

Abstract
Purpose
MicroRNAs (miRNAs) have been widely investigated as potential biomarkers for several malignancies. To establish the feasibility of miRNA expression profiling of small biopsy samples of pancreatic cancers, we assessed expression profiles in freshly collected aspirates obtained immediately after surgical resection of the pancreas.
Methods
We used separate fine needles (20-23 gauge) to aspirate the pancreatic cancer and adjacent normal pancreatic tissue. miRNAs that were differentially expressed in pancreatic cancers and matched paraneoplastic normal pancreatic tissues were identified using an miRNA microarray.
Results
We identified 158 aberrantly expressed miRNAs in pancreatic cancers; 51 were overexpressed and 107 underexpressed compared with normal pancreatic tissue. To confirm the microarray findings, quantitative RT-PCR was performed on individual samples. We chose eight miRNAs for further analysis; of which five were overexpressed (miR-21, miR-27a, miR-146a, miR-200a, and miR-196a) and three underexpressed (miR-217, miR-20a, and miR-96) in pancreatic cancer samples compared to benign pancreatic tissue. Expression of miR-21, miR-27a, miR-146a, miR-200a, and miR-196a was significantly increased in cancer fine-needle aspirates relative to matched controls in all samples. Expression of miR-217, miR-20a, and miR-96 was significantly downregulated in almost all pancreatic cancer tissues.
Conclusion
We demonstrate the feasibility of performing miRNA profiling on very small specimens obtained using fine-needle aspiration of pancreatic cancers.
Keywords: MicroRNAs, Pancreatic neoplasms, Biopsy, Fine-needle
INTRODUCTION
Pancreatic surgery is associated with a high rate of complications because of distinctive features of the pancreas (the tissue is soft and exerts an exocrine function). The resection field is usually both extensive and destructive because the pancreas lies deep and is in close proximity to surrounding organs [1]. Therefore, a correct differential diagnosis is important to avoid unnecessary operations on patients with benign pancreatic diseases, such as pancreatitis and pancreatic tuberculosis, which can be confused with pancreatic malignancies. If a pancreatic lesion is obscure, a biopsy is usually performed via fine-needle aspiration (FNA) guided by endoscopic ultrasound (EUS). However, biopsy interpretation may be hindered by the small sample size and the presence of inflammatory changes that mask or mimic neoplasms [2,3]. Thus, the utility of biopsies in the making of medical decisions on surgery is rather limited. Many researchers have sought to identify biomarkers that accurately distinguish pancreatic cancer from benign pancreatic lesions [4].
MicroRNAs (miRNAs) have been widely investigated as potential biomarkers for several malignancies [5,6,7,8]. Pancreatic ductal adenocarcinoma has a unique miRNA signature that may help differentiate pancreatic cancer from other diseases [9,10,11,12,13,14]. However, the potential application of these markers to preoperative evaluation of pancreatic lesions has not yet been investigated extensively.
In the present work, we obtained the miRNA expression profiles of freshly collected aspirates to explore the feasibility of miRNA expression profiling of pancreatic cancer in small biopsy samples.
METHODS
Tissue collection
Surgical specimens from 11 consecutive patients who had undergone resection for pathologically confirmed pancreatic ductal adenocarcinoma, from January 2013 through August 2013, were subjected to miRNA profiling. FNA (2-5 needle passes per patient; mean, 3.5) using 20- to 23-gauge needles was performed separately on cancer masses and adjacent normal pancreatic tissue immediately after operation. This procedure was the same as that of diagnostic FNA, which is performed during preoperative evaluation of a pancreatic mass in a clinical setting. We also obtained tissue sections of pancreatic ductal adenocarcinomas from another 19 patients, and cryopreserved these samples for comparative analysis.
This study was approved by the Institutional Review Board of the Catholic University of Korea College of Medicine, and all patients gave informed consent in the manner prescribed by the Declaration of Helsinki. All tissues were anonymized, and analyses were performed in parallel to avoid batch effects.
