta-analysis.
Results:
Maximum studies were found to be conducted on mesiobuccal canal of mandibular 1st molar with curvature ranging from 15-60°. The difference in canal centering ability of different rotary cutting Ni-Ti instruments was not statistically significant.
Conclusion:
All endodontic rotary cutting Ni-Ti instruments are capable of producing centered preparations. Protaper depicted the best centering ability. Computed tomography is an effective method of evaluating canal centering ability.
Keywords: Centering ability, meta-analysis, Ni-Ti rotary files, systematic review
INTRODUCTION
It has been suggested that successful root canal treatment is dependent on effective biomechanical preparation and thorough cleaning and shaping of the root canal systems. The introduction of Nickel-Titanium (Ni-Ti) rotary files in endodontics almost two decades ago has changed the way root canal preparations are performed, enabling more complicated root canal systems to be shaped with fewer procedural errors. Since inception in 1993 when Serene et al. extensively tested and marketed the first Ni-Ti rotary files, some of the more than 30 current Ni-Ti instruments systems on the market are classified according to their design, shaping characteristics, breakage potential, and clinical performance.[1] Out of which shaping or centering ability, which is the ability of an instrument to remain centered in the root canal system is the most important characteristic to be studied. A number of studies on both extracted teeth and simulated canals have shown that rotary Ni-Ti instruments allow more rapid, more centered canal preparations than stainless steel instruments (Glossen et al. 1995, Kum et al. 2000).[2,3] The centering ability of different rotary Ni-Ti instruments was also compared according to their design features such as taper and cross-sectional design. Most of these studies are on Protaper (progressive taper) file system. Centering ability of Protaper was compared with other rotary Ni-Ti files by different methods like cone beam computed tomography (CBCT), micro-CT, spiral CT, stereomicroscopic magnifier, digital camera with superimposed images etc. on mesiobuccal canal of maxillary or mandibular teeth or in simulated canals. But all these studies have variable results, no systematic review and none has quantified the centering ability or defined their statistical significance.
With the rise of evidence-based dentistry in the last two decades, systematic reviews and meta-analysis have been widely used for synthesis of evidence on beneficial and/or harmful effects of different designs of rotary files. Results from these reviews and meta-analyses provide important information for drawing clinical guidelines regarding performance of different file systems and making recommendations.[4]
Even though in endodontics, centering ability is one of the parameters used more frequently to know the performance of the file, there is no statistical correlation between it and other important characteristics like file design. There are many studies that have compared the centering ability of different file systems but none has quantified their importance or defined their statistical significance. Hence, this study was undertaken to systematically evaluate the comparative studies of centering ability of Protaper and different rotary cutting Ni-Ti instruments. This quantitative overview could be considered as a meta-analysis study performed under non experimental conditions to assess the effects of certain clinical parameters on centering ability of different rotary Ni-Ti files.
MATERIALS AND METHODS
Literature search
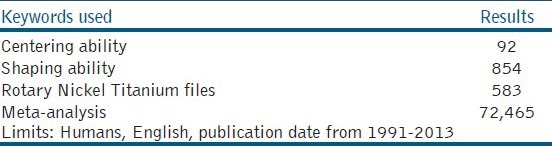
A comprehensive search was initiated on canal centering ability of different rotary cutting Ni-Ti files such as Protaper, Hero Shaper, K3, Mtwo, Race, Wave One by selecting articles published in Peer reviewed journals during 1991-2013 using “Pub Med” database. The articles were assessed and selected on the basis of keywords such as: Centering ability, shaping ability, apical transportations, nickel-titanium, rotary files, systematic review, and Meta-analysis [Table 1].
Table 1.
Results of Pub Med search
Inclusion criteria
Study with original data.
Articles published in English.
Studies with statistical analysis.
Comparison of centering ability of different rotary Ni-Ti files.
Study in mesiobuccal canal of human mandibular 1st molar with degree of curvature 15-60°.
Studies involving pre- and post-operative images of cross section at three different levels.
Study with minimum of 20 samples in each group.
Exclusion criteria
Articles displaying only graphic data.
Studies without statistical analysis.
Study in simulated canals.
Comparison of centering ability of rotary file systems other than protaper.
