

Abstract
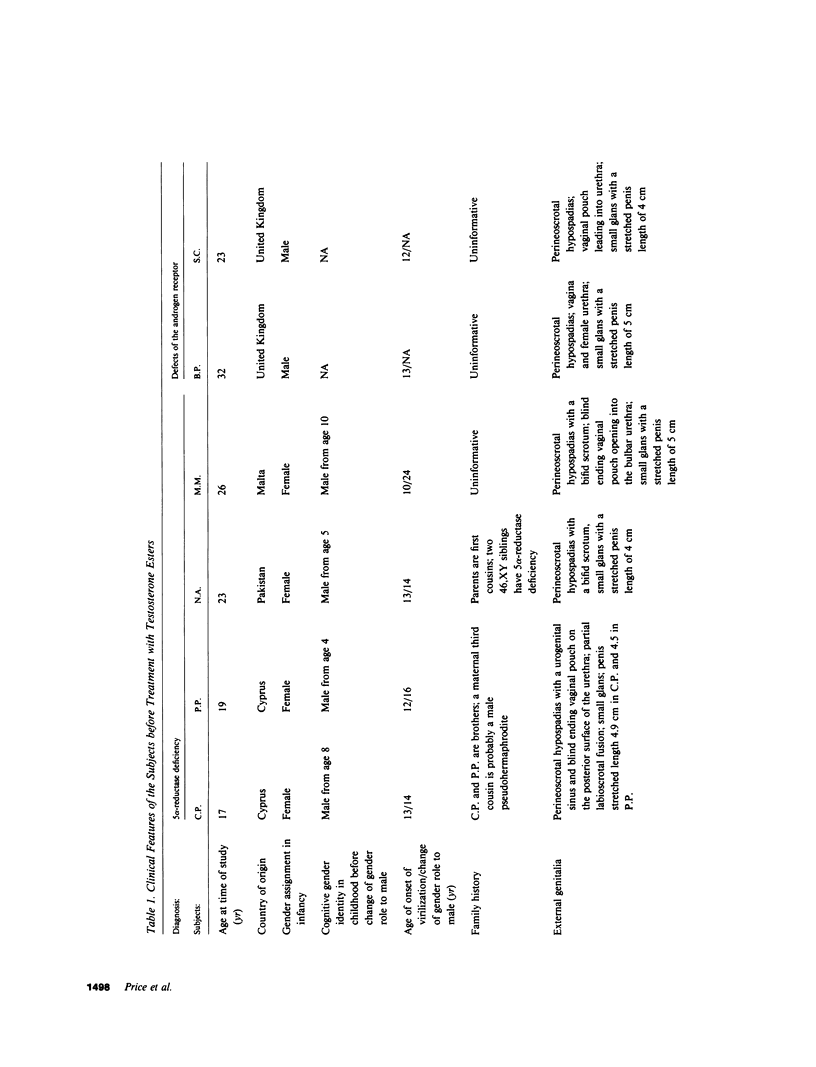
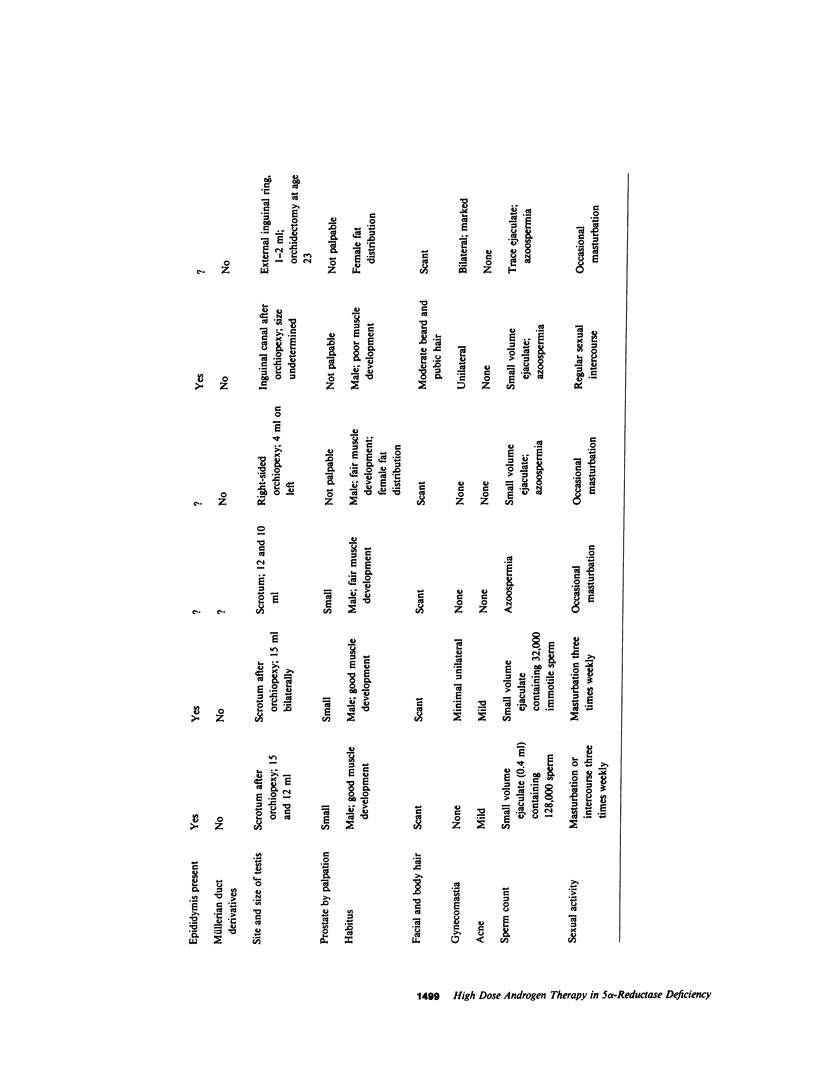
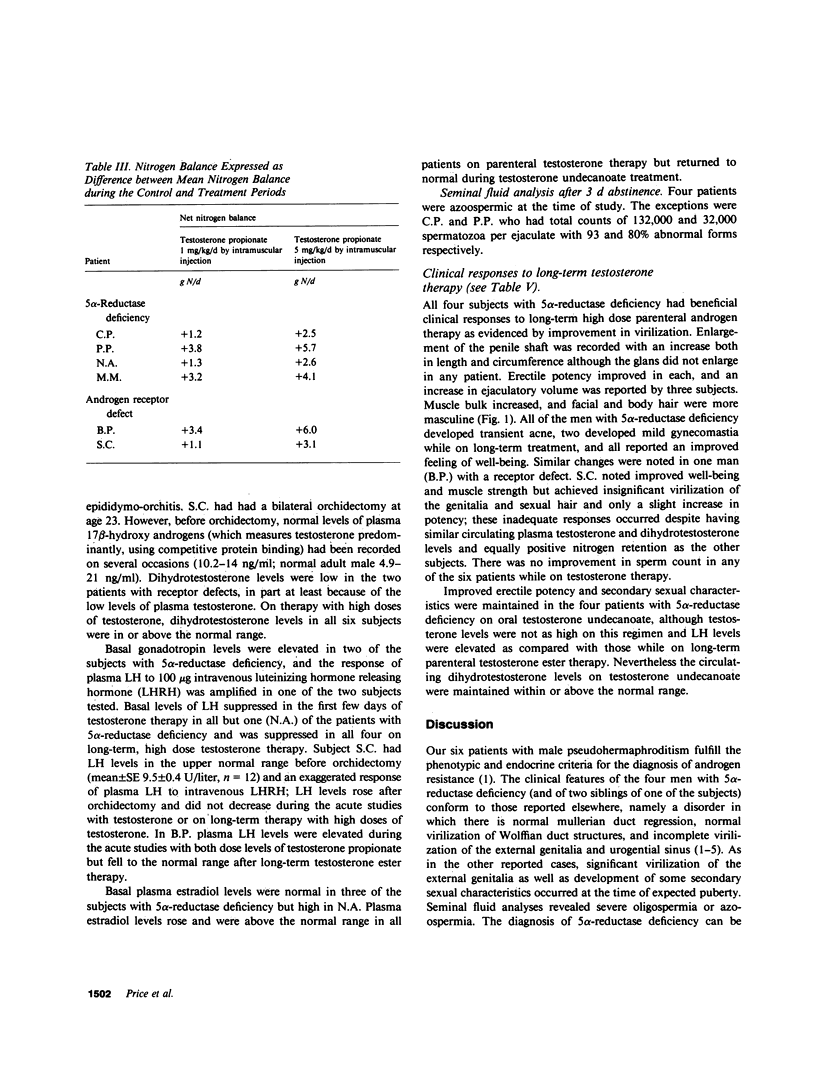
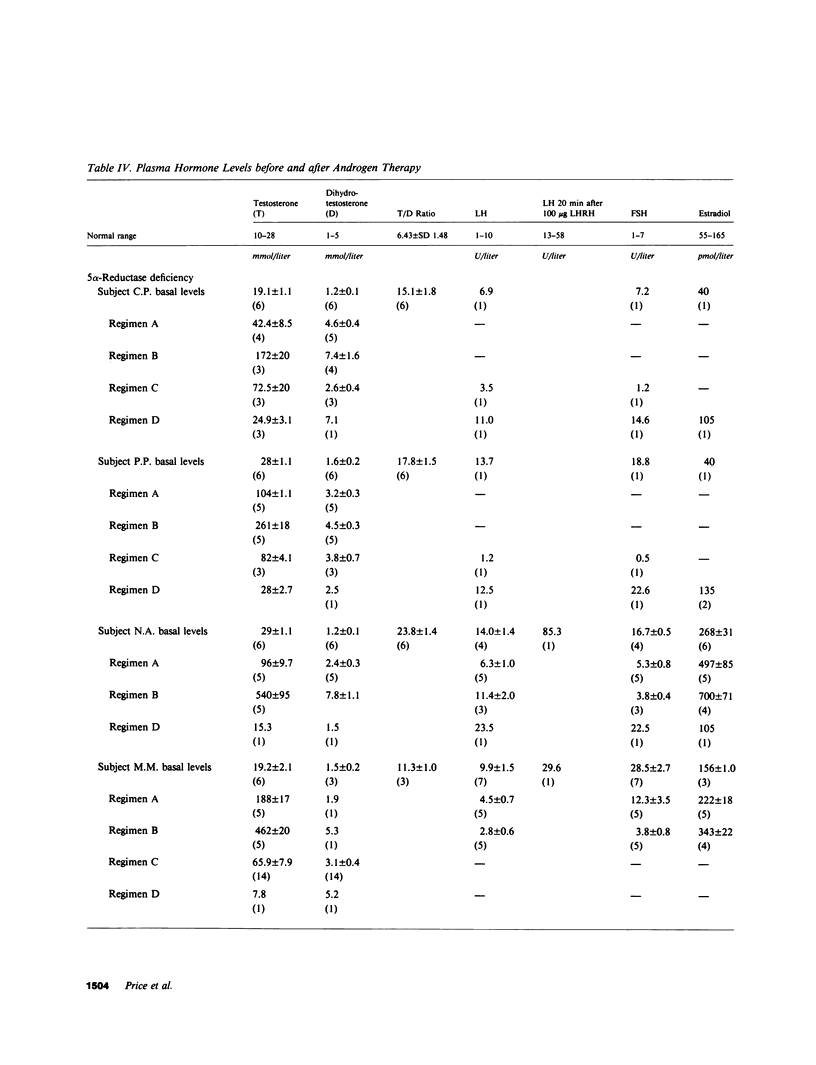
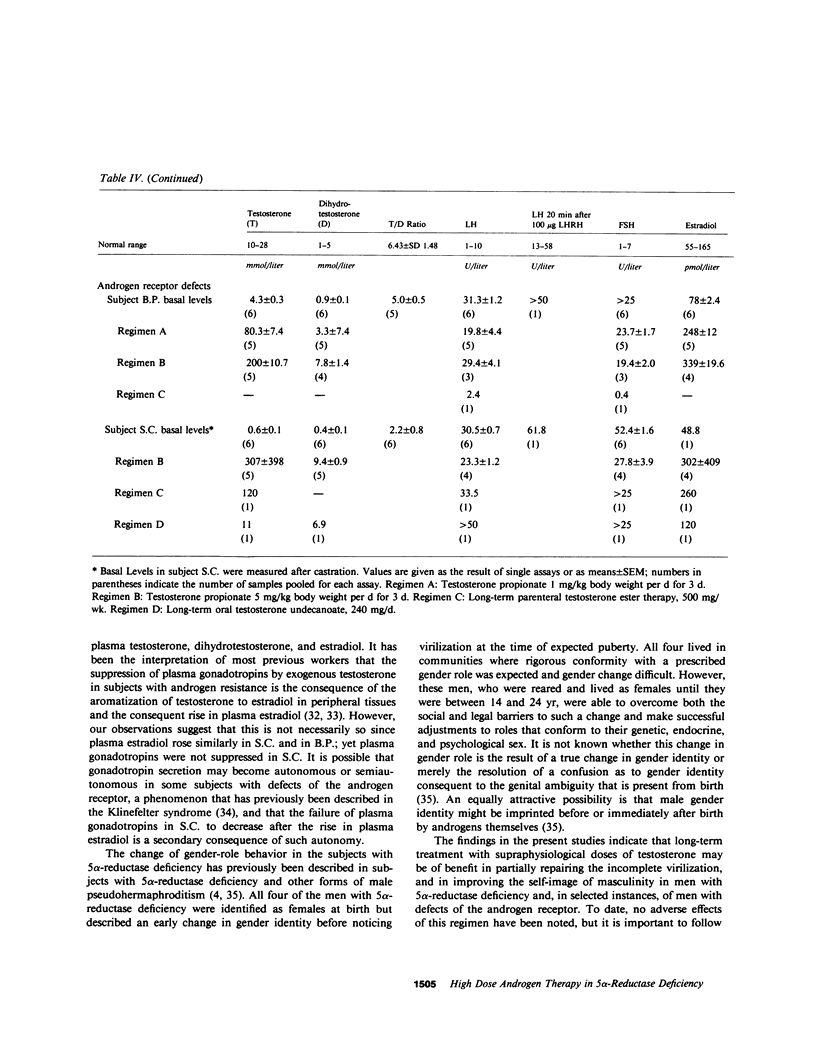
We describe the clinical and biochemical features of six men with male pseudohermaphroditism due to androgen resistance. Each of the subjects had male-gender behavior but incomplete virilization. The underlying defects in androgen metabolism were defined by studies of the 5 alpha-reductase enzyme and the androgen receptor in fibroblasts cultured from biopsies of genital skin. Four of the six have 5 alpha-reductase deficiency, and two have defects of the androgen receptor (the Reifenstein syndrome). The responses of these men to androgen treatment were assessed by monitoring nitrogen balance, plasma luteinizing hormone (LH) values, and clinical parameters of virilization including penile growth, potency and ejaculatory volume, muscle bulk, and growth of body and facial hair. In all of the subjects with 5 alpha-reductase deficiency and one man with the Reifenstein syndrome significant response occurred, as evidence by nitrogen retention, lowered plasma LH levels, and improved virilization, with doses of parenteral testosterone esters that raised plasma testosterone levels above the normal male range and brought plasma dihydrotestosterone levels into the normal male range. The subject who did not respond with clinical virilization nevertheless showed nitrogen retention in response to acute testosterone administration. This patient had a profound deficiency of the androgen receptor, whereas the man with a receptor defect who did respond clinically to therapy had normal amounts of a qualitatively abnormal receptor. We conclude that high dose androgen therapy may be of benefit in improving virilization, self-image, and sexual performance in subjects with 5 alpha-reductase deficiency who have male-gender behavior and in some subjects with defects of the androgen receptor.