RNA extraction
RNA was extracted using Ambion RecoverAll Total Nucleic Acid Isolation Kits (Ambion, Austin, TX, USA). In short, tissue samples were ground and subjected to protease digestion in RNAse-free tubes. RNA was captured on glass-fiber filters and eluted into 60-mL amounts of nuclease-free water after washing in ethanol. RNA levels were quantified using a NanoDrop 8000 spectrophotometer (NanoDrop, Wilmington, DE, USA). FNA specimens from normal pancreatic tissues yielded 1.2-41 mg of total RNA (mean, 15.8 µmg). FNA specimens from cancer tissues yielded considerably less RNA, ranging from 1.0 to 32 µg (mean, 5.9 µg). RNA was extracted as follows: After vigorous manual shaking, each sample was centrifuged for 5 minutes at room temperature to remove debris. The supernatant was removed, 0.2-mL chloroform per 1 mL of TRIzol added, and incubation for 2-5 minutes at room temperature followed (after vigorous shaking). All samples were centrifuged for 15 minutes at 4℃ at no more than 12,000 × g, yielding a lower red phenolchloroform phase, an interphase, and a colorless upper aqueous phase containing all of the RNA. This phase was transferred to a fresh tube and RNA precipitated by addition of 500-µL isopropanol. All samples were centrifuged again for 15 minutes at 4℃ and the RNA precipitate formed a gel-like pellet on the sides and bottom of the tube. Ethanol (0.25 mL per 1 mL of TRIzol) was added and the sample applied directly to an RNeasy column and then washed with buffer to remove impurities. RNA was eluted in a final volume of 15 µL.
MicroRNA profiling
Fresh samples from 11 pancreatic ductal adenocarcinomas and 11 matched adjacent normal pancreatic tissues were analyzed using the miRCURY LNA Array platform (Exiqon, Woburn, MA, USA). In each case, 750-ng amounts of test and control total RNA were labeled with Hy3 and Hy5 fluorescent materials, respectively, using mercury LNA microRNA Hi-Power Labeling Kits, Hy3/Hy5 (Exiqon, Vedbaek, Denmark) following the procedure described by the manufacturer. Each Hy3-labeled test sample and Hy5-labeled reference sample were mixed and hybridized to the seventh-generation array, which features capture probes targeting all human, mouse, and rat miRNAs registered in miRBASE 16.0. Hybridized chips were washed, processed to detect biotin-containing transcripts (using the streptavidin-Alexa647 conjugate), and scanned on an Axon 4000B microarray scanner (Axon Instruments, Sunnyvale, CA, USA). We next analyzed miRNA expression using miRCURY LNA Arrays containing Tm-normalized capture probes for 3,100 miRNAs, including all known and registered miRNAs, and human miRPlus sequences not yet annotated in miRBase.
Quantitative real-time PCR (to quantify the levels of eight selected miRNAs)
Real-time RT-PCR was performed on all samples to validate miRNA profiling results; we used an ABI 7500 Fast Real-time PCR platform (Applied Biosystems, a division of Thermo Fisher Scientific Inc., Waltham, MA, USA) to this end. We selected eight miRNAs identified as of interest by miRNA microarray profiling (upregulated: miR-21, miR-27a, miR-146a, miR-200a, and miR-196a; downregulated: miR-217, miR-20a, and miR-96). Reverse transcription was performed using species-specific primers (Applied Biosystems) (Table 1). Data were analyzed with the aid of ABI Prism 7700 SDS software (Applied Biosystems).
Table 1.
Primers for reverse transcription-polymerase chain reaction
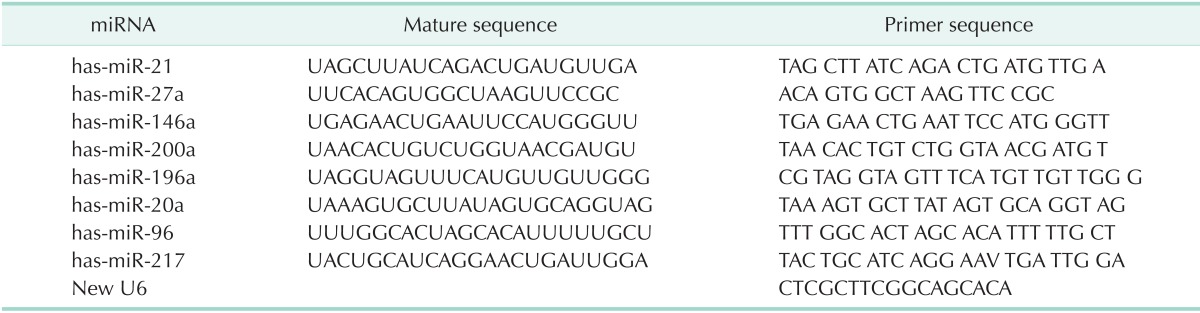
miRNA, microRNA.
