

Abstract
Objective:
To evaluate the marginal gap (MG) and absolute marginal discrepancy (MD) of full ceramic crowns with two finish line designs, shoulder and chamfer, using microcomputed tomography (micro-CT) before and after cementation.
Materials and Methods:
Sixty extracted human maxillary premolar teeth were divided into two groups based on the finish line design: Group I: 90° shoulder and Group II: 135° chamfer. The specimens were further grouped based on the type of full ceramic crown they received: Group A: Feldspathic Cerec inLab ceramic system, Group B: Cerec inLab aluminum oxide ceramic system and Group C: Lithium disilicate press ceramic system. Before cementation, five crowns from each group were scanned using micro-CT in two sections, sagittal and coronal, to determine the MG and MD values for four regions of the crown (sagittal buccal, sagittal lingual, coronal mesial and coronal distal). After cementation and thermal cycling, the scanning was repeated. Measurements were obtained from 10 points for each region, 80 points totally, to evaluate the MG and MD values. Files were processed using NRecon and CTAn software. Results were statistically analyzed using one- and two-way ANOVA and Tukey HSD tests (P = 0.05).
Results:
Full ceramic systems showed clinically acceptable marginal adaptation values. The Feldspathic Cerec inLab ceramic system generally presented the lowest variance, except in the MG values of the coronal mesial region. The MG and MD values of all ceramics increased significantly after cementation, except in the shoulder preparation design (sagittal buccal region) for MG and in the chamfer preparation design (sagittal lingual region) for MD values.
Conclusions:
Full-ceramic crowns showed clinically acceptable marginal adaptation values. The Feldspathic Cerec inLab ceramic system (Vitablocs Mark II) generally presented the lowest variance when compared with the other ceramics, except for the MG values on the mesial surface of the coronal section.
Keywords: Full ceramic crowns, marginal fit, microcomputed tomography technique
INTRODUCTION
Ceramic systems with high crystalline content were introduced in dentistry with the objective of replacing the metal frameworks used for metal ceramic crowns. Essential requirements for the clinical success of all-ceramic crown restorations include good esthetics, high fracture resistance and perfect marginal fit.[1] Cerec inLab feldspathic ceramic systems (Vitablocs Mark II) are industrially manufactured, fine-structure, feldspar ceramic blocks used to fabricate anterior crowns with Cerec Sirona inLab MC XL Computer aided design and manufacturing (CAD/CAM) systems of Sirona Dental Systems GmbH. Cerec inLab aluminum oxide ceramic systems (In-Ceram 2000 AL) are pre-sintered blocks consisting of pure aluminum oxide. In this form, which facilitates easy processing, they are used to grind enlarged bridge and crown frameworks in the inLab system. The lithium disilicate press ceramic system (IPS e.max Press) encompasses a high-stability framework material that consists of lithium disilicate (SiO2-Li2O). The restorations can be customized either by using a layering technique based on fluorapatite glass ceramic or by using the staining technique.
Poor marginal adaptation of ceramic crowns can result in damage to the tooth, periodontal tissues and the restoration.[2] Large marginal discrepancies result in dissolution of the luting agent and favor microleakage of bacteria and their byproducts.[3] As a consequence, the tooth becomes more susceptible to inflammation of the vital pulp (post-operative sensitivity),[4] secondary caries and marginal discoloration.[5]
The dental fraternity is yet to come to a consensus on what constitutes an acceptable marginal discrepancy (MD). A marginal gap (MG) ranging from 10 to 500 μm, with mean values from 50 to 100 μm, has been defined as acceptable.[6] Marginal openings ranging from 50 to 120 μm are considered to be clinically acceptable in terms of longevity.[7,8] For CAD/CAM restorations, the generally acceptable MG discrepancies are between 50 and 100 μm.[9,12]
Holmes et al.[13] define MG as the perpendicular measurement from the cervical margin of the casting to the preparation margin, and absolute MD as the angular combination of the MG and extension error (overextension or underextension). In other words, it is the combination of the vertical and horizontal MDs. According to Holmes et al.,[14] the perpendicular measurement from the internal surface of the margin of the crown or casting to the outermost edge of the finish line of the tooth margin is termed as the MG. Therefore, MG refers to the surface of the cement that is left exposed intraorally and can be dissolved, leading to secondary caries and pulp implications due to microleakage. MD, on the other hand, is indicative of the extension of the crown margins in relation to the margins of the abutment and is of great importance mainly in overextension cases, as it enhances plaque accumulation and compromises health [Figures 1 and 2].
Figure 1.
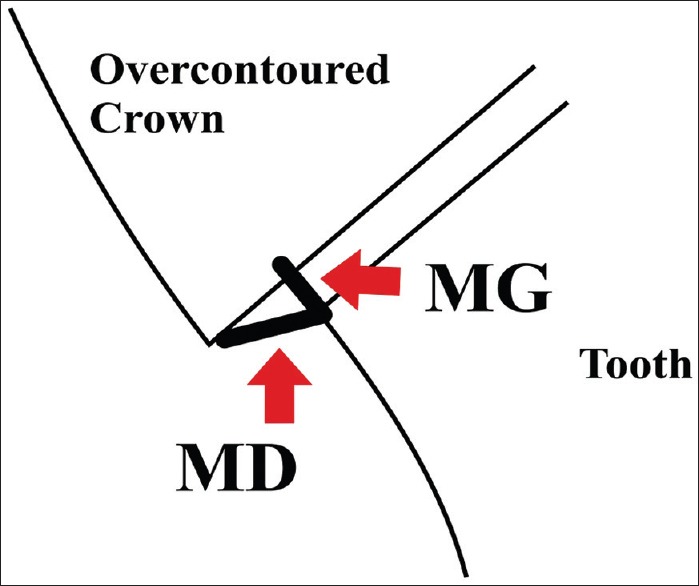
The drawings of marginal gap and marginal values
Figure 2.
