

Abstract
First, we sought to better understand the predisposition of novice female runners to injury by identifying potential differences in running mechanics and strength between experienced female runners and active novice runners. Secondly, we aimed to assess the relationship between hip and trunk strength with non-sagittal hip kinematics during running. Two female populations were recruited: 19 healthy experienced runners and 19 healthy active novice runners. Strength measurements of the hip abductors and external rotators were measured using a hand held dynamometer while trunk endurance was assessed via a side-plank. Next, an instrumented gait analysis was performed while each participant ran at 3.3 m/s. Group comparisons were made using an independent t-test to identify differences in the impact peak, loading rate, peak non-sagittal hip joint angles, trunk endurance, and hip strength. Pearson’s correlation coefficients were calculated between hip kinematics and strength measurements. There were no statistically significant differences in impact peak, loading rate, peak non-sagittal hip kinematics, or strength. However, the novice runners did show a clinically meaningful trend towards increased peak hip internal rotation by 3.8 degrees (effect size 0.520). A decrease in trunk side-plank endurance was associated with an increased peak hip internal rotation angle (r=−.357, p=0.03), whereas isometric strength was not related to kinematics. Programs aiming to prevent injuries in novice runners should target trunk performance and possibly hip neuromuscular control, rather than hip strength.
Keywords: hip strength, side-plank, impact peak, loading rate, non-sagittal hip kinematics
INTRODUCTION
Running is an increasingly popular form of exercise with over 50 million runners in the United States of America alone [1]. Unfortunately, up to 70% of these runners will develop an overuse injury within any one year period [2]. Of all groups, novice runners are especially at risk of developing an injury. Their injury rates have been reported to be higher than recreational, competitive, marathon, or cross-country runners [3]. Focusing on injury prevention among novice runners is important since getting an early injury may be a deterrent to maintaining an exercise program. However, there are few evidence based recommendations for healthy active people to follow who desire to start a running program.
Training errors are thought to contribute to a majority of running related injuries [4]. Specifically, increasing mileage too soon in the program may not allow the musculoskeletal system to adapt to the repetitive high-impact forces that accompany running [5]. To minimize the risk of injury, it has been suggested to limit increases in duration or intensity by no more than 10% a week [6]. However, a recent study has found that a graded running program in novice runners using the 10% rule was ineffective in reducing the rate of injury [7]. Sport participation history prior to starting a running program has also been associated with injury where participation in non-axial load sports (e.g. swimming, cycling) was a predictor of greater injury rates [8]. Although, preconditioning with exercises that induce axial-loading (e.g. walking and hopping) has been shown to have no influence on injury rates in novice runners [9]. If the rate of mileage increase and preconditioning does not reduce injury rates, then other potential modifiable risk factors, such as running mechanics and muscle strength, may have a role in the development of injuries in novice runners. However, the contribution of these factors has yet to be investigated in detail.
Running mechanics are increasingly recognized as an important contributing factor in the development of injuries. Specifically, increased peak tibial shock, impact peak, and vertical loading rates have been associated with tibial stress fractures [10]. Increased hip internal rotation and adduction joint angles have been linked to knee injuries [11, 12], where these joint angles tend to be more exaggerated in women [13]. Examples of altered mechanics seen in females during the stance phase of running include greater peak hip adduction and knee internal rotation with iliotibial band syndrome [11] and greater peak hip adduction and hip internal rotation with patellofemoral pain [12]. However, it remains unclear whether novice runners have these abnormal mechanics prior to starting a running program that may predispose them to injury.
Hip strength may also be related to running injuries. For example, injured legs in runners have been shown to demonstrate significantly weaker hip abductors and external rotator muscles [14, 15]. Specific to knee injuries, females with patellofemoral pain have demonstrated decreased hip abduction and external rotation strength by up to 26% and 36%, respectively [16, 17] while females with iliotibial band syndrome demonstrated weaker hip abductors by around 20% compared to the healthy limb and control participants [18]. These strength deficits are commonly used to explain the source of abnormal joint kinematics [17].