Statistical and bioinformatic analysis
Data from each FNA specimen were analyzed as follows. The miRNA levels measured on the chips were converted into discrete variables by splitting the samples into two classes (highand low-level expression) using the mean miRNA expression level as a threshold. On expression analysis, P-values were calculated using Student t-test after adjustment using Benjamini and Hochberg multiple testing. The confidence levels of the chosen means were 95%. All calculations were performed with the aid of R/bioconductor (principally the limma package). miRNA profiling identified a subset of 99 top miRNAs (miRNAs associated with P-values less than 0.05) of all miRNAs targeted by the Array that were differentially expressed in cancer and normal tissues. Next, all samples were subjected to quantitative RT-PCR (qRT-PCR) to amplify each of eight selected miRNA species. miRNA expression levels in pancreatic cancer samples were calculated and compared to those of normal pancreatic tissues. Relative expression levels were analyzed using the cycle threshold (Ct) method. The expression level of each miRNA was normalized to that of U6sn RNA (an internal control). Control amplification of the small endogenous RNA U6 (a housekeeping gene) was performed on all samples. The postamplification thresholds for all samples were set to be identical, to allow the Ct values of each miRNA to be compared. Mean Ct values were calculated for each specimen and normalized to those of RNA U6 in the same samples. Thus: miRNA expression levels were normalized by subtracting the Ct value of the U6sn RNA internal control from that of each miRNA (Ct miRNA minus Ct U6sn). All data are presented as such normalized Ct values, and miRNA expression levels in controls (paraneoplastic normal pancreatic tissues) were set to 1.0.
RESULTS
The clinical and pathological features of 11 FNA and 19 cryopreserved specimens are summarized in Table 2. All malignant specimens were pathologically confirmed to exhibit pancreatic ductal adenocarcinoma, and all paraneoplastic normal pancreatic tissues were found to be free of malignant cells upon retrospective review of pathologists' reports.
Table 2.
The clinical and pathological features of 11 FNAretrieved and 19 cryopreserved pancreas ductal adenocarcinoma samples

FNA, fine-needle aspiration.
Expression profiling of miRNAs
miRNAs differentially expressed in pancreatic cancers and matched paraneoplastic normal pancreatic tissues were identified using the miRNA microarray. Fig. 1 shows a heat map and hierarchical clustering data revealing the overall expression patterns of the miRNAs. Red represents an expression level higher than normal, and green lower than normal. Microarray analysis identified 158 differentially expressed miRNAs; 51 were overexpressed and 107 underexpressed in pancreatic cancer compared to normal pancreatic tissue. Of these miRNAs, the top 10 differentially expressed miRNAs (up or down) are shown in Table 3.
Fig. 1.
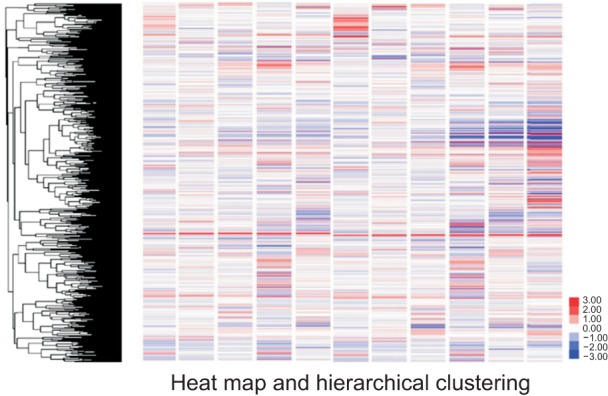
A heat map and hierarchical clustering showing the overall expression patterns of microRNAs. Red represents an expression level higher than that of the normal control, and green lower expression.