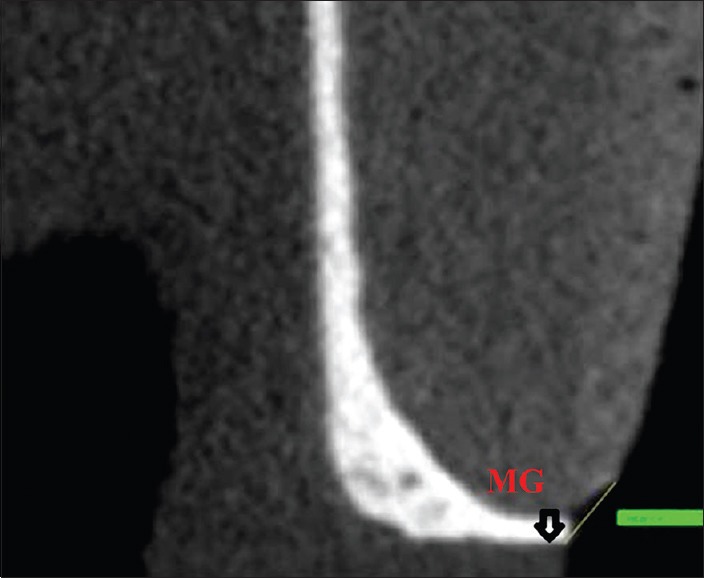
Marginal gap and marginal discrepancy measurements by microcomputed tomography
Different methods have been used to evaluate internal and MGs. The clinical marginal fit can be roughly estimated either directly with a mirror and a probe or indirectly by making an impression of the tooth and producing an epoxy replica that can be evaluated by an optical or scanning electron microscope.[14] In laboratory studies, it is possible to section the tooth–restoration sample for direct evaluation under a microscope.[15,16,17] A new method that uses microcomputed tomography (micro-CT) has been applied for non-destructive analysis of the restorations.[18,19] This technique allows 2 dimensional (2D) and 3 dimensional (3D) investigation of the marginal and internal gaps, within the range of a few micrometers, in multiple sites and directions.[18]
The hypothesis of this study was that there is no difference in the MG and MD values in different regions of the tooth, for shoulder and chamfer finish line designs, both before and after cementation and thermal cycle. The aim of this investigation was to evaluate the marginal fit of three full ceramic systems with two different finish line designs, both before and after the cementation and thermal cycle procedures.
MATERIALS AND METHODS
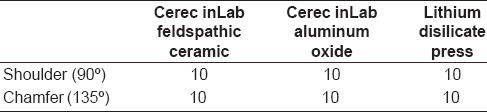
Sixty extracted human maxillary premolar teeth with no caries or anatomical defects were divided into two groups based on the finish line design [Table 1]; Group 1: 90° shoulder and Group 2: 135° chamfer. Furthermore, each group was divided into three groups to receive three different types of full ceramic crowns; Group A: Cerec inLab feldspathic ceramic system (Vitablocs Mark II, Vita Zahnfabrik, Bad Säckingen, Almanya); Group B: Cerec inLab aluminum oxide ceramic system (Vita In-Ceram 2000 AL, Vita Zahnfabrik, Bad Säckingen, Almanya) and Group C: Lithium disilicate press ceramic system (IPS e.Max Press, Ivoclar Vivadent, Schaan, Liechtenstein).
Table 1.
Groups and subgroups summarized in table
Preparation of the tooth
The preparation design according to standardized rules was completed by a computer, a 3D mechanical CAD programme - Solid Works. For Group I, the preparation design included a 90° shoulder, 1 mm deep, with smooth margins. The Group II design included a 135° chamfer, 1 mm deep, with rounded internal margins. It was 6 mm high and included a horizontal occlusal table. All sharp angles were functionally rounded and a convergence angle of 8° was established by a milling machine (Acuvey 2012 CNC Machine).
Reconstruction of full ceramic crowns
A polyvinyl siloxane impression (Aquasil™, Dentsply, Petropolis, RJ, Brazil) of the model was made and a working cast was obtained using Type IV special CAD/CAM stone (GC Fujirock EP Optixscan (GC, Leuven, Belgium). The ceramic systems were produced according to the manufacturers’ instructions. Cerec inLab feldspathic ceramic system (Group A) crowns were produced totally from CAD/CAM ingots and Cerec inLab aluminum oxide ceramic system (Group B) ceramic crowns’ core structures were also produced from CAD/CAM ingots. Lithium disilicate press ceramic system (Group C) crowns were customized using a layering technique based on fluorapatite glass ceramic. The MG and MD values were then determined using the micro-CT technique both before and after cementation.
