

Abstract
The aim of this clinical case series is to present a diagnosis and different treatment methods of patients in different ages with amelogenesis imperfecta (AI) as well as further treatments during a 3-6 years follow-up period. A number of 31 patients (16 female, 15 male with a mean age of 10.77 ± 2.65 years) with AI have been examined for the study group between 2007 and 2010 years. A detailed anamnesis was recorded, followed by a clinical and radiological assessment of oral health. The types of AI classified for each patient according to clinical and radiographic evaluation. The main complaints of patients, presence of dental caries and dental anomalies were noted. Necessary treatments had been planned for the individual cases of AI. A number of 19 patients had hypoplastic (HP) form, and 10 patients showed hypomaturation (HM) form of AI, while one patient showed hypocalcified form of AI and one patient had HM-HP form with taurodontism. Main complaints were chiefly related to dissatisfactory esthetics and dental sensitivity. Caries prevalence index was 93.5%. Mean decayed, missing, filling permanent teeth (DMF) and DMF surface (DMFS) were found as 2.74 ± 1.71 and 6.23 ± 3.99; df (decayed, filling primary teeth) and dfs (decayed, filling primary teeth surface) were found as 3.12 ± 2.85 and 5.24 ± 4.97, respectively. All patients received individual clinical care, including preventive, restorative, and prosthetic treatments. Patients have scheduled for regular follow-up in every 3 months. Composite restorations were used as the most common treatment (25 patients, 80.6%). The treatment plan should be based on patient's age, type of defects and individual needs of the patients. Necessary treatment plan is essential, not only due to functional and aesthetic reasons, but also for the positive psychological impact on young patients.
Keywords: Amelogenesis imperfecta, management, treatment
INTRODUCTION
Amelogenesis imperfecta (AI) is a group of hereditary conditions that primarily affect the quality and/or the quantity of dental enamel, with a variable occurrence of approximately 1/700-1/14,000.[1,2,3,4,5,6] Currently, mutations in six genes are known to have causal roles in the genetic etiology of AI: Amelogenin, enamelin, enamelysin, kallikrein-4, distal less and family with sequence similarity 83.[1,6,7,8,9]
Various classification systems proposed for the different AI types are based on genetic heritance, histopathology, and specific clinical dental characteristics.[1,2,10,11,12] Witkop's classification is the most frequently cited one in the literature.[1] Four major categories based primarily on phenotype (hypoplastic [HP], hypomaturation [HM], hypocalcified [HC], HM-HP with taurodontism) subdivided into 15 subtypes based on clinical phenotype and mode of inheritance.[1,3,6] In general, the inheritance pattern is usually autosomal dominant or recessive, or X linked. Within affected families, there is an extremely variable clinical appearance of enamel hypoplasia, hypocalcification, or HM, depending on which stages of enamel formation are involved.[2]
Amelogenesis imperfecta has been associated with different dental anomalies including discolored teeth, microdontia, congenitally missing teeth, taurodontism, pulpal calcification, hypercementosis, crown and root resorption.[2,13,14,15,16,17,18,19] In addition, AI was shown to be associated with malocclusions such as open bite and cross bite.[19,20,21] Anterior open bite is the result of defects in the eruptive mechanism, secondary to the disturbances of the enamel epithelium. Other common causes of anterior open bite are tongue thrusting and thumb sucking habits seen in AI patients.[5] Singhal et al. and Rowley et al. stated that the incidence of open bite in patients with AI varies from 24% to 60%, respectively.[5,20]
Children with AI experience many oral difficulties. In certain forms of AI; an increased incidence of carries, delayed tooth eruption, or even teeth retention are reported.[18] Other clinical problems regardless of subtype, are unsatisfactory aesthetics, thermal sensitivity of teeth and loss of occlusal vertical dimension.[2,22] As the detective enamel is very thin or even completely absent, the yellowish or brown dentin of the crown is revealed, and the teeth are very sensitive.[18,19] Apart from these difficulties, this condition also brings appearance-related psychological problem and lack of self-confidence due to the appearance of their teeth.[18] There are also other difficulties of managing AI including dental inexperience and anxiety of a child and parental expectation all of which further complicate its management.[19]
Amelogenesis imperfecta affects deciduous dentition as well as a permanent dentition and requires a specific preventive and restorative care approach.[19]
The currently available different materials and methods for restorative procedures have made it both exciting and confusing for dental practitioners. It has been reported adhesive restorative techniques, over-dentures, porcelain-fused-to-metal crowns, fixed partial dentures, full porcelain crowns, inlay/onlay restorations and lately zirconium crowns are mainly used for the prosthodontic treatment of AI patients.[2,18,19,22,23,24,25,26] An appropriate oral hygiene is essential as gingival inflammation and bleeding do not allow sufficient conservative and prosthodontic treatment.[2,18] However, the appropriate treatment plan should be individual and based on patient's need.