Full text
PDF




Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boyar R. M., Moore R. J., Rosner W., Aiman J., Chipman J., Madden J. D., Marks J. F., Griffin J. E. Studies of gonadotropin-gonadal dynamics in patients with androgen insensitivity. J Clin Endocrinol Metab. 1978 Nov;47(5):1116–1122. doi: 10.1210/jcem-47-5-1116. [DOI] [PubMed] [Google Scholar]
- Caminos-Torres R., Ma L., Snyder P. J. Testosterone-induced inhibition of the LH and FSH responses to gonadotropin-releasing hormone occurs slowly. J Clin Endocrinol Metab. 1977 Jun;44(6):1142–1153. doi: 10.1210/jcem-44-6-1142. [DOI] [PubMed] [Google Scholar]
- FAWCETT J. K. The semi-micro Kjeldahl method for the determination of nitrogen. J Med Lab Technol. 1954 Jan;12(1):1–22. [PubMed] [Google Scholar]
- Faiman C., Winter J. S. The control of gonadotropin secretion in complete testicular feminization. J Clin Endocrinol Metab. 1974 Oct;39(4):631–638. doi: 10.1210/jcem-39-4-631. [DOI] [PubMed] [Google Scholar]
- Franchimont P., Kicovic P. M., Mattei A., Roulier R. Effects of oral testosterone undecanoate in hypogonadal male patients. Clin Endocrinol (Oxf) 1978 Oct;9(4):313–320. doi: 10.1111/j.1365-2265.1978.tb02216.x. [DOI] [PubMed] [Google Scholar]
- French F. S., Van Wyk J. J., Baggett B., Easterling W. E., Talbert L. M., Johnston F. R., Forchielli E., Dey A. C. Further evidence of a target organ defect in the syndrome of testicular feminization. J Clin Endocrinol Metab. 1966 May;26(5):493–503. doi: 10.1210/jcem-26-5-493. [DOI] [PubMed] [Google Scholar]
- Griffin J. E., Durrant J. L. Qualitative receptor defects in families with androgen resistance: failure of stabilization of the fibroblast cytosol androgen receptor. J Clin Endocrinol Metab. 1982 Sep;55(3):465–474. doi: 10.1210/jcem-55-3-465. [DOI] [PubMed] [Google Scholar]
- Griffin J. E., Punyashthiti K., Wilson J. D. Dihydrotestosterone binding by cultured human fibroblasts. Comparison of cells from control subjects and from patients with hereditary male pseudohermaphroditism due to androgen resistance. J Clin Invest. 1976 May;57(5):1342–1351. doi: 10.1172/JCI108402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin J. E. Testicular feminization associated with a thermolabile androgen receptor in culutred human fibroblasts. J Clin Invest. 1979 Dec;64(6):1624–1631. doi: 10.1172/JCI109624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin J. E., Wilson J. D. Studies on the pathogenesis of the incomplete forms of androgen resistance in man. J Clin Endocrinol Metab. 1977 Dec;45(6):1137–1143. doi: 10.1210/jcem-45-6-1137. [DOI] [PubMed] [Google Scholar]
- Imperato-McGinley J., Guerrero L., Gautier T., Peterson R. E. Steroid 5alpha-reductase deficiency in man: an inherited form of male pseudohermaphroditism. Science. 1974 Dec 27;186(4170):1213–1215. doi: 10.1126/science.186.4170.1213. [DOI] [PubMed] [Google Scholar]
- Imperato-McGinley J., Peterson R. E., Gautier T., Cooper G., Danner R., Arthur A., Morris P. L., Sweeney W. J., Shackleton C. Hormonal evaluation of a large kindred with complete androgen insensitivity: evidence for secondary 5 alpha-reductase deficiency. J Clin Endocrinol Metab. 1982 May;54(5):931–941. doi: 10.1210/jcem-54-5-931. [DOI] [PubMed] [Google Scholar]
- Imperato-McGinley J., Peterson R. E., Gautier T., Sturla E. Androgens and the evolution of male-gender identity among male pseudohermaphrodites with 5alpha-reductase deficiency. N Engl J Med. 1979 May 31;300(22):1233–1237. doi: 10.1056/NEJM197905313002201. [DOI] [PubMed] [Google Scholar]
- Imperato-McGinley J., Peterson R. E., Leshin M., Griffin J. E., Cooper G., Draghi S., Berenyi M., Wilson J. D. Steroid 5 alpha-reductase deficiency in a 65-year-old male pseudohermaphrodite: the natural history, ultrastructure of the testes, and evidence for inherited enzyme heterogeneity. J Clin Endocrinol Metab. 1980 Jan;50(1):15–22. doi: 10.1210/jcem-50-1-15. [DOI] [PubMed] [Google Scholar]