Data extraction
The data was extracted and tabulated by Author name, publication year, sample size, number of experimental groups, methods to evaluate canal centering ability, instrument cross section and taper, tip design, rake angle, mean and standard deviation. Studies in vivo that compared canal centering ability of Protaper with other rotary Ni-Ti files such as Hero shaper, K3, Mtwo, Wave One were identified. Articles were screened, out of which eight met the inclusion criteria. In total, from each study mean and standard deviation of centering ability of Protaper File with other rotary Ni-Ti files at different levels were extracted and tabulated. An excel sheet was prepared in which the file system used, tooth, root, root canal, degree of curvature, root section, number of samples, method of evaluation, formula used, software used, taper of files, and apical preparations of these eight studies were compared with each other.
Calculation of centering ability
Gambill et al. (1996)[5] defined centering ratio as the measurement of the ability of the instruments to stay centered in the canal [Figure 1]. This ratio was calculated as follows:
Figure 1.
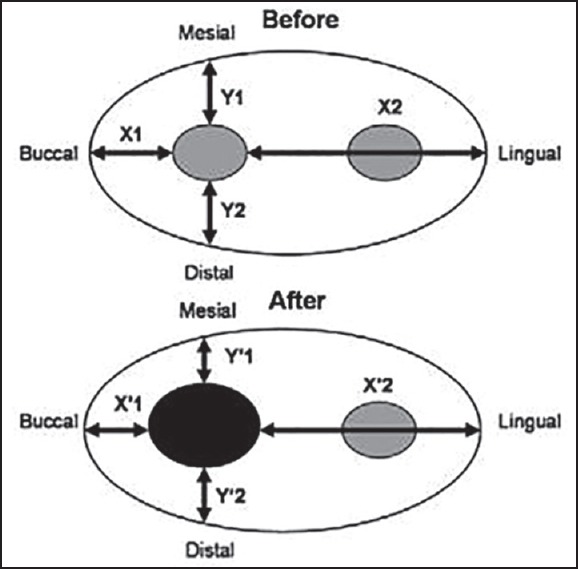
Schematic representation of the images used in the evaluation
D1: X1 X2 = (X1-X´1) (X2-X´2)
D2: Y1 Y2 = (Y1-Y´1) (Y2-Y´2)
A result of 1 indicates perfect centering. The closer the result to zero, the worst the ability is after instrument to remain centered.
The observations were subjected to Meta-analysis using the meta-analysis software system Meta-analysis In eXcel (MIX) 2.0 Professional. Forest plot was plotted to assess heterogeneity among studies and Funnel plot was used to show publication bias.
What is meta-analysis?
A statistical analysis that combines or integrates the results of several independent clinical trials considered by the analyst to be combinable. It is a reliable method of synthesizing published information and providing direct evidence to clinical practice. Forest plot and Funnel plot are obtained using meta-analysis Software. Forest plots are graphical representations of the results of meta-analysis. In forest plot, each study is represented by a line. It also provides the summary data entered for each study. In addition, it provides the weight for each study; the effect measure, method, and the model used to perform the meta-analysis; the confidence intervals used; the effect estimate from each study, the overall effect estimate, and the statistical significance of the analysis. Funnel plots are graphical aids in which an estimate of underlying quantity is plotted against interpretable measure of its precision. If publication bias is not present, funnel plot is roughly symmetrical. If funnel plot is not symmetrical and does not resemble an inverted funnel then publication bias are seen.
RESULTS
Data summary of included studies
Five articles met the inclusion criteria and were selected for the final analysis.[6,7,8,9,10]
Mesiobuccal canal of mandibular 1st molar was used in five studies and maxillary molars in three studies.
Transverse section of roots was used. Number of samples ranged from 20-90.
The file system Protaper universal, Twisted file were used in three studies; Profile vortex, Hero Shaper in two studies; Revo S in two studies; RaCe in two studies; Greater taper, Mtwo, K3 in one study each.
The degree of curvature ranged from 15-60°.
Micro-CT, stereomicroscopic magnifier and spiral CT were used in two studies each, CBCT and digital camera was also used.
Reciprocating motion was used in all file systems.
Meta-analysis
The meta-analysis Software System MIX 2.0 Professional was used to perform the meta-analysis.
Forest plot depicted that chi square test for heterogeneity is significant i.e. 85% and confidence interval is narrow. So, there was heterogeneity in the studies. This plot depicted that Protaper has more centering ratio when compared with other Ni-Ti files like Hero Shaper but was not statistically significant [Figure 2].
Figure 2.