Measurement of the MG and MD values
The MG and MD values of five teeth from each group were determined from two sections (sagittal and coronal) for four different regions (sagittal buccal, sagittal lingual, coronal mesial and coronal distal). The sections were opened in the CTAn program (Skyscan 1172, Kontich, Belgium) for the evaluation of MG and MD values.
The sagittal and coronal sections were evaluated. The points where the preparation of the crown started to be visible, and then the end, were determined. The sections between these two points were calculated for the MG and MD values. The measurements were obtained in millimeters from each surface of the tooth - buccal and lingual surfaces in the sagittal section and mesial and distal surfaces in the coronal section - at 40 different points to obtain 80 MG and MD values. Files were processed using NRecon (Version 1.6.6.0, Skyscan, Kontich, Belgium) and CTAn software [Figure 3]. Thereafter, 900 - 1000 sections of each specimen were reconstructed with the help of the NRecon program. The views were converted to a 2000 × 2000 pixel bitmap (BMP) format in the 8-bit gray-dynamic scale. The views of each section were opened and saved in Dataviewer 1.4.4 program for completion of the reconstruction.
Figure 3.
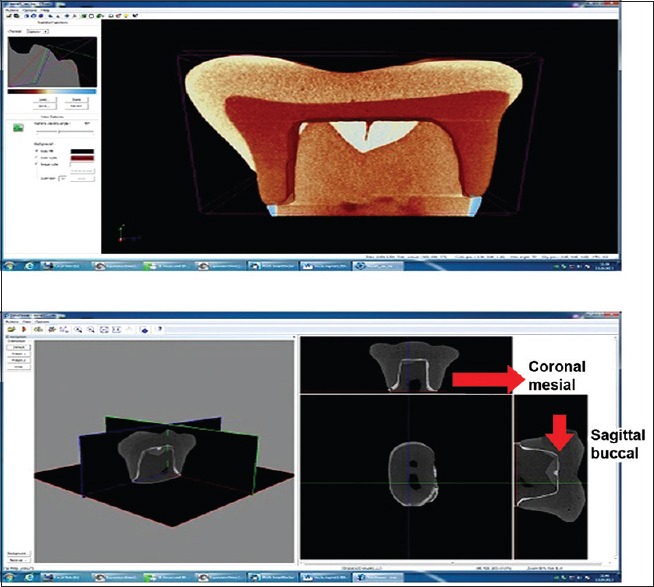
CTAn images of marginal gap and marginal discrepancy values by microcomputed tomography
After the initial measurements, the full ceramic crowns were cemented with the self-etch, self-cure resin cement (Multilink Automix) (Ivoclar Vivadent, Schaan, Liechtenstein) with finger pressure. Thereafter, the specimens were subjected to thermal cycling (5000 cycles, 5 - 55°C). The MG and MD values were determined again by the micro-CT technique in order to evaluate the changes effected by the cementation and the thermal cycling procedures. Results were statistically analyzed using one-way ANOVA, two-way ANOVA, Tukey HSD and paired t-tests (P = 0.05).
RESULTS
The MG and MD values of the three ceramic groups before cementation have been presented with measurement location and margin configuration, and are presented as mean ± SD in milimeters in Figures 4 and 5. Group 2B showed higher MG values (0.15 ± 0.07) than Group 2A (0.05 ± 0.02) on the buccal surface of the sagittal section. Group 1A showed higher MG values (0.14 ± 0.05) than Group 2A (0.05 ± 0.02) on the buccal surface of the sagittal section. Group A crowns showed higher MG values (0.79 ± 0.03) than Group C crowns (0.14 ± 0.06) on the mesial surface of the coronal section. Group 2B showed higher MD values (0.25 ± 0.11) than Group 1A (0.18 ± 0.04) on the lingual surface of sagittal section. The MD values of Group B on the lingual surface of the sagittal section (0.23 ± 0.85) and on the distal surface of the coronal section (0.21 ± 0.09) were higher than those on the mesial surface of the coronal section (0.18 ± 0.09). Therefore, the marginal fit before cementation was better on the mesial surface of the coronal section (P < 0.05) [Figure 4].
Figure 4.
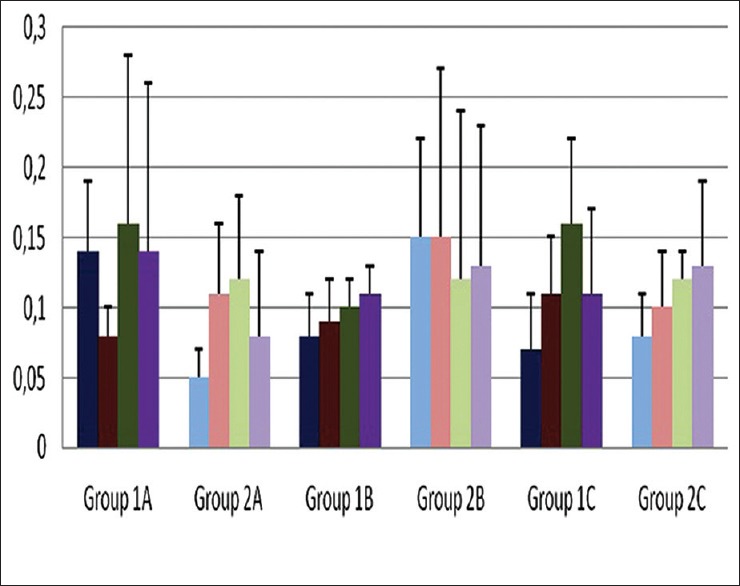
Mean and SD values of marginal gap values of full ceramics before cementation
Figure 5.