The aim of this clinical case series is to present a diagnosis and different treatment methods of patients in different ages with AI as well as further treatments during a 3-6 years follow-up period.
CASE REPORT
Subject screening
Amelogenesis imperfecta patients admitted to Istanbul University, Faculty of Dentistry, Department of Pedodontics, Turkiye for elimination of aesthetical, functional and psychosocial problems. This study was approved by the Ethics Committee of the Istanbul University, Cerrahpasa Medical Faculty, Turkiye (No: 83045809/14486) in accordance with the Declaration of Helsinki. A total of 31 patients (16 female, 15 male) between 6 and 18 years old (mean age of 10.77 ± 2.65 years) with AI have been examined between 2007 and 2010 years.
Detailed medical, dental, and family histories were obtained, followed by a detailed clinical and radiological assessment of the patients. All participants were examined and classified by one calibrated pediatric dentist (M.K) through use of Witkop's classification of AI.[1] Affected individuals were also evaluated clinically for the presence of skin, hair, fingernail and osseous abnormalities known to be a sign of any syndromic conditions that could be associated with AI. Nonsyndromic patients with AI were included in the study. Furthermore, initial dental photographs and panoramic radiographs were obtained from all participants.
The main complaints of patients were dissatisfaction with the appearances of their teeth, extreme dental sensitivity, presence of dental caries and other dental anomalies such as open bite and orthodontic problems. An individual preventive and therapeutic treatment protocol was planned with specialist dentists from other disciplines for all patients.