Mechanics and strength are typically measured together, where alterations in mechanics observed in injured participants are often explained using strength deficits. For example, decreased hip muscle strength observed in patellofemoral pain patients was proposed as a contributor to increased hip internal rotation [17]. Using musculoskeletal modeling, up to 40% muscle weakness can be tolerated before normal gait is impaired [19], suggesting that strength and mechanics may not be related. However, it is unclear if this extends to running. Hence the explicit relationship between isometric strength and kinematics warrants further investigation to determine if strength deficits can be used as an explanation for abnormal mechanics in novice runners.
Core dysfunction has been coupled with lower extremity injuries [20]. Females have exhibited decreased core endurance (as measured by the side-plank) compared to males, which has been proposed as a reason for a higher injury rates among females [14]. Whether novice female runners have a decreased trunk endurance that causes abnormal mechanics and places them at risk for injury remains unanswered.
The objectives of this study were twofold. First, we sought to better understand the predisposition of novice female runners to injury by identifying potential differences in running mechanics and strength between trained female runners and active novice runners. We expected active novice runner women to have a greater impact peak, a greater loading rate, higher peak hip adduction and internal rotation angles, weaker hip muscles, and decreased trunk endurance when compared with healthy experienced runners. Secondly, we aimed to assess the relationship between hip and trunk strength with non-sagittal hip kinematics during running. We expected increased non-sagittal joint angles to be associated with decreased strength [17].
METHODS
Two populations were recruited using flyers posted around the community: healthy experienced runners and healthy active novice runners. The experienced runners consisted of 19 females that had been consistently running at least 12 miles a week for the last year (average: 20.2 miles/week) (Table 1). The novice runner group consisted of 19 healthy active females who had not run for at least 5 years but reported a minimum of 5 out of 10 on the Tegner activity scale (Table 1). Participants were excluded if she had a previous injury within the last 6 months or any surgery of the lower extremity. Based on an a priori power analysis using GPower [21], 11 participants were required for each group to provide enough statistical power (β=0.8, α=0.05) to detect a large effect size (Cohen’s d of 0.5) as well as sufficiently power a two-tailed, independent t-test between groups. Each participant provided informed, written consent before involvement in the study. Data was collected following a protocol approved by the institutional review board at the University of Kentucky.
Table 1.
Subject demographics.
| Healthy Experienced runners | Healthy Active Novice runners | |
|---|---|---|
| Age (yrs) | 23 (3) | 24 (3) |
| Mass (kg) | 59.0 (6.5) | 60.5 (7.6) |
| Height (m) | 1.66 (0.06) | 1.66 (0.05) |
| Tegner | 6.6 (0.8) | 6.5 (1.6) |
Mean (SD).
Strength measurements of the hip abductors and external rotators were assessed for the right side of each participant using a hand held dynamometer (Lafayette Instruments, Lafayette, IN) and a stabilization strap via a previously established method [16]. For the hip abductors, the participant was placed in a side lying position and instructed to raise the upper leg toward the ceiling while pressing against a hand held dynamometer placed proximal to the tibiofemoral joint line. The external rotators were assessed in a sitting posture with the thigh stabilized and the participant instructed to push against the dynamometer placed on the inside of the leg superior to the ankle joint. For both strength tests, the participants were asked to increase how much they were pushing over three seconds and hold their maximum effort for the next two seconds. Each participant performed two practice trials and subsequently three testing trials. The maximum efforts reached during the testing trials were averaged for each participant. The raw force values were multiplied by femur length (the distance from the greater trochanter to the medial tibiofemoral joint line), normalized by mass, and multiplied by 100. Trunk strength was assessed by asking the participant to hold a side-plank (e.g. side-bridge) for as long as possible, up to two minutes (greater than the normative values obtained in healthy, young adults [14, 22]). The time at which the participant was no longer able to hold the correct position was recorded. The correct position consisted of holding oneself in a plane, propped on the elbow of the designated side with the opposite arm crossed at the chest. When two minutes was reached, the test ended.