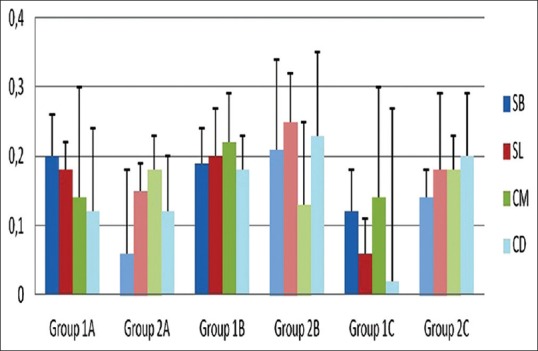
Mean and SD values of marginal discrepancy values of full ceramics before cementation
The MG and MD values of the ceramic groups after cementation have been presented along with measurement location and finish line configuration, and are presented as mean ± SD in Figures 6 and 7. The MG values of Group 1B on the buccal surface of the sagittal section increased significantly after cementation (0.23 ± 0.14). The MG values of Group 1A (0.32 ± 0.11) and Group 2C (0.31 ± 0.15) on the lingual surface of the sagittal section (0.34 ± 0.13) and on the mesial surface of the coronal section (0.30 ± 0.15) increased significantly after cementation. The MG values on the distal surface of the coronal section for Groups 1C (0.23 ± 0.08) and 2A (0.24 ± 0.11) also increased significantly. Group B showed higher MD mean values than Group A on the lingual surface of the sagittal section after cementation. The MD values on the buccal surface of the sagittal section of Group 1B (0.32 ± 0.10) and Group 2C (0.29 ± 0.08) also increased significantly after cementation. The MD values on the lingual surface of the sagittal section for Groups 1A (0.24 ± 0.07) and 2A (0.18 ± 0.13) exhibited a significant increase following cementation. The MD values of Group 1A (0.26 ± 0.06) and Group 2C (0.38 ± 0.18) on the mesial surface of the coronal section also increased after cementation. Except for the MG values for the shoulder preparation design on the buccal surface of the sagittal section and the MD values for chamfer preparation design on the lingual surface of the sagittal section, the MG and MD mean values significantly increased for all ceramics after cementation [Figures 6 and 7].
Figure 6.
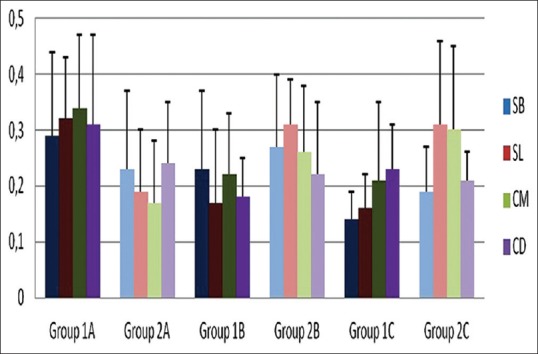
Mean and SD values of marginal gap values of full ceramics after cementation
Figure 7.
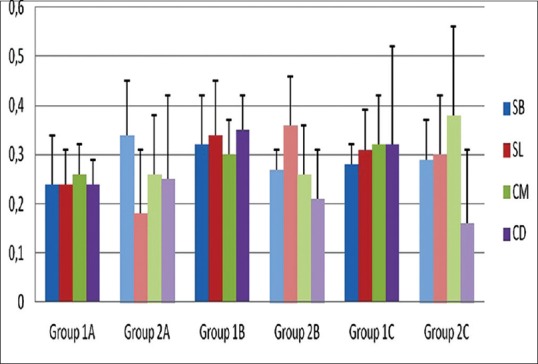
Mean and SD values of marginal discrepancy values of full ceramics after cementation
We tried to prepare a table with statistical differences lettering; however, it was not clear and understandable. It was more complex than graphics by lettering.
DISCUSSION
The results of this study support the rejection of part of the null hypothesis that there is no difference in the MG and MD in different regions of the teeth for shoulder and chamfer finish line designs, both before and after the procedures of cementation and thermal cycling. Except for two measurement locations, the mean values of MG and MD increased significantly for all ceramics after cementation. There were significant or insignificant differences in the MG and MD values between the various measurement locations and also between the two preparation designs of the ceramic crowns. Significant differences emerged in the comparison of the MG and MD between shoulders and chamfer finish line designs of the feldspathic ceramic system and chamfer finish line design of the Cerec in Lab aluminum oxide ceramic system.