Clinical findings and treatment plan
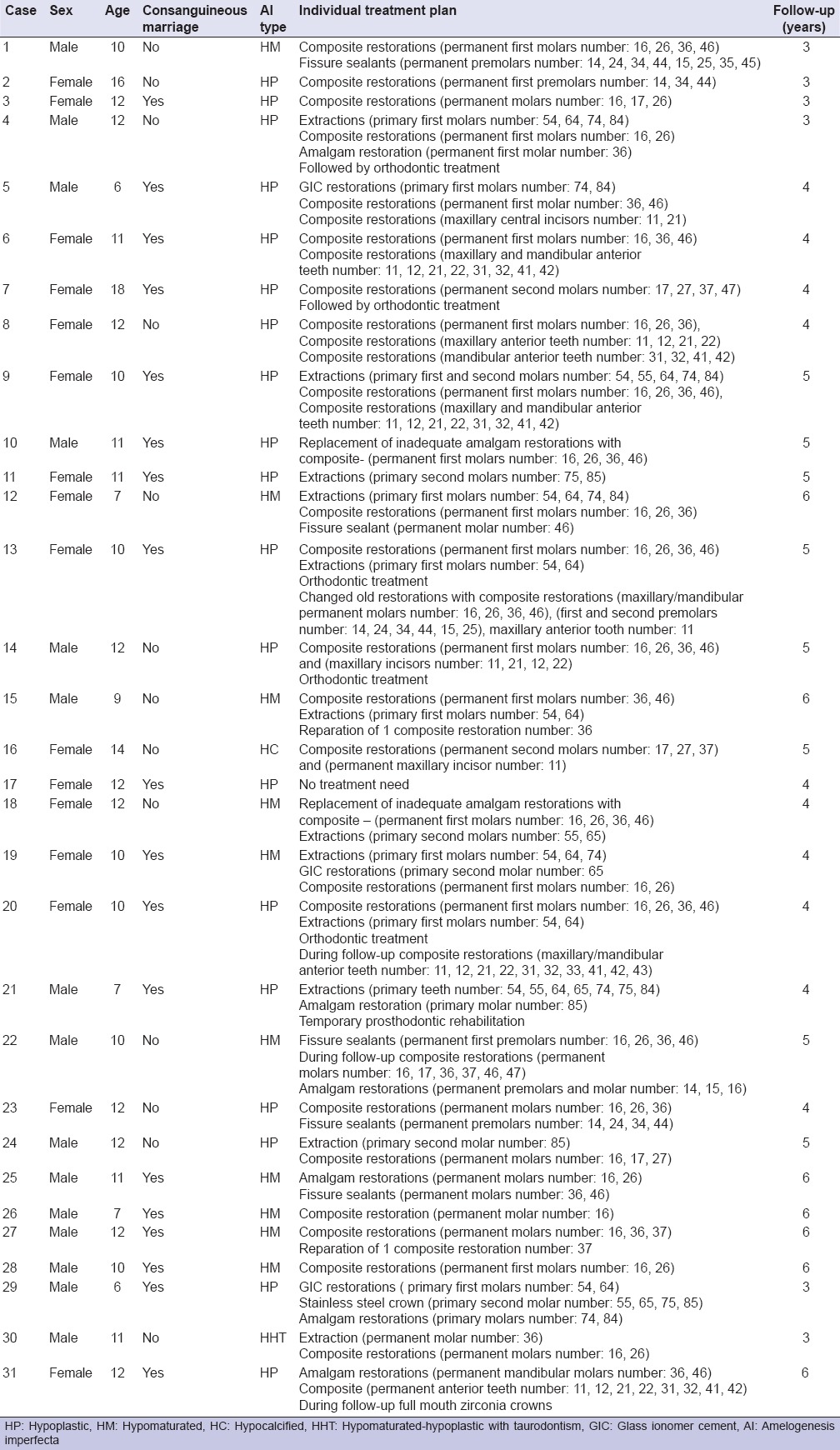
Descriptive data (age, gender, consanguineous marriage, types of AI) and treatment details (previous treatment history, initial treatment, follow-up period and treatment during follow-up) are summarized in Table 1. In 19 of patients HP form (61.2%) of AI was diagnosed, in 10 patients HM form (32.2%), in one patient HC form (3.2%) and in one patient AI combined with taurodontism (3.2%). Eighteen of the patients stated consanguineous marriages.
Table 1.
Distribution of dental anomalies in AI patients’ according to types
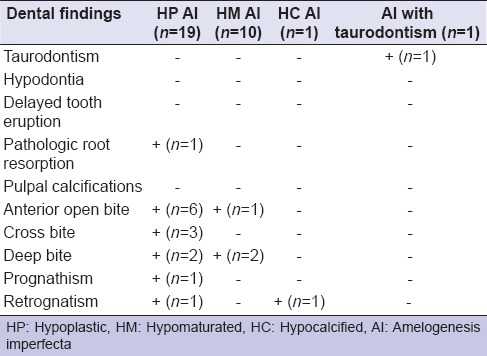
A number of 19 patients was diagnosed with HP form of AI (61.2%), 10 patients with HM form (32.2%), and 1 patient with HC form (3.2%) while one patient was diagnosed with AI combined with taurodontism (3.2%).
High caries prevalence was found, and caries prevalence index of the patients was 93.5%. Mean decayed, missing, filling permanent teeth (DMF) and decayed, missing, filling permanent teeth surface (DMFS) were found as 2.74 ± 1.71 and 6.23 ± 3.99; df (decayed, filling primary teeth) and dfs (decayed, filling primary teeth surface) were found as 3.12 ± 2.85 and 5.24 ± 4.97, respectively. Main complaints of the patients were chiefly related to dissatisfactory aesthetics and dental sensitivity.
Distribution of dental anomalies according to AI types is summarized in Table 1. Anterior open bite was found in seven patients (22.5%), (six HP type of AI and one HM type of AI). Crossbite (three HP type of AI) and deep bite (two HP and two HM type of AI) were also seen in some of the patients.