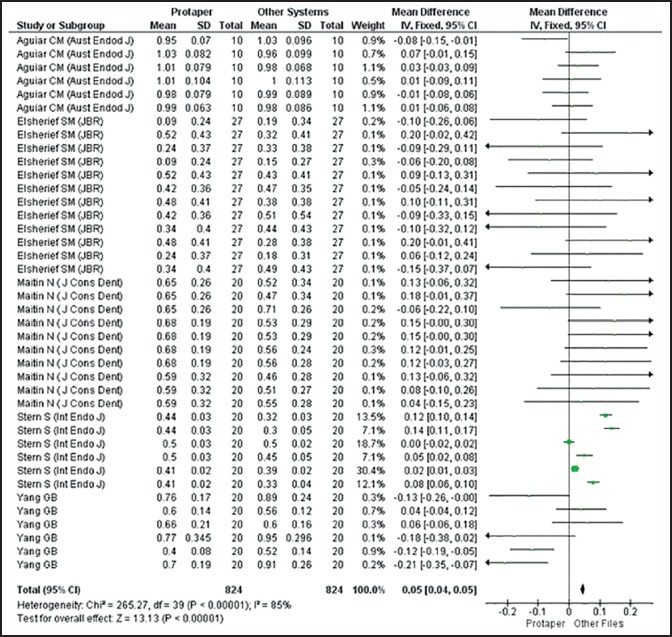
Forest plot of included studies
Funnel plot is not a very reliable method of investigating publication bias, although it does gives us some idea of whether our study results are scattered symmetrically around a central, more precise effect. Funnel plot asymmetry may be due to publication bias but it may also result from clinical heterogeneity between studies due to different control event rates or methodological heterogeneity between studies. The circles represent studies and maximum are within funnel so low publication bias. Absence of bias indicates symmetrical and inverted funnel [Figure 3].
Figure 3.
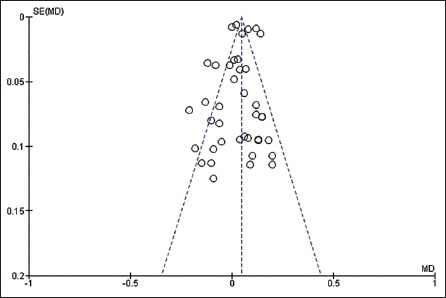
Funnel plot of included studies
DISCUSSION
Meta-analysis is the statistical analysis of a collection of analytic results for the purpose of integrating the findings. The advantage of meta-analysis over the traditional literature review is the possibility of combining results from many studies to establish statistical significance with studies that have conflicting results and also to develop a more correct estimate of effect magnitude and provide a more complex analysis of data. It is also used to examine subgroups with individual numbers that are not statistically significant. Thus, it is one of the important tools for the evidence based dentistry.
The aim of bio-mechanical preparation of root canal is to form a continuously tapered shape with the smallest diameter at the apical foramen and the largest at the orifice to allow effective irrigation and filling, without any deviation from the original trajectory in curved and thin canals using techniques and instruments which have the greatest precision and shortest working time. Many instruments have been recommended but only a few seem to be capable of achieving these primary objectives of root canal preparation consistently. Ni-Ti instruments are mainly used because they have greater flexibility and capacity for maintaining the original configuration without creating any iatrogenic events such as canal transportations etc. Since their introduction in 1993 by Serene et al., numerous Ni-Ti rotary systems are introduced and their canal centering ability is studied by various researchers. In most of these studies centering ability of Protaper was compared with other Ni-Ti files with varying results. Variations in results could be due to variation in file design, taper of different files, tip design, method to study centering ability, apical preparation diameters required for the comparisons of the shaping and cleaning ability of different root canal instruments.[1]
Meta-analysis was conducted to minimize bias and random error. In the studies selected from articles centering ability was calculated from pre and post-instrumentation canal thickness measurements by calculating ratio as given by Gambill et al. 1996.[5] All these studies were conducted on either maxillary or mandibular molars with curvature ranging between 15-60°. In these studies, Protaper was compared with Protaper Universal (PU), Twisted file (TF), Profile vortex, Revo S, Hero shaper, Mtwo, Race, Twisted file, Stainless steel, GT rotary. Studies on simulated canals were not included for meta analysis as these studies do not give variation in the results due to variation in the canal anatomy and dentin hardness.