Retroreflective markers were placed on the participant according to a previously established configuration consisting of anatomical landmarks and tracking clusters on the thighs, shanks, and heels [23]. The anatomical landmarks used were the L4–5 junction, iliac crests, anterior superior iliac spines, greater trochanters, femoral epicondyles, tibial plateaus, malleoli, as well as on the shoes at the first and fifth metatarsal heads. All participants wore the same type of running shoe, New Balance WR662 (New Balance, Brighton, MA, USA). Participants warmed up at a self-selected walking speed for five minutes on an instrumented treadmill (Bertec Corporation, Columbus, OH). Marker trajectories and force plate data were then recorded while the participant ran at 3.35 m/s (8 minute mile pace) for 2 minutes. Three-dimensional marker trajectories and force plate data were collected at 200 Hz using a 15 camera motion analysis system (Motion Analysis Corporation) and at 1200 Hz, respectively.
Visual 3D (C-motion, Germantown, MD, USA) was used to process the data. First, a fourth-order low-pass zero-lag Butterworth filter was used to filter the marker trajectories at 8 Hz and force plate data at 35 Hz. These cutoff frequencies were chosen from a residual analysis of the data [24]. Next, a functional hip joint center was calculated [25]. Finally, inverse kinematics was performed on a previously established biomechanical model [12] employing six degree-of-freedom joints. Hip angles were calculated using successive body fixed rotations of the order flexion-extension, ab-adduction, followed by internal-external rotation [26]. Custom LabView code (National Instruments, Austin, TX, USA) was subsequently utilized to extract the vertical impact peak, loading rate, and peak non-sagittal hip angles during stance. Consistent with other studies, loading rate was defined as the slope of the vertical ground reaction force between 20 to 80% of the time period between heel strike and the impact peak where heel strike was determined as the point when the vertical ground reaction force first reached 30 N [10, 27]. Data were collected from five trials for each participant and then averaged to give discrete variables.
Using SPSS (SPSS Inc., Chicago, IL), an independent t-test was used to assess group differences for the impact peak, loading rate, peak hip internal rotation during stance, peak hip adduction during stance, hip external rotator strength, and hip abductor strength. In conjunction with the t-test, the effect size, i.e. Cohen’s d, was determined using the equations of Portney and Watkins [28]. An effect size of greater than 0.5 was a moderate to large effect size [29] and deemed clinically meaningful. Given the number of subjects (19 per group), a post-hoc power analysis using GPower indicated the statistical analysis had enough power to detect an effect size of >0.38. Pearson’s correlation coefficients were also calculated in SPSS to assess the relationship between hip kinematics and strength measurements. P-values less that 0.05 were defined as statistically significant.
RESULTS
No significant differences were found between experienced runners and novice runners in impact peak, loading rate, non-sagittal hip kinematics, or strength (Table 2). The effect size of hip internal rotation was clinically meaningful where novice runners tended towards more internal rotation. Trunk side-plank endurance and hip internal rotation angle were significantly correlated with each other where an increase in endurance was associated with a decreased internal rotation angle (Figure 1). There was no significant correlation between hip abduction strength and adduction angle, hip rotation strength and rotation angle, or trunk side-plank endurance and adduction angle.
Table 2.
Comparison of loading characteristics, kinematics, and strength between experienced runners and novice runners.
| Variables | Experienced runner group |
Novice runner group |
Difference | p-value | Effect Size |
|---|---|---|---|---|---|
| Vertical impact peak (BW) | 1.60 (0.33) | 1.65 (0.37) | 0.05 (0.04) | 0.67 | 0.143 |
| Loading rate (BW/s) | 78.2 (25.0) | 73.1 (18.5) | 5.1 (6.5) | 0.48 | 0.232 |
| Hip adduction angle (deg) | 16.7 (3.4) | 15.4 (4.5) | 1.2 (1.2) | 0.34 | 0.326 |
| Hip internal rotation angle (deg) | 11.2 (7.4) | 15.0 (7.2) | 3.7 (0.2) | 0.12 | 0.520 |
| Right side-plank (sec) | 88 (25) | 76 (26) | 12 (1) | 0.09 | 0.470 |
| Right hip external rotation strength (Nm/kg) | 6.8 (1.9) | 6.4 (1.5) | 0.5 (0.4) | 0.44 | 0.234 |
| Right hip abduction strength (Nm/kg) | 15.5 (3.8) | 14.9 (3.7) | 0.6 (0.0) | 0.56 | 0.160 |
Significant p-values and effect sizes are bold and italicized. Mean (SD).