Evaluation of the marginal fit on the midproximal surfaces of the crown/abutment junction is critical in the evaluation of marginal fit of a crown system, because the accessibility for maintenance of oral hygiene is decreased in these regions compared with the buccal and lingual surfaces. However, in most studies, the midproximal surfaces of the crown/abutment junction could not be evaluated by the routine marginal fit measurement methods. The current study has the advantage of the MG and MD values of mesial and distal surfaces of the coronal section being measured by the novel micro-CT technique. There are only a few studies that use this methodology for this purpose in the field of dentistry.[18,19,20] Micro-CT is a non-destructive, reliable and innovative method of analysis that allows high-resolution investigation of both the internal and the MG between tooth preparation and the restoration. It allows 2D and 3D measurements to be performed from any angle or position. Therefore, in the present study, the marginal fit could be evaluated in both the x- and y-axes, providing a more realistic perception of the MGs.
Nevertheless, comparison with previously conducted research is difficult as different methods of measurement were employed. Borba et al.[20] and Pelekanos et al.[19] applied the micro-CT technique to evaluate the fit of ceramic crowns and suggested that this method can be recommended as a useful tool for the evaluation of marginal and internal fit of dental restorations. The authors of the present study corroborate this recommendation.
In two recent studies of Borba et al.,[20,21] the marginal and internal fit of zirconia-based all-ceramic three unit fixed partial dentures (FPD) produced by the Cerec inLab CAD/CAM system were evaluated using the micro-CT technology. Different levels of adaptation were observed within the FPD at the different measuring points. Pelekanos et al.[19] found that the slip-cast technique and the Wol-Ceram system were the methods that presented the best MG values of 22 and 35 μm, respectively. The mean MD values of the slip-cast copings and Cerec inLab copings were 60.09 and 187.64 μm, respectively, in accordance with the current study's MD values of 60 - 200 μm for the same ceramic groups. In the present study, the Cerec inLab feldspathic ceramic system with chamfer finish line design (on the buccal surface of sagittal section) and the Cerec inLab feldspathic ceramic system with shoulder finish line design (on the lingual surface of sagittal section) presented the best results for MG, with values of 50 and 80 μm, respectively, before cementation. Lithium disilicate press ceramic system with shoulder finish line design (on the distal surface of coronal section) and Cerec inLab feldspathic ceramic system with chamfer finish line design (on the buccal surface of sagittal section) also presented the best results for MD, with values of 20 and 60 μm, respectively, before cementation. The difference in results may be due to the usage of the Cerec inLab technique and also the use of different measuring instruments. Difference in sample size and the number of measurements obtained per specimen may also have contributed to the variation. The slip cast technique is not machine dependent and MG values are indicative of the technician's ability, whereas for Cerec inLab, MG is indicative of the ability of the system.
In the study by Krasanaki et al.,[22] the influence of two different preparation types on the marginal fit of CAD/CAM alumina copings was evaluated. Copings were scanned using micro-CT and no correlation was found between copings and preparation type, in contrast with the present study in which chamfer finish line designs of aluminum oxide ceramic system showed better marginal fit as compared with shoulder finish line designs of the feldspathic ceramic system.
There have been many studies in which different methods have been used to evaluate the internal and MGs. Sulaiman et al.[23] and Grey et al.[24] determined the MGs of conventional InCeram crowns using the silicone paste technique to be 160.66 and 123 μm, respectively. These results were in accordance with the study by Yeo et al.[25]
A study by Rinke et al.[26] on the marginal fit of different all-ceramic crowns showed an overall variation ranging from 18 to 145 μm before cementation.[27] In the present study, the mean values of MG showed variation ranging from 50 to 160 μm before cementation and 140 to 340 μm after cementation. The mean values of MD in the current study showed variation ranging between 20 and 250 μm before cementation and 160 and 360 μm after cementation.
Bindl et al.[27] reported favorable results for crown restorations milled with the Cerec-2 system. They obtained mean MGs of 59.9 μm with Vita Mark II and 73.4 μm with Vita In-Ceram Alumina, with the difference between both values reaching statistical significance. In the study of Bindl et al.;[27] the results were clearly less favorable both with Vita Mark II (142.3 μm) and with Vita In-Ceram Alumina (98.1 μm). In the present study, the Cerec inLab feldspathic ceramic system (Vitablocs Mark II) generally presented the lowest variance when compared with the other ceramics, except for the MG values on the mesial surface of the coronal section. This result can be correlated with the manufacturing technique of the ceramic. When this ceramic system is used, restorations can be milled directly to their final dimensions. This factor may contribute to better marginal fit compared with other full-ceramic systems. In the current study, the lowest mean MG values for the Cerec inLab aluminum oxide ceramic system (Vita In-Ceram 2000 AL) before and after cementation were 80 and 180 μm, respectively, which are higher than the values found in an earlier study[28] for In-Ceram Alumina copings (57/117 μm). This result may be related to the technique and the coping-ceramic difference. In a recent study,[29] the MD values of In-Ceram all-ceramic crowns were reported to be 81.43 μm before cementation and 122.92 μm after cementation, which are lower than the lowest values of Vita In-Ceram AL ceramics in the current study (130 μm before cementation and 210 μm after cementation). The MD values of the IPS e.Max Press ceramics were found to be 95.65 μm before cementation and 137.97 μm after cementation, which are in accordance with the lowest values of the present study (60 μm before cementation and 160 μm after cementation).[29] In the current study, the mean MG for IPS e.Max ceramics ranged from 70 to 160 μm, which is in agreement with earlier studies.