In forest plot, each study is represented by a line. Width or length of the line represents confidence interval for effect estimate of each study. There is a box in a line for each study. Midpoint of the box represents weight given to each study. This is done so that eyes are drawn towards studies given more weight. Diamond represents overall effect. Width of the diamond represents confidence interval for overall effect estimate. 95% confidence interval means that there is 95% chance that true effect will lie in the same range. Vertical middle line is line of no effect. The Forest plot also provides the summary data entered for each study. In addition, it provides the weight for each study; the effect measure, method and the model used to perform the meta-analysis; the confidence intervals used; the effect estimate from each study, the overall effect estimate, and the statistical significance of the analysis.
Funnel plot is plotted to measure publication bias. The circles represent studies and maximum are within funnel so low publication bias. Absence of bias indicates symmetrical and inverted funnel.
Point estimate is best guess of the true effect in the population. Ninety-five percent confidence intervals mean that there is a 95% chance that the true effect in the population will lie within the range. They also mean that if the trial is repeated, there is a 95% chance that the point estimate from the trial lies within the 95% confidence intervals obtained in the systematic review. These are based on the sample being representative and the assumption that there are no systematic errors that can bias the results.
Different cross-sectional geometries of rotary instruments are believed to increase cutting efficiency, consequently reducing contact areas and torsional loads. Protaper instruments, in particular, were developed with a non-radial land design intended for more effective cutting. In addition, these instruments present multiple tapers over the length of their cutting blades that are designed to allow each instrument to engage a smaller zone of dentin. The protaper rotary instruments have a convex triangular cross-sectional design and a non-cutting safety tip. The basic sequence of protaper universal exhibits an advanced flute design that combines multiple tapers within the shaft, a convex triangular cross-sectional design, blades close to the non-cutting pilot tip as well as an increasing chip space (space for the accumulation of debris) from tip to shaft.
The methods commonly used for evaluating canal shaping ability are radiographs[11], tooth sections,[12] and plastic blocks.[13] Several methodologies have been proposed to assess the action of endodontic instruments on the canal walls such as radiographic platform superimposing images of before and after instrumentation, muffle system and CT, which is the most current methodology for this type of analysis. The use of CT has been suggested for this purpose because it is a nondestructive method that allows measuring the amount of root dentin removed by endodontic instruments. Cone beam computed tomography is a three-dimensional high-resolution imaging method. Furthermore, CBCT images permit nondestructive and metrically exact analyses of variables such as volume, surface areas, cross-sectional shape, and taper. The fraction of prepared surface can be analyzed with software which does not interfere in the original format of the images(digital imaging communications in medicine, DICOM), permitting the analysis of the exact position and direction of canal transportation by CT scans obtained in voxel for three-dimensional analyses which allows the determination of the values of radiological density.[14] In this Meta-analysis, CBCT was used as a tool in 2 studies i.e., by Cesar Augusto Pereira OLIVEIRA[15] and Samia M. Elsherief.[10]
Cesar Augusto Pereira OLIVEIRA et al. (2009)[15] analyzed the apical third of curved roots after mechanical preparations with different rotary systems and Samia M. Elsherief et al. (2013)[10] analyzed the curved root canals with three different nickel titanium rotary instruments after mechanical preparation. Both of them found CBCT to be the most accurate method of assessing the centering ability of root canal system.
In the last decade although a new statistical methodology, named network meta-analysis, has been developed,[16] which incorporates all available evidence into a general statistical framework for comparisons of all available treatments. Thus, network meta-analysis may play an important role in the improvement of the decision making process by optimizing the use of the existing data.
CONCLUSION
This article reviewed the literature to compare the differences in the canal centering ability of different rotary cutting Ni-Ti instruments. When it comes to the selection of file system in clinical conditions, we should all consider all the factors that would influence the centering ability. The size of the taper is one of the main factors involved in apical root transportation. All rotary cutting Ni-Ti instruments showed the ability to remain centered in the root canals and capable of producing centered preparations. Although there was a difference as Protaper showed better centering ability than others however this difference was not statistically significant. CBCT was found to be the most effective method of evaluating canal centering ability. Because of a wide variety of factors would influence the centering ability, the clinician should be selective in choosing the file system that best fits the individual needs of each tooth.