Following a complex examination and preparing a detailed treatment plan; first, all decayed teeth were restored with composite, glass ionomer cement (GIC) and amalgam materials [Figure 1]. Composite restorations were used as the most common treatment (25 patients, 80.6%); in six patient's amalgam restorations (19.3%) and in three patients (9.6%) GIC were preferred. Preventive treatment such as fissure sealants and topical fluoride gels were applied to some of the patients. According to indications, tooth extraction and following temporary prosthodontics rehabilitation were applied to achieve pain relief and provide satisfactory function and aesthetic. The definitive esthetic restorations were achieved by zirconia crowns or metal-ceramic crowns [Figure 2]. During follow-up periods, the patients who diagnosed with varying degrees of secondary caries and failure of restorations have been retreated with new restorations for better aesthetic appearance.
Figure 1.
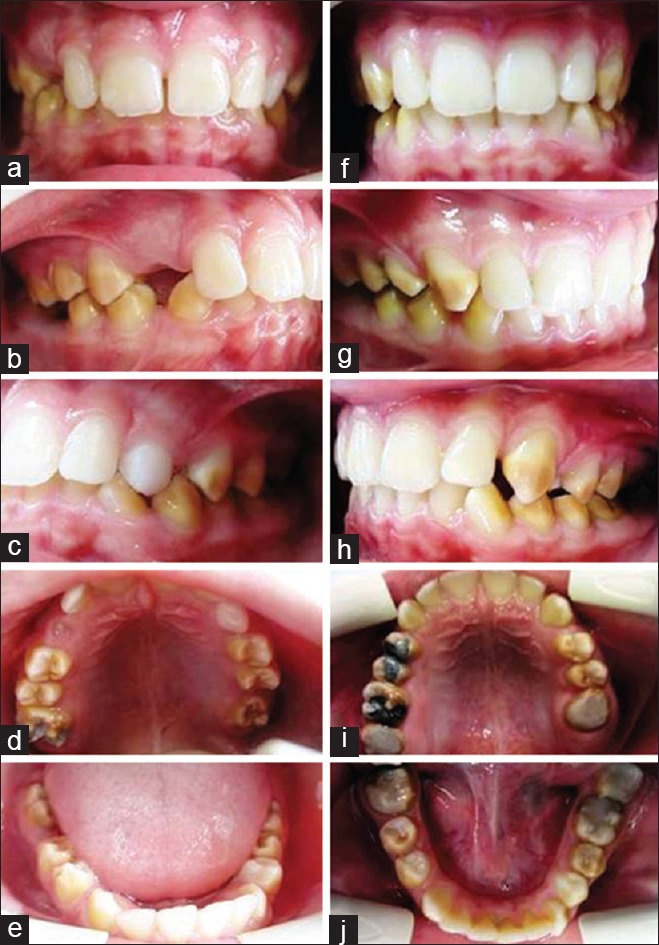
(a-e) Case 22 before and (f-j) after treatment
Figure 2.
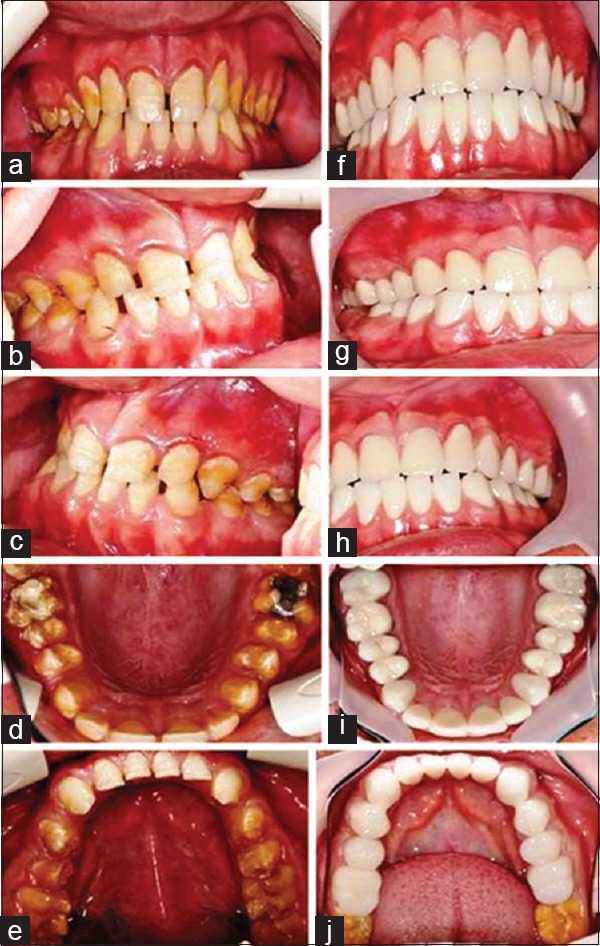
(a-e) Case 31 before and (f-j) after treatment
Regular follow-up periods carried out in every 3 months during 3-6 years. During the follow-up period, five patients have been referred to Orthodontic Department for their treatment [Figure 3]. Individual treatment procedures described in Table 2 for each patient's.
