

Abstract
There is a considerable disparity between clinical practice and recommendations based on meta-analyses of antipsychotic polypharmacy in clozapine resistant schizophrenia. For this reason, we investigated the clinical response to reducing the use olanzapine that had been previously added on clozapine treatment among seriously ill hospitalized patients. In a randomized controlled trial with crossover design, we studied volunteer patients (N=15) who had olanzapine added on to clozapine in a state mental hospital. Clozapine monotherapy was just as effective as clozapine-olanzapine therapy, according to results from Clinical Global Impression Scale and Global Assessment of Functioning as primary outcome measures. Polypharmacy is widely used in treating schizophrenia, and usually, add-on medications are started because of worsening of the clinical state. A major confounding feature of these add-ons is whether observed improvements are caused by the medication or explained by the natural fluctuating course of the disorder. The present study, in spite of its small size, indicates the necessity of reconsidering the value of polypharmacy in treating schizophrenia.
Key words: antipsychotics, clozapine, clozapine resistant schizophrenia, polypharmacy, randomized controlled trial
Introduction
Treatment resistance and inadequate response to antipsychotic (AP) medication are significant clinical problems.1 Treatment resistant patients represent 20-30 % of people with schizophrenia.2 These patients are commonly treated with clozapine.3,4 Also, atypical AP monotherapies at therapeutic doses have been suggested to be the best pharmacological treatment of schizophrenia.5 In spite of recommendations, these patients often have added-on polypharmacy with several APs. This augmentation has been questioned in several studies.
From the results of four randomized controlled trials (RCTs), Paton et al.6 suggested that augmentation of clozapine with another AP cannot be recommended but it is worth of a long enough clinical trial. After reviewing 19 RCTs, Correll et al.7 suggested that antipsychotic co-treatment may be superior to monotherapy in certain clinical situations. However, it was not possible to derive firm clinical recommendations from these results. The most commonly used antipsychotic in those trials was clozapine (542 subjects). Thus, it remains unclear whether or not the potential benefits of co-treatment among acute patients are restricted to pharmaceutical combinations that include clozapine. Based on 10 placebo controlled studies, Taylor and Smith8 concluded that the addition of another AP to clozapine was of marginal benefit, but this was only found in studies that lasted up to 16 weeks, and therefore co-treatment seemed to be of doubtful clinical significance. Barbui et al.9 searched through the Cochrane Schizophrenia Group Trials Register, Medline and Embase databases for studies on clozapine monotherapy versus clozapine plus another randomly allocated AP and concluded that the evidence from such studies did not support the rational for adding a second AP to clozapine (Table 1.) Recently, Zink10 stated that adding another AP to clozapine might be beneficial only in cases of treatment-emergent symptoms. Kane and Correll11 also concluded that the value of AP polypharmacy with clozapine remains unclear.
Table 1.
Meta-analysis and reviews on antipsychotic augmentation of clozapine.
| Review | Number of RCTs/ placebo-controlled trials | Number of patients | Design | Deduction/ recommendation |
|---|---|---|---|---|
| Paton et al. 20076 | 4 | 166 | clozapine+AP | worth of long clinical trial |
| Correll et al. 20097 | 19 | 266 | two FGAs | AP+AP superior in certain clinical situations - benefits restricted to clozapine combination? |
| 161 | FGA+SGA | |||
| 133 | two SGAs | |||
| Taylor & Smith 20098 | 10 | 522 | clozapine/clozapine+AP | marginal benefit |
| Barbui et al. 20099 | 21 | 1480 | ||
| 742/738 | clozapine/clozapine+AP | no support for clozapine+AP |
AP, antipsychotic; RCT, randomized controlled trial.
The aim of the present study was to determine if clozapine monotherapy is as effective as clozapine-olanzapine therapy for treatment-resistant schizophrenia in a randomized double-blind setting.
Materials and Methods
Patients
In 2009, 30 schizophrenic patients in the Niuvanniemi State Mental Hospital received clozapine-olanzapine therapy for severe psychotic symptoms after only partially responding to clozapine alone. Of these original 30 patients, 15 volunteered for this study by signing the informed consent. All these volunteers (N=15) participated in the trial. Insufficient response to the medication considered was observed when the Global Assessment of Functioning (GAF)12 had been rated <25 and, on clinical treatment-resistance reported by each patient’s own physician.