ACKNOWLEDGEMENTS
The authors thank Dr. Puneet Gupta for their assistance in processing the data.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Serene TP, Adams JD, Saxena A. St. Louis: Ishiaku EuroAmerica; 1995. Nickel-Titanium instruments: Applications in Endodontics. [Google Scholar]
- 2.Glossen CR, Hiller RH, Dove B, del Rio CE. A comparison of root canal preparations using Ni-Ti hand, Ni-Ti engine-driven, and K-Flex endodontic instruments. J Endod. 1995;21:146–51. doi: 10.1016/s0099-2399(06)80441-3. [DOI] [PubMed] [Google Scholar]
- 3.Kum KY, Spängberg L, Cha BY, Il-Young J, Msd, Seung-Jong L, et al. Shaping ability of three ProFile rotary instrumentation techniques in simulated resin root canals. J Endod. 2000;26:719–23. doi: 10.1097/00004770-200012000-00013. [DOI] [PubMed] [Google Scholar]
- 4.Ades AE, Sculpher M, Sutton A, Abrams K, Cooper N, Welton N, et al. Bayesian methods for evidence synthesis in cost-effectiveness analysis. Pharmacoeconomics. 2006;24:1–19. doi: 10.2165/00019053-200624010-00001. [DOI] [PubMed] [Google Scholar]
- 5.Gambill JM, Alder M, del Rio CE. Comparison of nickel titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996;22:369–75. doi: 10.1016/S0099-2399(96)80221-4. [DOI] [PubMed] [Google Scholar]
- 6.Southard DW, Oswald RJ, Natkin E. Instrumentation of curved molar root canals with the Roane technique. J Endod. 1987;13:479–89. doi: 10.1016/S0099-2399(87)80015-8. [DOI] [PubMed] [Google Scholar]
- 7.Bramante CM, Berbert A, Borges RP. A methodology for evaluation of root canal instrumentation. J Endod. 1987;13:243–5. doi: 10.1016/S0099-2399(87)80099-7. [DOI] [PubMed] [Google Scholar]
- 8.Weine FS, Kelly RF, Lio PJ. The effect of preparation procedures on original canal shape and on apical foramen shape. J Endod. 1975;1:255–62. doi: 10.1016/S0099-2399(75)80037-9. [DOI] [PubMed] [Google Scholar]
- 9.Paque F, Ganahl D, Peters OA. Effects of root canal preparation on apical geometry assessed by micro-computed tomography. J Endod. 2009;35:1056–9. doi: 10.1016/j.joen.2009.04.020. [DOI] [PubMed] [Google Scholar]
- 10.Oliveira CA, Meurer MI, Pascoalato C, Silva SR. Cone-beam computed tomography analysis of the apical third of curved roots after mechanical preparation with different automated systems. Braz Dent J. 2009;20:376–81. doi: 10.1590/s0103-64402009000500004. [DOI] [PubMed] [Google Scholar]
- 11.Elsherief SM, Zayet MK, Hamouda IM. Cone-beam computed tomography analysis of curved root canals after mechanical preparation with three nickel-titanium rotary instruments. J Biomedic Res. 2013;27:326–35. doi: 10.7555/JBR.27.20130008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lumley T. Network meta-analysis for indirect treatment comparisons. Stat Med. 2002;21:2313–24. doi: 10.1002/sim.1201. [DOI] [PubMed] [Google Scholar]
- 13.Aguiar CM, Sobrinho PB, Teles F, Câmara AC, de Figueiredo JA. Comparison of the centring ability of the ProTaper™ and ProTaper Universal™ rotary systems for preparing curved root canals. Aust Endod J. 2013;39:25–30. doi: 10.1111/j.1747-4477.2010.00276.x. [DOI] [PubMed] [Google Scholar]
- 14.Stern S, Patel S, Foschi F, Sherriff M, Mannocci F. Changes in centring and shaping ability using three nickel–titanium instrumentation techniques analysed by micro-computed tomography (μCT) Int Endod J. 2012;45:514–23. doi: 10.1111/j.1365-2591.2011.02004.x. [DOI] [PubMed] [Google Scholar]
- 15.Maitin N, Arunagiri D, Brave D, Maitin SN, Kaushik S, Roy S. An ex vivo comparative analysis on shaping ability of four NiTi rotary endodontic instruments using spiral computed tomography. J Conserv Dent. 2013;16:219–23. doi: 10.4103/0972-0707.111318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yang GB, Zhou XD, Zheng YL, Zhang H, Shu Y, Wu HK. Shaping ability of progressive versus constant taper instruments in curved root canals of extracted teeth. Int Endod J. 2007;40:707–14. doi: 10.1111/j.1365-2591.2007.01296.x. [DOI] [PubMed] [Google Scholar]