Figure 3.
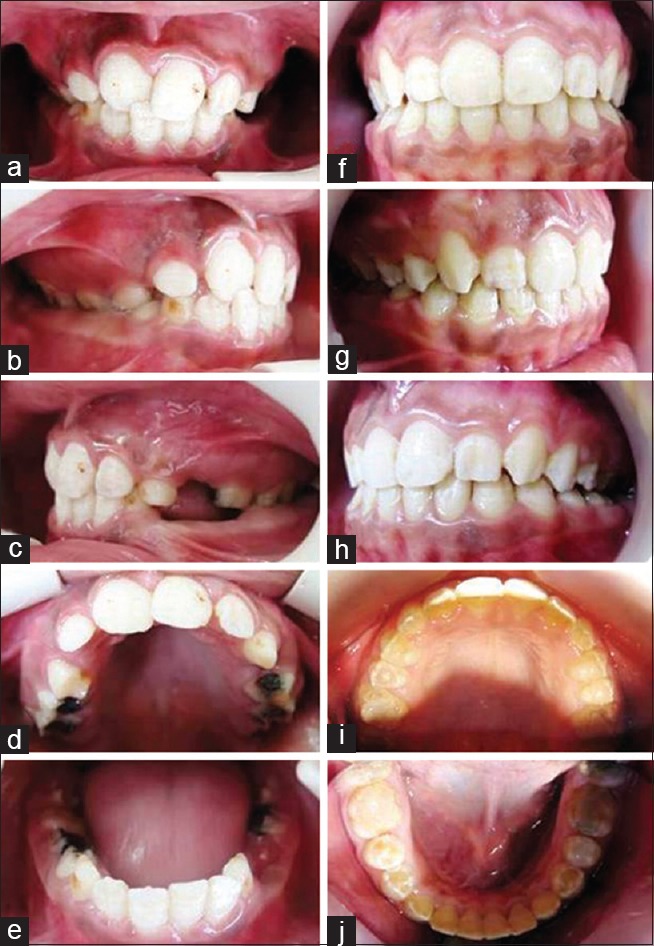
(a-e) Case 13 before and (f-j) after treatment
Table 2.
Clinical evaluation and oral rehabilitation of patients with AI
DISCUSSION
There have been several clinical reports describing restorative and esthetic treatment care in individual AI patients.[2,4,16,18,19,23,25] The most frequently described conditions are in association with delayed tooth eruption and changes in crown morphology.[18] Similarly, our patients have shown delayed tooth eruption and microdontia.
Dental treatment could be medically necessary and very important for possession of teeth and oral aesthetics for a normal psychosocial development. However, the restoration of aesthetics and function of teeth in childhood patients suffering from AI often present to the dentist a major challenge.[27] As with all children, initial experience with a dental profession plays a part in their cooperation in the future.[19]
Historically, patients with AI have been treated with extractions or with the construction of complete removable dentures.[22] These options are psychologically serious when the problem must be addressed to adolescent patients.[4,23,27] In this study, primary and permanent molar teeth were extracted because of infection and excessive loss of tooth structure in 11 patients.
Management directed at three aspects of treatment includes prevention, restoration and aesthetics. Preventive aspects in the primary and mixed dentition include dietary advice, fluoride supplements and oral hygiene instructions. Oral hygiene can be particularly difficult for these patients due to the sensitivity while brushing. The use of warm water for tooth brushing will go some way towards relieving symptoms while rinsing. Also, regular use of fluoride mouthwashes can help to reduce sensitivity and prevent caries.[19,22] Followed by oral hygiene instructions; fissure sealants and topical fluoride applications should be applied during the primary and permanent dentition in clinical follow-up term.[4,16,23,25,27] In this case series; because of the caries incidence, restorative treatments were applied more than preventive treatments. After restorative treatments, patients were received preventive treatments.