The following criteria were required for inclusion; an age of at least 18 years, competence to understand the meaning of the study and give informed consent, insufficient response to clozapine-olanzapine therapy, unchanged psychotropic medication during the last two months and no concurrent pregnancy.
The subjects were randomized in two groups. In group A, olanzapine was gradually changed to placebo for a period of eight weeks and group B received olanzapine add-on. Olanzapine and placebo were dispensed in similar gelatin capsules that were formulated for this trial. After the eight week period, the two groups were crossed over and the treatments repeated (Figure 1). No additional psychotropic medication except benzodiazepine up to 20 mg/day as diazepam equivalents was allowed. A patient was dropped from the study if additional medications were added. After randomization, two patients changed their mind and refused to take part in the trial, and these were dropped from the study (Figure 2).
Figure 1.
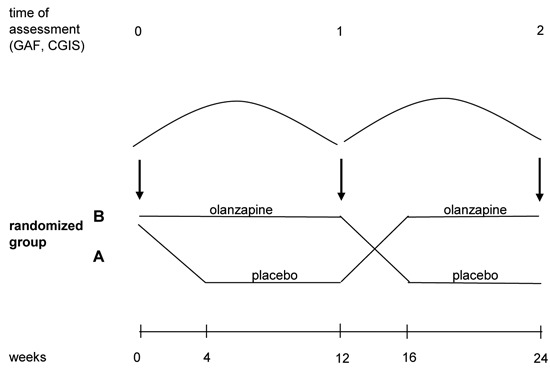
Study design. GAF, Global Assessment of Functioning; CGIS, Clinical Global Impression Scale.
Figure 2.
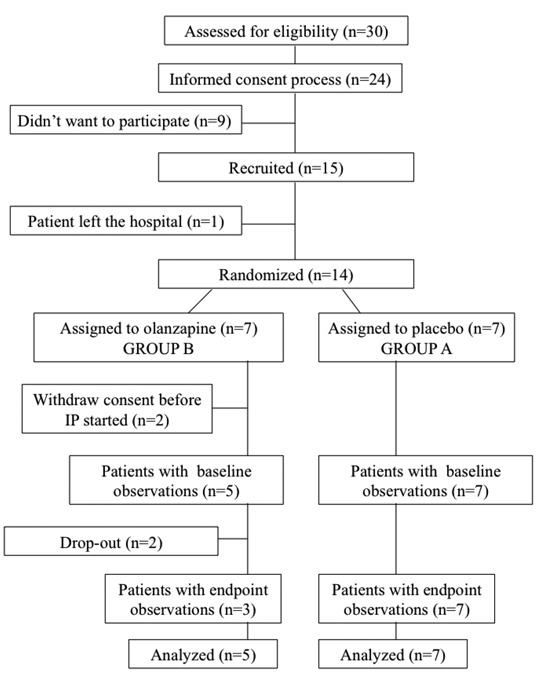
Patient flowchart.
Ethical considerations
Every patient in this study signed the informed consent. The ethical committee of Kuopio University Hospital gave the ethical approval for this study.
This study followed Good Clinical Practice (GCP) and all applicable regulatory requirements and ethical principles described in the Declaration of Helsinki. The validity of informed consent was ensured by two investigators. The rights, safety and well-being of the patients had priority when obtaining informed consent and throughout the study. Foreseeable risks and inconveniences were slight because no new investigational products were used. Olanzapine is a drug with marketing authorization and the placebo contained only pure microcrystal cellulose. In dispensing the investigational product, patients were in the hospital’s wards and received relevant dosages of their study medication regularly at the correct time of the day. The rater (ER-T) is an experienced clinical psychiatrist and forensic psychiatrist with extensive experience in using the applied rating scales. The assistant rater (PK) is a registered nurse and a trained Clinical Research Associate (CRA) who was present during every rating session to reassure all ethical aspects.
Primary outcome measures
The Clinical Global Impression Scale (CGIS)13 was applied at baseline and at study weeks 12 and 24. The Global Assessment of Functioning (GAF)12 was administered at the same time points. Both CGIS and GAF are commonly used in clinical psychiatry. The rater was blind to the study medication (i.e., either olanzapine or placebo) until the completion of the trial in each case.