Table 3.
The top 10 differentially expressed (up or down) miRNAs in pancreatic cancer compared with normal pancreatic tissue

miRNA, microRNA.
a)Average Hy3 signal intensity. b)Log2 (-fold change) when the miRNA expression levels of test and control samples were compared.
qRT-PCR of selected miRNAs
We performed quantitative real-time PCR on individual samples to confirm the microarray data. We chose eight miRNAs (exhibiting at least a threefold change in expression level) for further analysis based on the miRNA profiling data described above, and literature data [15,16,17]. These were five overexpressed (miR-21, miR-27a, miR-146a, miR-200a, and miR-196a) and three underexpressed (miR-217, miR-20a, and miR-96) miRNAs. In other words, these miRNAs were expressed to greater and lesser levels in cancer compared to control tissue, respectively.
The levels of all of miR-21, miR-27a, miR-146a, and miR-196a were significantly higher in FNA specimens from cancer tissue relative to matched control tissue in all samples, and, in more than half of the samples, the level was >10 folds greater. However, the expression level of miR-200a varied, in contrast to what we expected, considering the high level of integration of the microarray data (Figs. 2, 3). Compared to the levels in control tissue, the expression levels of miR-217, miR-20a, and miR-96 were significantly downregulated in almost all pancreatic cancer tissues (Figs. 2, 3).
Fig. 2.

Comparative expression analysis of miR-21 (A), miR-27a (B), miR-146a (C), miR-200a (D), miR-196a (E), miR-217 (F), miR-20a (G), and miR-96 (H) levels in 11 fine-needle aspiration specimens from cancer relative to matched normal control tissue, as estimated by quantitative RT-PCR. The expression levels in control paraneoplastic normal pancreatic tissues were set to 1.0 in terms of log2 values.
Fig. 3.

Box plot showing the overall expression levels of eight species of microRNAs (miRNAs) as revealed by quantitative RT-PCR (qRT-PCR) in 11 fine-needle aspiration specimens from cancer compared to control tissue. The expression levels in control paraneoplastic normal pancreatic tissues were set to 1.0 in terms of log2 values.
In addition, the mean expression levels of the eight species of miRNAs were assessed by qRT-PCR in 19 cryopreserved sections of pancreatic cancer compared with 11 control tissues. The results were similar to those described above: The expression levels of miR-21, miR-27a, miR-146a, miR-200a, and miR-196a were significantly higher, and those of miR-217, miR-20a, and miR-96 significantly lower, in cancer specimens than controls (Fig. 4). The reproducibility of the qRT-PCR assay showed that miRNAs can be efficiently extracted from fresh FNA specimens, allowing data from multiple samples to be compared.
Fig. 4.

Box plot showing the expression levels of eight species of microRNAs (miRNAs), assessed using quantitative RT-PCR (qRT-PCR), in 19 cryopreserved sections of pancreatic cancer tissue compared with 11 control tissues. The expression levels in control paraneoplastic normal pancreatic tissues were set to 1.0 in terms of log2 values.
DISCUSSION
It is essential to develop sensitive and specific biomarkers for diagnosis of pancreatic cancer because most patients are asymptomatic at early stages, and the disease may be inoperable at diagnosis. The differential diagnosis of pancreatic cancer from benign conditions including pancreatitis and pancreatic tuberculosis is also a major problem. The potential morbidity and mortality associated with needless radical resection, frequently accompanied by serious complications, must be avoided [18,19,20]. Conventional diagnostic methods such as imaging (enhanced CT or MRI), serum tumor marker analysis (of CA19-9, CA-125, and CEA levels), and other modalities, do not always aid in differential diagnosis, and are sometimes poorly effective [20,21]. Thus, an objective molecular test preoperatively discriminating pancreatic cancer from benign pancreatic disease would be clinically valuable.