Restorative aspects in the primary dentition composite direct veneers for anterior teeth, GIC and stainless steel crowns for primary molars; in the mixed dentition stainless steel crowns, onlays for permanent molars, composite or GICs for primary and permanent teeth. For permanent incisors, direct or indirect composite veneers will improve aesthetics, reduce sensitivity and reduce incisal wear.[4,16,19,23,25,27] Good periodontal health and eruption process are important for long term success of restorative treatments. However, the margins of any restoration will become visible and additional treatment will be required at intervals.[19] In this study, initial restorative treatments were chosen conservative, using composite and GIC materials. Stainless steel crowns were needed in only one case.
The esthetic aspects in the primary dentition include giving minimal intervention GIC restorations, direct and indirect composite resin veneers in the mixed dentition and porcelain veneers, full crowns, over-dentures and complete dentures in the permanent dentition.[4,16,23,25,27] The fixed prosthodontic treatment selected, albeit invasive, is more conservative than other considered alternatives. Treatment methods involving extractions of excessive defected teeth, endodontic and restorative procedures, removable and over-denture prosthesis, implant supported fixes prosthesis are also considerable depending on patient's growth, age and needs.[23,28] In the present study, zirconia crowns were preferred in young adults for aesthetic and psychological rehabilitation.
In our case group, we found the prevalence of caries as 93.5%. DMF and DMFS were found as 2.74 ± 1.71 and 6.23 ± 3.99; df and dfs were found as 3.12 ± 2.85 and 5.24 ± 4.97. The individuals with AI had experienced many oral difficulties including sensitivity and aesthetics mostly caused by active dental caries. The main reason for high caries activity pretty much depends on the completeness of the enamel structure.[4] When we indicated any carious lesions present, we restored without any delay; when we indicated as poor prognosis that is deemed unrestorable we considered as the extraction. However, there is still no standard formula, current protocol or guideline for successful treatment. Initial treatment should be planned depending on AI type, severity and oral health habits of the patient.[5,24,25,26] Successful bonding of composite resins to teeth affected by AI type, how the enamel responds to acid etching.[4] High failure rates with adhesive restorations in patients with AI have been described, especially with HC AI.[7] In this type of AI, the enamel has a higher protein content, which might reduce the bonding of restorations. Although deproteinization in HC AI has been reported to enhance the bonding of composite restorations, the recent study concluded that the procedure of deproteinization had no significant effect on the success of the adhesive restorations.[29] In this case series, old restorations were changed for a better aesthetic appearance.
Although there are several clinical case reports related with treatment management of patients with AI, in our knowledge it is one of the largest single-center series published to date in the dental literature. Markovic et al. presented a case series of 12 AI patients (7 female, 5 male; mean aged 10.6 ± 4.6 years old).[4] In that case series, patients were instructed to maintain meticulous oral hygiene and a professional dental prophylaxis were periodically performed. Preventive treatments were modified as new materials for enamel remineralization. Posterior teeth were protected with GIC and fissure sealants. Direct composite resin restorations were used to improve the appearance anterior teeth. Metal-ceramic fixed partial dentures, and definitive direct composite resin restorations were applied by interdisciplinary approaches. Our treatment plans are similar to this case series.
Preventive applications and if necessary restorative treatments have been applied to children with AI in primary and mixed dentition. While GIC and amalgam restorations have been chosen for treatment of posterior teeth, composite restorations have been used for anterior teeth and posterior teeth with excessive loss. In the permanent dentition, to provide an aesthetic with orthodontic treatment and composite restorations in case of moderate tooth structure loss, composite restorations have been performed in terms of the esthetic approach. In cases with excessive tooth loss or missing tooth, prosthetic rehabilitation has been preferred as treatment approach.
CONCLUSIONS
Amelogenesis imperfecta is characterized by abnormal enamel formation associated with multiple anomalies and requires interdisciplinary long term treatment. The dentist has to diagnose the condition as early as possible to offer early intervention and ensure long term survival of the restorations. It is important to encourage the child and parents for complete oral rehabilitation. The treatment plan should be based on patient's age, type of defects and individuals needs of the patients. Necessary treatment plan is essential, not only due to functional and aesthetic reasons, but also for the positive psychological impact on young patients.