- Large D. M., Anderson D. C. Twenty-four hour profiles of circulating androgens and oestrogens in male puberty with and without gynaecomastia. Clin Endocrinol (Oxf) 1979 Nov;11(5):505–521. doi: 10.1111/j.1365-2265.1979.tb03103.x. [DOI] [PubMed] [Google Scholar]
- Leshin M., Griffin J. E., Wilson J. D. Hereditary male pseudohermaphroditism associated with an unstable form of 5 alpha-reductase. J Clin Invest. 1978 Sep;62(3):685–691. doi: 10.1172/JCI109176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Medina M., Ulloa-Aguirre A., Fernández M. A., Pérez-Palacios G. The role of oestrogens on gonadotrophin secretion in the testicular feminization syndrome. Acta Endocrinol (Copenh) 1980 Nov;95(3):314–318. doi: 10.1530/acta.0.0950314. [DOI] [PubMed] [Google Scholar]
- Moore R. J., Griffin J. E., Wilson J. D. Diminished 5alpha-reductase activity in extracts of fibroblasts cultured from patients with familial incomplete male pseudohermaphroditism, type 2. J Biol Chem. 1975 Sep 25;250(18):7168–7172. [PubMed] [Google Scholar]
- Moore R. J., Wilson J. D. Steroid 5alpha-reductase in cultured human fibroblasts. Biochemical and genetic evidence for two distinct enzyme activities. J Biol Chem. 1976 Oct 10;251(19):5895–5900. [PubMed] [Google Scholar]
- Perez-Palacios G., Ortiz S., López-Amor E., Morato T., Febres F., Lisker R., Scaglia H. Familial incomplete virilization due to partial end organ insensitivity to androgens. J Clin Endocrinol Metab. 1975 Nov;41(5):946–952. doi: 10.1210/jcem-41-5-946. [DOI] [PubMed] [Google Scholar]
- Peterson R. E., Imperato-McGinley J., Gautier T., Sturla E. Male pseudohermaphroditism due to steroid 5-alpha-reductase deficiency. Am J Med. 1977 Feb;62(2):170–191. doi: 10.1016/0002-9343(77)90313-8. [DOI] [PubMed] [Google Scholar]
- Rosenfield R. L., Lawrence A. M., Liao S., Landau R. L. Androgens and androgen responsiveness in the feminizing testis syndrome. Comparison of complete and "incomplete" forms. J Clin Endocrinol Metab. 1971 May;32(5):625–632. doi: 10.1210/jcem-32-5-625. [DOI] [PubMed] [Google Scholar]
- Savage M. O., Preece M. A., Jeffcoate S. L., Ransley P. G., Rumsby G., Mansfield M. D., Williams D. I. Familial male pseudohermaphroditism due to deficiency of 5 alpha-reductase. Clin Endocrinol (Oxf) 1980 Apr;12(4):397–406. doi: 10.1111/j.1365-2265.1980.tb02727.x. [DOI] [PubMed] [Google Scholar]
- Skakkebaek N. E., Bancroft J., Davidson D. W., Warner P. Androgen replacement with oral testosterone undecanoate in hypogonadal men: a double blind controlled study. Clin Endocrinol (Oxf) 1981 Jan;14(1):49–61. doi: 10.1111/j.1365-2265.1981.tb00364.x. [DOI] [PubMed] [Google Scholar]
- Strickland A. L., French F. S. Absence of response to dihydrotestosterone in the syndrome of testicular feminization. J Clin Endocrinol Metab. 1969 Sep;29(9):1284–1286. doi: 10.1210/jcem-29-9-1284. [DOI] [PubMed] [Google Scholar]
- Walsh P. C., Madden J. D., Harrod M. J., Goldstein J. L., MacDonald P. C., Wilson J. D. Familial incomplete male pseudohermaphroditism, type 2. Decreased dihydrotestosterone formation in pseudovaginal perineoscrotal hypospadias. N Engl J Med. 1974 Oct 31;291(18):944–949. doi: 10.1056/NEJM197410312911806. [DOI] [PubMed] [Google Scholar]
- Wilbert D. M., Griffin J. E., Wilson J. D. Characterization of the cytosol androgen receptor of the human prostate. J Clin Endocrinol Metab. 1983 Jan;56(1):113–120. doi: 10.1210/jcem-56-1-113. [DOI] [PubMed] [Google Scholar]
- Wilson J. D. Dihydrotestosterone formation in cultured human fibroblasts. Comparison of cells from normal subjects and patients with familial incomplete male pseudohermaphroditism, Type 2. J Biol Chem. 1975 May 10;250(9):3498–3504. [PubMed] [Google Scholar]
- Wilson J. D., Griffin J. E., George F. W., Leshin M. The endocrine control of male phenotypic development. Aust J Biol Sci. 1983;36(2):101–128. doi: 10.1071/bi9830101. [DOI] [PubMed] [Google Scholar]