Figure 1.
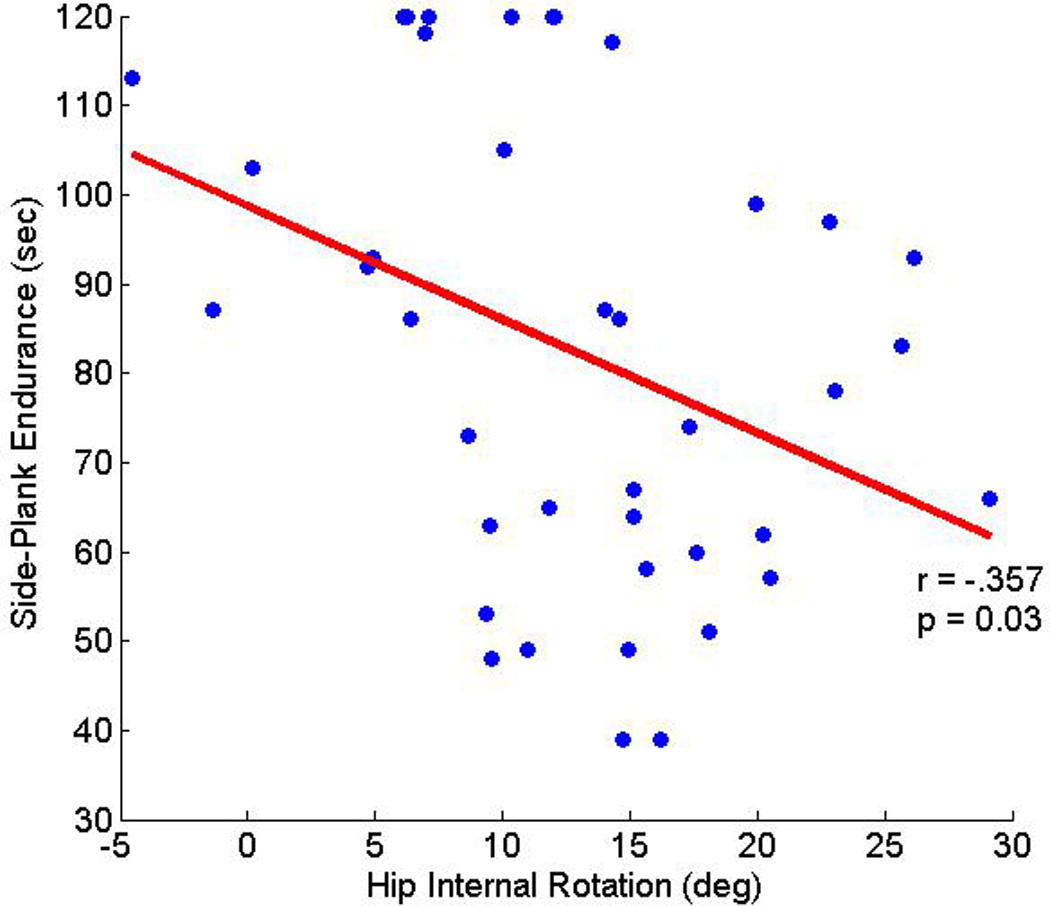
Side-plank endurance and hip internal rotation angle were significantly correlated.
DISCUSSION
The goals of this study were to compare running mechanics between experienced female runners and active novice runners, as well as investigate the relationship between strength and kinematics. There were three main findings: (1) the novice runners did show a trend towards increased peak hip internal rotation that was associated with a moderate effect size; (2) experienced runners and novice runners showed no differences in impact peak, loading rate, peak hip adduction angle during running, or differences in strength; (3) trunk side-plank endurance was associated with hip rotation whereas isometric hip strength was not associated with any kinematics. These results have implications for injury prevention programs and study design.