ACKNOWLEDGMENTS
We thank to families for their participation; Pelin Barlak, Tugce Tanyeri and Yelda Kasımoglu for patient's treatment. This investigation was supported by Scientific Research Projects Coordination Unit of Istanbul University. Project number: UDP-12561.
Footnotes
Source of Support: Scientific Research Projects Coordination Unit of Istanbul University. Project Number: UDP-12561.
Conflict of Interest: None declared
REFERENCES
- 1.Witkop CJ., Jr Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: Problems in classification. J Oral Pathol. 1988;17:547–53. doi: 10.1111/j.1600-0714.1988.tb01332.x. [DOI] [PubMed] [Google Scholar]
- 2.Yip HK, Smales RJ. Oral rehabilitation of young adults with amelogenesis imperfecta. Int J Prosthodont. 2003;16:345–9. [PubMed] [Google Scholar]
- 3.Rathi NV, Singh MG, Kumar M, Dahake PT, Thakur R, Ranjan MK. Oral rehabilitation of amelogenesis imperfect: A case report. Indian J Dent Sci. 2013;3:64–6. [Google Scholar]
- 4.Markovic D, Petrovic B, Peric T. Case series: Clinical findings and oral rehabilitation of patients with amelogenesis imperfecta. Eur Arch Paediatr Dent. 2010;11:201–8. doi: 10.1007/BF03262745. [DOI] [PubMed] [Google Scholar]
- 5.Singhal R, Pathak A, Goenka P. Amelogenesis imperfecta with anterior open bite: A rare case report. Int J Clin Paediatr Dent. 2011;4:245–7. doi: 10.5005/jp-journals-10005-1118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kwok-Tung L, King NM. The restorative management of amelogenesis imperfecta in the mixed dentition. J Clin Pediatr Dent. 2006;31:130–5. doi: 10.17796/jcpd.31.2.b575277016661476. [DOI] [PubMed] [Google Scholar]
- 7.Urzúa B, Ortega-Pinto A, Farias DA, Franco E, Morales-Bozo I, Moncada G, et al. A multidisciplinary approach for the diagnosis of hypocalcified amelogenesis imperfecta in two Chilean families. Acta Odontol Scand. 2012;70:7–14. doi: 10.3109/00016357.2011.574973. [DOI] [PubMed] [Google Scholar]
- 8.Hu JC, Chan HC, Simmer SG, Seymen F, Richardson AS, Hu Y, et al. Amelogenesis imperfecta in two families with defined AMELX deletions in ARHGAP6. PLoS One. 2012;7:e52052. doi: 10.1371/journal.pone.0052052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cho SH, Seymen F, Lee KE, Lee SK, Kweon YS, Kim KJ, et al. Novel FAM20A mutations in hypoplastic amelogenesis imperfecta. Hum Mutat. 2012;33:91–4. doi: 10.1002/humu.21621. [DOI] [PubMed] [Google Scholar]
- 10.Rao S, Witkop CJ., Jr Inherited defects in tooth structure. Birth Defects Orig Artic Ser. 1971;7:153–84. [PubMed] [Google Scholar]
- 11.Winter GB, Brook AH. Enamel hypoplasia and anomalies of the enamel. Dent Clin North Am. 1975;19:3–24. [PubMed] [Google Scholar]
- 12.Witkop CJ. Hereditary defects in enamel and dentin. Acta Genet Stat Med. 1957;7:236–9. doi: 10.1159/000150974. [DOI] [PubMed] [Google Scholar]
- 13.Aldred MJ, Crawford PJ. Variable expression in amelogenesis imperfecta with taurodontism. J Oral Pathol. 1988;17:327–33. doi: 10.1111/j.1600-0714.1988.tb01545.x. [DOI] [PubMed] [Google Scholar]
- 14.Collins MA, Mauriello SM, Tyndall DA, Wright JT. Dental anomalies associated with amelogenesis imperfecta: A radiographic assessment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:358–64. doi: 10.1016/s1079-2104(99)70043-0. [DOI] [PubMed] [Google Scholar]