The maximum value of MG for good clinical prognosis was determined to be 200 μm by Bjorn et al.[30] As per this standard, the results of the current study are within clinically acceptable limits. Values proposed in the literature for maximally acceptable marginal discrepancies for dental restorations vary from 50 to 120 μm.[7,31] The MD range of the present study is higher when compared with these studies, ranging from 120 to 250 μm. This can be attributed to the differences in the manufacturing technique as well as the measurement methods.
The results obtained in the current study show that there were statistically significant differences in the MG between the two finish line groups (shoulder and chamfer). In some studies, no significant difference was found between the MD values of the ceramics with shoulder and chamfer finish line designs.[11,28,32] In a recent study,[33] the average MG recorded for the chamfer design was 94 and 91 μm. In another study, MGs were greater for the chamfer finish line than for the shoulder.[34] Souza et al.[35] found that rounded shoulder preparation design showed significantly lower MD values than chamfer finish line design for full ceramics.[35] In contrast, zirconia crown copings with shoulder preparation design exhibited higher discrepancies than zirconia crowns with chamfer preparation design combined with 15° taper angle in another study.[36] In the current study, the Cerec inLab feldspathic ceramic system with chamfer finish line design showed better marginal fit than shoulder finish line design of the same ceramic on the buccal surface of the sagittal section and the Cerec inLab aluminum oxide ceramic system with chamfer preparation design showed higher MD values than the Cerec in Lab feldspathic ceramic system with shoulder finish line design on the lingual surface of the sagittal section before cementation.
In the present study, MD exhibited statistically significant differences between the buccolingual and mesiodistal aspects, similar to another study in which the facial and lingual margins exhibited significantly larger MD values than the mesial and distal margins.[23] However, other authors have not found significant differences between surfaces in their studies.[37]
As has been reported in previous studies,[37] MD in this study also increased markedly after cementation, even for the Cerec inLab feldspathic ceramic system. The three different ceramic systems demonstrated noticeable differences with respect to the MD values before and after cementation. Likewise, the three ceramic systems tested were fabricated through different laboratory procedures. Manufacturing of lithium disilicate press ceramic system copings involved the use of die spacers (Aqua Fit, Renfert GbmH, Hilzingen, Germany), whereas the Cerec inLab feldspathic ceramic system and the Cerec inLab aluminum oxide ceramic core structures were fabricated with a pre-determined internal relief of 30 μm and fabricated from CAD/CAM ingots. The preparation design and dimensions of the restorations may have affected the initial marginal fit and flowing off of luting material during the cementation process. As pressable ceramics are fabricated on gypsum casts using the lost wax technique, any form changes inherent in the processed materials might also affect the adaptation of the final restoration. Furthermore, wax patterns can exhibit significant shrinkage contraction that might result in additional discrepancies.
Krejci et al.[38] found that the type of margin did not influence the marginal adaptation after cementation. In our study, MG and MD values of the ceramics generally increased significantly after cementation, as has been reported in other studies,[28,39,40,41,42] and MD increased significantly after cementation in all of the groups analyzed. This finding may be explained by the difference in the clinicians’ cementation technique.
CONCLUSION
The MG and MD values of the full ceramics increased significantly after cementation, with exceptions of the MG values on the buccal surface of the sagittal section for shoulder preparation design and the MD values on the lingual surface of the sagittal section for chamfer preparation design of full-ceramic crowns.
Full-ceramic crowns showed clinically acceptable marginal adaptation values. The Feldspathic Cerec inLab ceramic system (Vitablocs Mark II) generally presented the lowest variance when compared with the other ceramics, except for the MG values on the mesial surface of the coronal section.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Boening KW, Wolf BH, Schmidt AE, Kästner K, Walter MH. Clinical fit of Procera AllCeram crowns. J Prosthet Dent. 2000;84:419–24. doi: 10.1067/mpr.2000.109125. [DOI] [PubMed] [Google Scholar]