The novice runners did show a clinically meaningful trend towards increased peak hip internal rotation by 3.7 degrees. However, this difference did not achieve statistical significance. Quantifying both the effect size, which shows the size of group separation, and the p-value, which indicates the chance that the difference is due to chance alone, allowed us to more deeply explore the data. In this case, we believe that we were able to observe a large effect that was not statistically significant because the t-test was more sensitive to within group variability (7 degrees) than the calculation of the effect size. Historically, transverse plane motion has been recognized to be the most variable [30] but yet for clinicians is recognized to be one of the more important planes of motion to study for a variety of injuries (e.g. those with an ACL injury [31]). Thus, the 3.5 degree difference between experienced and novice runners, in our opinion, is of sufficient size that a clinician would intervene. Since there was no correlation between isometric strength and joint angles, this kinematic change may reflect a lack of control in the novice runners or increased control in the experienced runners. Thus, a possible target for injury prevention programs in novice, female runners may be hip control rather than strengthening exercises. Future experiments could test the feasibility of using a preconditioning program with these exercises to decrease peak hip internal rotation angles in novice runners.
There were no significant differences in impact peak, loading rate, peak hip adduction angle during running, hip strength, or trunk endurance between trained and novice runners. Although these results do not provide insight into why novice runners have increased injury rates, they do eliminate possible factors. Other variables such as muscle electromyography, joint torques, and power should be the focus of future work in novice runners. Given that no strength differences were observed between these groups, using electromyography to elucidate control mechanisms in novice runners seems particularly relevant. Our results may also help studies in their choice of participant populations. Studies investigating running mechanics need not be restricted to just experienced runners, which may help with participant enrollment. Findings across studies that included or excluded runners based on activity level may be also reasonably compared.
Hip strength and mechanics are commonly assessed together. For example, decreased isometric hip strength and increased hip internal rotation angle have been concurrently observed in patellofemoral pain patients [17]. However, in our results we found a moderate relationship between trunk endurance (i.e. side-plank test) and hip axial rotation, not isometric hip strength and kinematics. This agrees with work by Souza et. al. who also found no relationship between isometric external rotational strength and hip internal rotation angle during running [32]. Interestingly, the relationship between side-plank performance and hip internal rotation could be due in part to the strong contribution from gluteus medius to the side-plank test [33]. The gluteus medius is believed to serve as an external rotator as the hip moves from a flexed to an extended position, as one would see during the stance phase of running and as evidenced by a modeling study that found 3 out of the 4 compartments of the gluteus medius have an external rotation moment arm as the hip approaches a neutral position [34]. Thus, while we are unable to completely separate out the contributions of the trunk and hip musculature from the side-plank results, there appears to be at least a theoretical argument for the contribution of gluteus medius endurance to running performance. These results seem to imply control and/or endurance of the gluteus medius rather than isometric strength may be more relevant to consider when investigating running. This extends the findings of a musculoskeletal modeling study that explored the robustness of walking to isometric muscle strength and found that up to 40% weakness can be tolerated [19]. Results of other studies in the literature also support strength and endurance testing that includes control, rather than just isometric strength. For example, muscle weakness in patellofemoral pain participants did not correspond with expected alterations in hip axial rotation and ab-adduction, which supports our findings that isometric muscle strength and kinematics are unrelated [35]. In promotion of motor control testing isokinetic hip strength (which involves elements of both control and strength) has been found to be moderately associated with trunk mechanics during running [36]. A study on preconditioning found a clinically meaningful increase in range of motion for hip axial rotation following a routine designed to increase volitional control of the hip and core muscles using plyometric exercises (e.g. abdominal draw-ins, side-lying straight-leg raises, etc) [37]. Future work could investigate how performance on plyometric exercises relates to mechanics in injured populations and which exercises are the most relevant to measure during a clinical assessment.