- 15.Aldred MJ, Savarirayan R, Lamandé SR, Crawford PJ. Clinical and radiographic features of a family with autosomal dominant amelogenesis imperfecta with taurodontism. Oral Dis. 2002;8:62–8. doi: 10.1034/j.1601-0825.2002.1c766.x. [DOI] [PubMed] [Google Scholar]
- 16.Ayers KM, Drummond BK, Harding WJ, Salis SG, Liston PN. Amelogenesis imperfecta – multidisciplinary management from eruption to adulthood. Review and case report. N Z Dent J. 2004;100:101–4. [PubMed] [Google Scholar]
- 17.Korbmacher HM, Lemke R, Kahl-Nieke B. Progressive pre-eruptive crown resorption in autosomal recessive generalized hypoplastic amelogenesis imperfecta. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:540–4. doi: 10.1016/j.tripleo.2006.08.022. [DOI] [PubMed] [Google Scholar]
- 18.Suchancova B, Holly D, Janska M, Stebel J, Lysy J, Thurzo A, et al. Amelogenesis imperfecta and the treatment plan-interdisciplinary team approach. Bratisl Lek Listy. 2014;115:44–8. doi: 10.4149/bll_2014_010. [DOI] [PubMed] [Google Scholar]
- 19.McDonald S, Arkutu N, Malik K, Gadhia K, McKaig S. Managing the paediatric patient with amelogenesis imperfecta. Br Dent J. 2012;212:425–8. doi: 10.1038/sj.bdj.2012.366. [DOI] [PubMed] [Google Scholar]
- 20.Rowley R, Hill FJ, Winter GB. An investigation of the association between anterior open-bite and amelogenesis imperfecta. Am J Orthod. 1982;81:229–35. doi: 10.1016/0002-9416(82)90055-0. [DOI] [PubMed] [Google Scholar]
- 21.Bäckman B, Adolfsson U. Craniofacial structure related to inheritance pattern in amelogenesis imperfecta. Am J Orthod Dentofacial Orthop. 1994;105:575–82. doi: 10.1016/S0889-5406(94)70142-3. [DOI] [PubMed] [Google Scholar]
- 22.Kamble VD, Parkhedkar RD. Multidisciplinary approach for restoring function and esthetics in a patient with amelogenesis imperfecta: A clinical report. J Clin Diagn Res. 2013;7:3083–5. doi: 10.7860/JCDR/2013/6665.3860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gokce K, Canpolat C, Ozel E. Restoring function and esthetics in a patient with amelogenesis imperfecta: A case report. J Contemp Dent Pract. 2007;8:95–101. [PubMed] [Google Scholar]
- 24.Claman L, Alfaro MA, Mercado A. An interdisciplinary approach for improved esthetic results in the anterior maxilla. J Prosthet Dent. 2003;89:1–5. doi: 10.1067/mpr.2003.5. [DOI] [PubMed] [Google Scholar]
- 25.Ozturk N, Sari Z, Ozturk B. An interdisciplinary approach for restoring function and esthetics in a patient with amelogenesis imperfecta and malocclusion: A clinical report. J Prosthet Dent. 2004;92:112–5. doi: 10.1016/S0022391304002288. [DOI] [PubMed] [Google Scholar]
- 26.Poulsen S, Gjørup H, Haubek D, Haukali G, Hintze H, Løvschall H, et al. Amelogenesis imperfecta-a systematic literature review of associated dental and oro-facial abnormalities and their impact on patients. Acta Odontol Scand. 2008;66:193–9. doi: 10.1080/00016350802192071. [DOI] [PubMed] [Google Scholar]
- 27.Neto NL, Paschoal MA, Kobayashi TY, Rios D, Silva SM. Early oral rehabilitation of a child with amelogenesis imperfecta. J Health Sci Inst. 2010;28:246–8. [Google Scholar]
- 28.Crawford PJ, Aldred M, Bloch-Zupan A. Amelogenesis imperfecta. Orphanet J Rare Dis. 2007;2:17. doi: 10.1186/1750-1172-2-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sönmez IS, Aras S, Tunç ES, Küçükesmen C. Clinical success of deproteinization in hypocalcified amelogenesis imperfecta. Quintessence Int. 2009;40:113–8. [PubMed] [Google Scholar]