- 2.Della Bona A, Kelly JR. The clinical success of all-ceramic restorations. J Am Dent Assoc. 2008;139(Suppl):8–13S. doi: 10.14219/jada.archive.2008.0361. [DOI] [PubMed] [Google Scholar]
- 3.Jacobs MS, Windeler AS. An investigation of dental luting cement solubility as a function of the marginal gap. J Prosthet Dent. 1991;65:436–42. doi: 10.1016/0022-3913(91)90239-s. [DOI] [PubMed] [Google Scholar]
- 4.Bergenholtz G, Cox CF, Loesche WJ, Syed SA. Bacterial leakage around dental restorations: Its effect on the dental pulp. J Oral Pathol. 1982;11:439–50. doi: 10.1111/j.1600-0714.1982.tb00188.x. [DOI] [PubMed] [Google Scholar]
- 5.Valderhaug J, Heloe LA. Oral hygiene in a group of supervised patients with fixed prostheses. J Periodontol. 1977;48:221–4. doi: 10.1902/jop.1977.48.4.221. [DOI] [PubMed] [Google Scholar]
- 6.Coli P, Karlsson S. Fit of a new pressure-sintered zirconium dioxide coping. Int J Prosthodont. 2004;17:59–64. [PubMed] [Google Scholar]
- 7.Suárez MJ, González de Villaumbrosia P, Pradíes G, Lozano JF. Comparison of the marginal fit of Procera AllCeram crowns with two finish lines. Int J Prosthodont. 2003;16:229–32. [PubMed] [Google Scholar]
- 8.Tan PL, Gratton DG, Diaz-Arnold AM, Holmes DC. An in vitro comparison of vertical margins gaps of CAD/CAM titanium and conventional cast restorations. J Prosthodont. 2008;17:378–83. doi: 10.1111/j.1532-849X.2008.00302.x. [DOI] [PubMed] [Google Scholar]
- 9.Att W, Komine F, Gerds T, Strub JR. Marginal adaptation of three different zirconium dioxide three-unit fixed dental prostheses. J Prosthet Dent. 2009;101:239–47. doi: 10.1016/S0022-3913(09)60047-0. [DOI] [PubMed] [Google Scholar]
- 10.Vigolo P, Fonzi F. An in vitro evaluation of fit of zirconium-oxide based ceramic four-unit fixed partial dentures, generated with three different CAD/CAM systems, before and after porcelain firing cycles and after glaze cycles. J Prosthodont. 2008;17:621–6. doi: 10.1111/j.1532-849X.2008.00366.x. [DOI] [PubMed] [Google Scholar]
- 11.Komine F, Iwai T, Kobayashi K, Matsumura H. Marginal and internal adaptation of zirconium dioxide ceramic copings and crowns with different finish line design. Dent Mater J. 2007;26:659–64. doi: 10.4012/dmj.26.659. [DOI] [PubMed] [Google Scholar]
- 12.Akbar JH, Petrie CS, Walker MP, Williams K, Eick JD. Marginal adaptation of Cerec 3 CAD/CAM composite crowns using two different finish line preparation designs. J Prosthodont. 2006;15:155–63. doi: 10.1111/j.1532-849X.2006.00095.x. [DOI] [PubMed] [Google Scholar]
- 13.Holmes JR, Bayne SC, Holland GA, Sulik WD. Considerations in measurement of marginal fit. J Prosthet Dent. 1989;62:405–8. doi: 10.1016/0022-3913(89)90170-4. [DOI] [PubMed] [Google Scholar]
- 14.Felton DA, Kanoy BE, Bayne SC, Wirthman GP. Effect of in vivo crown margin discrepancies on periodontal health. J Prosthet Dent. 1991;65:357–64. doi: 10.1016/0022-3913(91)90225-l. [DOI] [PubMed] [Google Scholar]
- 15.Tuntiprawon M, Wilson PR. The effect of cement thickness on the fracture strength of all-ceramic crowns. Aust Dent J. 1995;40:17–21. doi: 10.1111/j.1834-7819.1995.tb05607.x. [DOI] [PubMed] [Google Scholar]
- 16.Beuer F, Naumann M, Gernet W, Sorensen JA. Precision of fit: Zirconia three-unit fixed dental prostheses. Clin Oral Investig. 2009;13:343–9. doi: 10.1007/s00784-008-0224-6. [DOI] [PubMed] [Google Scholar]
- 17.Beuer F, Aggstaller H, Edelhoff D, Gernet W, Sorensen J. Marginal and internal fits of fixed dental prostheses zirconia retainers. Dent Mater. 2009;25:94–102. doi: 10.1016/j.dental.2008.04.018. [DOI] [PubMed] [Google Scholar]
- 18.Seo D, Yi Y, Roh B. The effect of preparation designs on the marginal and internal gaps in Cerec3 partial ceramic crowns. J Dent. 2009;37:374–82. doi: 10.1016/j.jdent.2009.01.008. [DOI] [PubMed] [Google Scholar]
- 19.Pelekanos S, Koumanou M, Koutayas SO, Zinelis S, Eliades G. Micro-CT evaluation of the marginal fit of different In-Ceram alumina copings. Eur J Esthet Dent. 2009;4:278–92. [PubMed] [Google Scholar]
- 20.Borba M, Cesar PF, Griggs JA, Della Bona Á. Adaptation of all-ceramic fixed partial dentures. Dent Mater. 2011;27:1119–26. doi: 10.1016/j.dental.2011.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Borba M, Miranda WG, Jr, Cesar PF, Griggs JA, Bona AD. Evaluation of the adaptation of zirconia-based fixed partial dentures using Micro-CT technology. Braz Oral Res. 2013;27:396–402. doi: 10.1590/S1806-83242013000500003. [DOI] [PubMed] [Google Scholar]