miRNAs have received considerable attention as potential biomarkers of human malignancies [6,7,12]. miRNAs are 18- to 24-nucleotide noncoding RNA molecules exhibiting remarkable evolutionary conservation. The principal functions of miRNAs are regulation of the stability and translation of nuclear mRNA transcripts. In general, miRNAs negatively regulate the expression of genes involved in many biological processes, including development, differentiation, and apoptosis. Acting posttranscriptionally, the molecules may fine-tune the expression levels of as many as 30% of all mammalian proteinencoding genes. To date, more than 700 human miRNAs have been identified [5]. Aberrant miRNA expression has been implicated in the initiation and progression of certain diseases, including various cancers. Approximately half of all human miRNA genes are located in fragile chromosomal regions affected in various human cancers [15]. The classic view of cancer as a genetic disease influenced by expression of oncogenes or tumor suppressor genes that code for proteins is now expanding to include miRNAs. Abnormal miRNA expression in cancer suggests that the miRNAs may be used as diagnostic signatures. Further, a molecular signature derived from about 200 miRNAs could be superior in terms of cancer classification in comparison to mRNA expression profiles of over 20,000 genes. Another technical advantage is the small size of miRNAs, reducing susceptibility to degradation not only in frozen but also formalin-fixed paraffin-embedded tissues, allowing for wider application of miRNA profiling in readily available clinical samples [13,22,23].
Considerable evidence has accumulated showing that miRNAs influence the course of numerous cancers. Thus, miR-21, miR-92am, and miR-200c are involved in colorectal cancer; let- 7 and miR-16 in nonsmall cell lung cancer; upregulation of miR-142 in diffuse large B-cell lymphomas; miR-146a and miR-222 in thyroid cancer; and miR-222 and miR-29a in breast cancer [24]. Pancreatic ductal adenocarcinoma has a unique miRNA signature featuring significantly higher expression of miR-21, miR-10b, miR-15b, miR-27a, miR-155, miR-146a, miR-210, miR-100, miR-200a, and miR-196a; and decreased expression of miR-217, miR-375, miR-30a, miR-20a, and miR-96, compared to the miRNA profiles of nonneoplastic pancreatic tissue [9,10,11,12,13,14]. However, miRNA profiling of pancreatic cancer has hitherto used experimental cell lines or paraffin/formalinpreserved pancreatic cancer tissues from surgical specimens. Consequently, although preclinical promise has been shown, no miRNA profiling method is yet recommended for clinical application in the management of patients with pancreatic lesions, not even for the preoperative differential diagnosis of pancreatic cancer from benign lesions.
In the present study, we sought to develop miRNA profiling of pancreatic cancer as a diagnostic tool. Current diagnosis and staging of pancreatic cancer are based on a combination of traditional radiological imaging and histological or cytological diagnosis using small amounts of tissue retrieved via EUSguided FNA, which requires the assistance of an experienced pathologist. Even the use of advanced imaging techniques followed by histological evaluation by a proficient pathologist sometimes fails to differentiate benign from malignant pancreatic lesions. Up to 6% of the cases suspected as malignant turn out to be benign at surgery, and the patients suffer needless postsurgical complications [21].
If the preoperative diagnosis of a pancreatic lesion is ambiguous, how might treatment be planned? We performed miRNA analysis on pancreatic FNA samples obtained from surgically resected specimens, not via biopsy. EUS-guided FNA is rather invasive and the amount of tissue retrieved is very small. The use of this procedure for research purposes, and not for practical diagnosis of a patient, would be unethical and therefore impossible. FNA of fresh surgical specimens immediately following resection reproduces the preoperative diagnostic procedure in current clinical practice, in the absence of ethical concerns. This approach also allowed us to compare miRNA profiles between a cancerous lesion and paraneoplastic normal pancreatic tissue from the same individual. To our knowledge, this is a unique feature of our present study.