Statistical Methods
Changes in GAF and CGIS were determined by using the equivalence test of means. In spite of the small sample size, a parametric test was used since GAF was normally distributed. The same test was applied for CGIS without normal distribution, because no non parametric equivalence test of means is available. A clinically meaningful change of GAF was set to 10, and to 1 for CGIS. Changes smaller than these values were considered to be clinically insignificant.
The equivalence tests of means were performed by using two-one side t-tests (TOST), using the hypotheses H0: M1-M2 <-10 or M1-M2>10 versus H1: Equivalence for GAF and H0: M1-M2 <-1 or M1-M2 >1 versus H1: Equivalence for CGIS, with H0 representing clinically significant changes in the means of each parameter and H1 representing equality.
Results
The patients in group A (N=7) were all male, while group B (N=5) consisted of 1 female and 4 male patients. Patient age, GAF-and CGIS-ratings at week 0 are presented in Table 2. The groups did not differ significantly from each other according to these parameters. The means and SD’s of GAF and CGIS in both groups, as well as changes of means in GAF- and CGIS-ratings from week 0 to week 12 and effect sizes are presented in Table 2.
Table 2.
Age, Global Assessment of Functioning and Clinical Global Impression Scale scores at weeks 0 and 12, and their changes from weeks 0 to 12, with mean differences of the changes and effect sizes.
| range | mean (SD) | range | mean (SD) | (Cohen’s d) | ||
|---|---|---|---|---|---|---|
| age, years | 32-51 | 44.14 (7.60) | 39–63 | 50 (9.57) | ||
| GAF, week 0 | 13-21 | 17.57 (3.05) | 12–25 | 19 (6.60) | ||
| GAF, week12 | 13-21 | 18.14 (2.79) | 9–25 | 18.8 (7.09) | ||
| GAF change 0-12 | -2-3 | 0.57 (1.62) | -3–2 | -0.20 (1.79) | 0.77 | 0.45 |
| CGIS, week 0 | 4-7 | 5.29 (0.95) | 5–7 | 5.6 (0.89) | ||
| CGIS, week12 | 4-7 | 5.29 (0.95) | 5–7 | 5.8 (1.10) | ||
| CGIS change 0-12 | 0-0 | 0.00 (0.00) | 0–1 | 0.20 (0.45) | -0.2 | -0.63 |
GAF, Global Assessment of Functioning; CGIS, Clinical Global Impression Scale.
The equivalence tests indicated the probability for clinically significant change as follows; P values <0.0001 for changes in the GAF and P values <0.0003 for changes in the CGIS. Thus, clinical changes in groups A and B for both parameters were considered to be equivalent.
In other words, clozapine monotherapy was just as effective as clozapine-olanzapine therapy in this study sample.
The results obtained by week 24 were not valid, due to the reduced number of cases by the end of the study. Therefore, only the results of the first 12 weeks are presented. During the study, one patient dropped out at study week 18+1 because of dizziness. Also, this patient thought he had developed the symptom due to the investigational product. However, he had the same adverse event at study week 12. This patient was randomized to group B, meaning that the placebo phase was going on at the time of his discontinuation.
Another patient’s participation in the trial was prematurely discontinued at study week 5 according to the protocol, and in this case the change in CGIS was clinically remarkable (-3). This patient suffered from intense mood changes, physical tiredness, increased psychotic symptoms and mental inflexibility. This patient had also been randomized to group B, hence he had received olanzapine preceding the discontinuation.
Otherwise, no serious adverse events occurred during the trial.