There are a few limitations and study design factors to consider in the interpretation of our results. First, the type of activity was not standardized in the screening of active individuals, which may cause large variability in the strength measurements. For example, some active individuals participated in weightlifting while others used a bicycle or elliptical machine as a primary means of exercise. Second, our study only considered active individuals. We would expect to see greater differences in mechanics between inactive and active individuals. However, future studies are needed to confirm this. Third, we only considered females since running mechanics have been shown to vary between sexes [13]. Fourth, the side-plank test was limited to two minutes. However, this limit was only achieved in 2 novice runners and 4 experienced runners, making it unlikely that this affected the results.
CONCLUSION
In conclusion, the novice runners did show a trend towards increased peak hip internal rotation that may be clinically meaningful but no differences in loading, strength, or peak hip adduction angle during running. There was a significant correlation between trunk endurance and hip internal rotation angle, indicating that decreased trunk endurance may lead to running related injuries. Injury prevention programs should target trunk performance and possibly hip neuromuscular control, rather than hip strength.
ACKNOWEDGEMENTS
This work was partially funded by the Division of Information and Intelligent Systems of the National Science Foundation, grant 1231545. Funding support was also provided by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under award number K23AR062069. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
CONFLICTS OF INTEREST
There are no conflicts of interest to disclose.
REFERENCES
- 1.USA, R. 2012 State of the Sport Part II: Running Industry Report. 2012:2013. [Google Scholar]
- 2.Hreljac A. Impact and overuse injuries in runners. Med Sci Sports Ex. 2004;36:845–849. doi: 10.1249/01.mss.0000126803.66636.dd. [DOI] [PubMed] [Google Scholar]
- 3.Tonoli C, Cumps E, Aerts I, Verhagen E, Meeusen R. Running related injuries in long-distance running: Incidence, risk factors and prevention. Sport en Geneeskunde. 2010;43:12. [Google Scholar]
- 4.Fields KB, Sykes JC, Walker KM, Jackson JC. Prevention of running injuries. Curr Sports Med Rep. 2010;9:176–182. doi: 10.1249/JSR.0b013e3181de7ec5. [DOI] [PubMed] [Google Scholar]
- 5.Hreljac A. Etiology, prevention, and early intervention of overuse injuries in runners: a biomechanical perspective. Phys Med Rehabil Clin N Am. 2005;16:651–667. doi: 10.1016/j.pmr.2005.02.002. [DOI] [PubMed] [Google Scholar]
- 6.Johnston C, Taunton J, Lloyd-Smith D, McKenzie D. Preventing running injuries. Practical approach for family doctors. Can Fam Phys. 2003;49:1101–1109. [PMC free article] [PubMed] [Google Scholar]
- 7.Buist I, Bredeweg SW, van Mechelen W, Lemmink KAPM, Pepping G-J, Diercks RL. No Effect of a Graded Training Program on the Number of Running-Related Injuries in Novice Runners: A Randomized Controlled Trial. Am J Sports Med. 2008;36:33–39. doi: 10.1177/0363546507307505. [DOI] [PubMed] [Google Scholar]
- 8.Buist I, Bredeweg SW, Lemmink KAPM, van Mechelen W, Diercks RL. Predictors of Running-Related Injuries in Novice Runners Enrolled in a Systematic Training Program: A Prospective Cohort Study. Am J Sports Med. 2010;38:273–280. doi: 10.1177/0363546509347985. [DOI] [PubMed] [Google Scholar]
- 9.Bredeweg SW, Zijlstra S, Bessem B, Buist I. The effectiveness of a preconditioning programme on preventing running-related injuries in novice runners: a randomised controlled trial. Br J Sports Med. 2012;46:865–870. doi: 10.1136/bjsports-2012-091397. [DOI] [PubMed] [Google Scholar]