Our immediate objective was to determine whether it was feasible to collect miRNA microarray and qRT-PCR data from very small amounts of fresh tissue obtained via diagnostic FNA. We assessed miRNA expression profiles in freshly collected materials obtained immediately after resection using separate needles to aspirate cancer and adjacent normal tissue. A total of 158 miRNAs was differentially expressed in the two tissues, as revealed by the miRCURY LNA Array platform. Consistent with earlier data on immortalized pancreatic cancer cell blocks and banked cancer tissue [12,13,16,22], we found that the expression levels of miR-21, miR-27a, miR-146a, miR-200a, and miR-196a were higher, and those of miR-217, miR-20a, and miR-96 lower, in FNA samples of cancers. Comparative qRT-PCR analysis of the expression levels of miR-21, miR-27a, miR-146a, miR-200a, and miR-196a in FNAs from 11 pancreatic cancers showed that all were expressed at significantly higher levels, in almost all samples, compared to normal tissue. In contrast, the expression levels of miR-217, miR-20a, and miR-96 were significantly lower in all samples.
In conclusion, we have shown that it is feasible to perform miRNA profiling of very small pancreatic cancer specimens obtained using FNA. The work may yield an important preoperative diagnostic tool, especially in terms of lesion resection. We found that the amount of tissue in most FNA samples sufficed for quantitative analysis of miRNA expression. Differentially regulated miRNAs observed in cryopreserved resection specimens of pancreatic cancer were also identified in freshly collected FNA materials.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Grobmyer SR, Pieracci FM, Allen PJ, Brennan MF, Jaques DP. Defi ning morbidity after pancreaticoduodenectomy: use of a prospective complication grading system. J Am Coll Surg. 2007;204:356–364. doi: 10.1016/j.jamcollsurg.2006.11.017. [DOI] [PubMed] [Google Scholar]
- 2.Godfrey EM, Rushbrook SM, Carroll NR. Endoscopic ultrasound: a review of current diagnostic and therapeutic applications. Postgrad Med J. 2010;86:346–353. doi: 10.1136/pgmj.2009.096065. [DOI] [PubMed] [Google Scholar]
- 3.Tadic M, Stoos-Veic T, Vukelic-Markovic M, Curic J, Banic M, Cabrijan Z, et al. Endoscopic ultrasound in solid pancreatic masses: current state and review of the literature. Coll Antropol. 2010;34:337–340. [PubMed] [Google Scholar]
- 4.Garcea G, Neal CP, Pattenden CJ, Steward WP, Berry DP. Molecular prognostic markers in pancreatic cancer: a systematic review. Eur J Cancer. 2005;41:2213–2236. doi: 10.1016/j.ejca.2005.04.044. [DOI] [PubMed] [Google Scholar]
- 5.Kloosterman WP, Plasterk RH. The diverse functions of microRNAs in animal development and disease. Dev Cell. 2006;11:441–450. doi: 10.1016/j.devcel.2006.09.009. [DOI] [PubMed] [Google Scholar]
- 6.Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer. 2006;6:857–866. doi: 10.1038/nrc1997. [DOI] [PubMed] [Google Scholar]
- 7.Budhu A, Ji J, Wang XW. The clinical potential of microRNAs. J Hematol Oncol. 2010;3:37. doi: 10.1186/1756-8722-3-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Srivastava SK, Bhardwaj A, Leavesley SJ, Grizzle WE, Singh S, Singh AP. MicroRNAs as potential clinical biomarkers: emerging approaches for their detection. Biotech Histochem. 2013;88:373–387. doi: 10.3109/10520295.2012.730153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nakata K, Ohuchida K, Mizumoto K, Kayashima T, Ikenaga N, Sakai H, et al. MicroRNA-10b is overexpressed in pancreatic cancer, promotes its invasiveness, and correlates with a poor prognosis. Surgery. 2011;150:916–922. doi: 10.1016/j.surg.2011.06.017. [DOI] [PubMed] [Google Scholar]