- 22.Krasanaki ME, Pelekanos S, Andreiotelli M, Koutayas SO, Eliades G. X-ray microtomographic evalution of the influence of two preparation types on the marginal fit of CAD/CAM alumina copings: A pilot study. Int J Prosthodont. 2012;25:170–2. [PubMed] [Google Scholar]
- 23.Sulaiman F, Chai J, Jameson LM, Wozniak WT. A comparison of marginal fit of In-Ceram, IPS Empress, and Procera crowns. Int J Prosthodont. 1997;10:478–84. [PubMed] [Google Scholar]
- 24.Grey NJ, Piddock V, Wilson MA. In vitro cornparison of conventional crowns and a new all-ceramic system. J Dent. 1993;21:47–51. doi: 10.1016/0300-5712(93)90051-q. [DOI] [PubMed] [Google Scholar]
- 25.Yeo IS, Yang JH, Lee JB. In vitro marginal fit of three all-ceramic crown systems. J Prosthet Dent. 2003;9:459–64. doi: 10.1016/j.prosdent.2003.08.005. [DOI] [PubMed] [Google Scholar]
- 26.Rinke S, Hüls A, Jahn L. Marginal accuracy and fracture strength of conventional and copy-milled all-ceramic crowns. Int J Prosthodont. 1995;8:303–10. [PubMed] [Google Scholar]
- 27.Bindl A, Mörmann WH. Marginal and internal fit of all-ceramic CAD/CAM crown-copings on chamfer preparations. J Oral Rehabil. 2005;32:441–7. doi: 10.1111/j.1365-2842.2005.01446.x. [DOI] [PubMed] [Google Scholar]
- 28.Quintas AF, Oliveira F, Bottino MA. Vertical marginal discrepancy of ceramic copings with different ceramic materials, finish lines, and luting agents: An in vitro evaluation. J Prosthet Dent. 2004;92:250–7. doi: 10.1016/j.prosdent.2004.06.023. [DOI] [PubMed] [Google Scholar]
- 29.Borges GA, Faria JS, Agarwal P, Spohr AM, Correr-Sobrinho L, Miranzi BA. In vitro marginal fit of three all-ceramic crown systems before and after cementation. Oper Dent. 2012;37:641–9. doi: 10.2341/11-012-L. [DOI] [PubMed] [Google Scholar]
- 30.Björn AL, Björn H, Grkovic B. Marginal fit of restorations and its relation to periodontal bone level. II. Crowns. Odontolo Revy. 1970;21:337–46. [PubMed] [Google Scholar]
- 31.Boening KW, Wolf BH, Schmidt AE, Kästner K, Walter MH. Clinical fit of Procera AllCeram crowns. J Prosthet Dent. 2000;84:419–24. doi: 10.1067/mpr.2000.109125. [DOI] [PubMed] [Google Scholar]
- 32.Akbar JH, Petrie CS, Walker MP, Williams K, Eick JD. Marginal adaptation of Cerec 3 CAD\CAM composite crowns using two different finish line preparation designs. J Prosthodont. 2006;15:155–63. doi: 10.1111/j.1532-849X.2006.00095.x. [DOI] [PubMed] [Google Scholar]
- 33.Tsitrou EA, Northeast AE, van Noort. Evaluation of the marginal fit of three margin designs of resin composite crowns using CAD\CAM. J Dent. 2007;35:68–73. doi: 10.1016/j.jdent.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 34.Cho L, Choi J, Yi YJ, Park CJ. Effect of finish line variants on marginal accuracy and fracture strength of ceramic optimized polymer\fiber-reinforced composite crowns. J Prosthet Dent. 2004;91:554–60. doi: 10.1016/j.prosdent.2004.03.004. [DOI] [PubMed] [Google Scholar]
- 35.Souzo RO, Özcan M, Pavanelli CA, Buso L, Lombardo GH, Michida SM, et al. Mesquita ve ark Marginal and internal discrepancies related to margin design of ceramic crowns fabricated by a CAD\CAM system. J Prosthodont. 2012;21:94–100. doi: 10.1111/j.1532-849X.2011.00793.x. [DOI] [PubMed] [Google Scholar]
- 36.Castillo Oyagüe R, Sánchez-Jorge MI, Sánchez Turrión A. Influence of CAD\CAM scanning method and tooth-preparation design on vertical misfit of zirconia crown copings. Am J Dent. 2010;23:341–6. [PubMed] [Google Scholar]
- 37.Gonzalo E, Suárez MJ, Serrano B, Lozzano JF. A comparison of the marginal vertical discrepancies of zirconium and metal ceramic posterior fixed dental prostheses before and after cementation. J Prosthet Dent. 2009;102:378–84. doi: 10.1016/S0022-3913(09)60198-0. [DOI] [PubMed] [Google Scholar]
- 38.Krejci I, Lutz F, Reimer M. Marginal adaptation and fit of adhesive ceramic inlays. J Dent. 1993;21:39–46. doi: 10.1016/0300-5712(93)90048-u. [DOI] [PubMed] [Google Scholar]
- 39.Wolfart S, Wegner SM, Al-Halabi A, Kern M. Clinical evaluation of marginal fit of a new experimental all-ceramic system before and after cementation. Int J Prosthodont. 2003;16:587–92. [PubMed] [Google Scholar]
- 40.Pera P, Gilodi S, Bassi F, Carossa S. In vitro marginal adaptation of alumina porcelain ceramic crowns. J Prosthet Dent. 1994;72:585–90. doi: 10.1016/0022-3913(94)90289-5. [DOI] [PubMed] [Google Scholar]
- 41.Beschindt SM, Strub JR. Evaluation of the marginal accuracy of different all-ceramic crown systems after simulation in the artificial mouth. J Oral Rehabil. 1999;26:582–93. doi: 10.1046/j.1365-2842.1999.00449.x. [DOI] [PubMed] [Google Scholar]
- 42.Kern M, Schaller HG, Strub JR. Marginal fit of restorations before and after cementation in vivo. Int J Prosthodont. 1993;6:585–91. [PubMed] [Google Scholar]