Discussion
Among studies concerning AP co-treatment with clozapine, this is the first study that was designed to identify clinical differences after reducing and subsequently removing an added-on AP, and in every case the same added-on AP; i.e. olanzapine. These conditions can be mentioned as particular strengths of this study. Still, an additional strength was that the patients were constantly hospitalized, which minimized potential mistakes in the administration of medication. A severe limitation of this study was the inherent heterogeneity of the disorder called schizophrenia, in addition to the small sample size. As individual features of this illness are highlighted among the treatment resistant patients, these results cannot be generalized to all schizophrenic patients. Although the study population was small, the resulting P values were low enough to show the equality of changes in critical parameters with modest effect size. The reliability of the result concerning CGIS may be affected by the use of a parametric test. However, the overall results indicate that that clozapine alone was equally effective as with added-on olanzapine, which means that polypharmacy was of no clinical benefit among these patients refractory to treatment schizophrenia. The conclusion is in line with the previous findings of wider reviews6-9 and recommendations.3-5,10,11
Polypharmacy is widely used in treating schizophrenia. The natural fluctuating course (i.e. regression to the mean) of the disease remains a major issue.
Add-on medications are administered when the clinical state has worsened, and sooner or later the state may get better, which could happen as well without add-on medication. However, this change is considered to be caused by augmented medication. In the present study, the clinical state of one patient worsened to the point of discontinuation. When the blind code was broken it was observed that he had on-going olanzapine as he had had before the trial.
In the present study, we did not find any specific reduction in side effects after reducing the added on AP. However, the long-term administration of unnecessary medication tends to cause needless side effects.
Conclusions
The clinical state of seriously ill schizophrenic patients who were on olanzapine-clozapine therapy was not affected by discontinuation of olanzapine. The natural fluctuating course of schizophrenia is often represented by worsening of psychotic symptoms which may lead to long-lasting and unnecessary AP polypharmacy.
Acknowledgements
The study was supported by funding from the Annual EVO Financing (special government subsidies from the Ministry of Health and Welfare, Finland). The researchers were independent from the funder. Data analyses were done by Timo Pessi, who is not incluced as an author.
References
- 1.Hegarty JD, Baldessarini RJ, Tohen M, et al. One hundred years of schizophrenia: a meta-analysis of the outcome literature. Am J Psychiatry 1994;151:1409-16. [DOI] [PubMed] [Google Scholar]
- 2.Conley RR, Kelly DL.Management of treatment resistance in schizophrenia. Biol Psychiatry 2001;50:898-911. [DOI] [PubMed] [Google Scholar]
- 3.Kane JM, Honigfeld G, Singer J, Meltzer H.Clozapine in treatment-resistant schizophrenics. Psychopharmacol Bull 1988;24:62-7. [PubMed] [Google Scholar]
- 4.Meltzer HY.Treatment of the neuroleptic-nonresponsive schizophrenic patient. Schizophr Bull 1992;18:515-42. [DOI] [PubMed] [Google Scholar]
- 5.Stahl SM, Grady MM.A critical review of atypical antipsychotic utilization: comparing monotherapy with polypharmacy and augmentation. Curr Med Chem 2004;11:313-27. [DOI] [PubMed] [Google Scholar]
- 6.Paton C, Whittington C, Barnes TR.Augmentation with a second antipsychotic in patients with schizophrenia who partially respond to clozapine: a meta-analysis. J Clin Psychopharmacol 2007;27:198-204. [DOI] [PubMed] [Google Scholar]
- 7.Correll CU, Rummel-Kluge C, Corves C, Kane JM, Leucht S.Antipsychotic combinations vs monotherapy in schizophrenia: a meta-analysis of randomized controlled trials. Schizophr Bull 2009;35:443-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Taylor DM, Smith L.Augmentation of clozapine with a second antipsychotic: a meta-analysis of randomized, placebo-controlled studies. Acta Psychiatr Scand 2009;119:419-25. [DOI] [PubMed] [Google Scholar]
- 9.Barbui C, Signoretti A, Mulè S, et al. Does the addition of a second antipsychotic drug improve clozapine treatment? Schizophr Bull 2009;35:458-68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zink M, Englisch S, Meyer-Lindenberg A.Polypharmacy in schizophrenia. Curr Opin Psychiatry 2010;23:103-11. [DOI] [PubMed] [Google Scholar]
- 11.Kane JM, Correll CU.Past and present progress in the pharmacologic treatment of schizophrenia. J. Clin Psychiatry 2010;71:1115-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.American Psychiatric Association. The global assessment of functioning (GAF). APA 1987. [Google Scholar]
- 13.Guy W.ECDEU assessment manual for psychopharmacology. Rockville: US Department of Health, Education, and Welfare; 1976. pp. 217-222. [Google Scholar]