- 10.Habbe N, Koorstra JB, Mendell JT, Offerhaus GJ, Ryu JK, Feldmann G, et al. MicroRNA miR-155 is a biomarker of early pancreatic neoplasia. Cancer Biol Ther. 2009;8:340–346. doi: 10.4161/cbt.8.4.7338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dillhoff M, Liu J, Frankel W, Croce C, Bloomston M. MicroRNA-21 is overexpressed in pancreatic cancer and a potential predictor of survival. J Gastrointest Surg. 2008;12:2171–2176. doi: 10.1007/s11605-008-0584-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Humeau M, Torrisani J, Cordelier P. miRNA in clinical practice: pancreatic cancer. Clin Biochem. 2013;46:933–936. doi: 10.1016/j.clinbiochem.2013.03.019. [DOI] [PubMed] [Google Scholar]
- 13.Lee EJ, Gusev Y, Jiang J, Nuovo GJ, Lerner MR, Frankel WL, et al. Expression profiling identifies microRNA signature in pancreatic cancer. Int J Cancer. 2007;120:1046–1054. doi: 10.1002/ijc.22394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Steele CW, Oien KA, McKay CJ, Jamieson NB. Clinical potential of microRNAs in pancreatic ductal adenocarcinoma. Pancreas. 2011;40:1165–1171. doi: 10.1097/MPA.0b013e3182218ffb. [DOI] [PubMed] [Google Scholar]
- 15.Zhang L, Jamaluddin MS, Weakley SM, Yao Q, Chen C. Roles and mechanisms of microRNAs in pancreatic cancer. World J Surg. 2011;35:1725–1731. doi: 10.1007/s00268-010-0952-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Panarelli NC, Chen YT, Zhou XK, Kitabayashi N, Yantiss RK. MicroRNA expression aids the preoperative diagnosis of pancreatic ductal adenocarcinoma. Pancreas. 2012;41:685–690. doi: 10.1097/MPA.0b013e318243a905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bloomston M, Frankel WL, Petrocca F, Volinia S, Alder H, Hagan JP, et al. MicroRNA expression patterns to differentiate pancreatic adenocarcinoma from normal pancreas and chronic pancreatitis. JAMA. 2007;297:1901–1908. doi: 10.1001/jama.297.17.1901. [DOI] [PubMed] [Google Scholar]
- 18.Samuel DO, Majid Mukhtar AA, Philip IO. A diagnostic pitfall: pancreatic tuberculosis, not pancreatic cancer. J Coll Physicians Surg Pak. 2013;23:211–213. [PubMed] [Google Scholar]
- 19.Sun GF, Zuo CJ, Shao CW, Wang JH, Zhang J. Focal autoimmune pancreatitis: radiological characteristics help to distinguish from pancreatic cancer. World J Gastroenterol. 2013;19:3634–3641. doi: 10.3748/wjg.v19.i23.3634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Matsumoto I, Shinzeki M, Toyama H, Asari S, Goto T, Yamada I, et al. A focal mass-forming autoimmune pancreatitis mimicking pancreatic cancer with obstruction of the main pancreatic duct. J Gastrointest Surg. 2011;15:2296–2298. doi: 10.1007/s11605-011-1543-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.van Gulik TM, Reeders JW, Bosma A, Moojen TM, Smits NJ, Allema JH, et al. Incidence and clinical findings of benign, inflammatory disease in patients resected for presumed pancreatic head cancer. Gastrointest Endosc. 1997;46:417–423. doi: 10.1016/s0016-5107(97)70034-8. [DOI] [PubMed] [Google Scholar]
- 22.Jiao LR, Frampton AE, Jacob J, Pellegrino L, Krell J, Giamas G, et al. MicroRNAs targeting oncogenes are down-regulated in pancreatic malignant transformation from benign tumors. PLoS One. 2012;7:e32068. doi: 10.1371/journal.pone.0032068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Singh P, Srinivasan R, Wig JD. Major molecular markers in pancreatic ductal adenocarcinoma and their roles in screening, diagnosis, prognosis, and treatment. Pancreas. 2011;40:644–652. doi: 10.1097/MPA.0b013e31821ff741. [DOI] [PubMed] [Google Scholar]
- 24.Toiyama Y, Hur K, Tanaka K, Inoue Y, Kusunoki M, Boland CR, et al. Serum miR-200c is a novel prognostic and metastasispredictive biomarker in patients with colorectal cancer. Ann Surg. 2014;259:735–743. doi: 10.1097/SLA.0b013e3182a6909d. [DOI] [PMC free article] [PubMed] [Google Scholar]