- 10.Milner CE, Ferber R, Pollard CD, Hamill J, Davis IS. Biomechanical factors associated with tibial stress fracture in female runners. Med Sci Sports Ex. 2006;38:323–328. doi: 10.1249/01.mss.0000183477.75808.92. [DOI] [PubMed] [Google Scholar]
- 11.Noehren B, Davis I, Hamill J. ASB clinical biomechanics award winner 2006 prospective study of the biomechanical factors associated with iliotibial band syndrome. Clin Biomech (Bristol, Avon) 2007;22:951–956. doi: 10.1016/j.clinbiomech.2007.07.001. [DOI] [PubMed] [Google Scholar]
- 12.Noehren B, Pohl MB, Sanchez Z, Cunningham T, Lattermann C. Proximal and distal kinematics in female runners with patellofemoral pain. Clin Biomech. 2012;27:366–371. doi: 10.1016/j.clinbiomech.2011.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ferber R, McClay Davis I, Williams IiiDS. Gender differences in lower extremity mechanics during running. Clin Biomech. 2003;18:350–357. doi: 10.1016/s0268-0033(03)00025-1. [DOI] [PubMed] [Google Scholar]
- 14.Leetun DT, Ireland ML, Willson JD, Ballantyne BT, Davis IM. Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sports Ex. 2004;36:926–934. doi: 10.1249/01.mss.0000128145.75199.c3. [DOI] [PubMed] [Google Scholar]
- 15.Niemuth PE, Johnson RJ, Myers MJ, Thieman TJ. Hip muscle weakness and overuse injuries in recreational runners. Clin J Sports Med. 2005;15:14–21. doi: 10.1097/00042752-200501000-00004. [DOI] [PubMed] [Google Scholar]
- 16.Ireland ML, Willson JD, Ballantyne BT, Davis IM. Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 2003;33:671–676. doi: 10.2519/jospt.2003.33.11.671. [DOI] [PubMed] [Google Scholar]
- 17.Souza RB, Powers CM. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J Orthop Sports Phys Ther. 2009;39:12–19. doi: 10.2519/jospt.2009.2885. [DOI] [PubMed] [Google Scholar]
- 18.Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA. Hip abductor weakness in distance runners with iliotibial band syndrome. Clin J Sports Med. 2000;10:169–175. doi: 10.1097/00042752-200007000-00004. [DOI] [PubMed] [Google Scholar]
- 19.van der Krogt MM, Delp SL, Schwartz MH. How robust is human gait to muscle weakness? Gait & Posture. 2012;36:113–119. doi: 10.1016/j.gaitpost.2012.01.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chuter VH, Janse de Jonge XAK. Proximal and distal contributions to lower extremity injury: A review of the literature. Gait & Posture. 2012;36:7–15. doi: 10.1016/j.gaitpost.2012.02.001. [DOI] [PubMed] [Google Scholar]
- 21.Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Beh Res Meth. 2007;39:175–191. doi: 10.3758/bf03193146. [DOI] [PubMed] [Google Scholar]
- 22.McGill SM, Childs A, Liebenson C. Endurance times for low back stabilization exercises: clinical targets for testing and training from a normal database. Arch Phys Med Rehabil. 1999;80:941–944. doi: 10.1016/s0003-9993(99)90087-4. [DOI] [PubMed] [Google Scholar]
- 23.Noehren B, Sanchez Z, Cunningham T, McKeon PO. The effect of pain on hip and knee kinematics during running in females with chronic patellofemoral pain. Gait & Posture. 2012;36:596–599. doi: 10.1016/j.gaitpost.2012.05.023. [DOI] [PubMed] [Google Scholar]
- 24.Winter DA. Biomechanics and motor control of human movement. 2009 [Google Scholar]
- 25.Schwartz MH, Rozumalski A. A new method for estimating joint parameters from motion data. J Biomech. 2005;38:107–116. doi: 10.1016/j.jbiomech.2004.03.009. [DOI] [PubMed] [Google Scholar]
- 26.Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Engr. 1983;105:136–144. doi: 10.1115/1.3138397. [DOI] [PubMed] [Google Scholar]
- 27.Mündermann A, Dyrby CO, Andriacchi TP. Secondary gait changes in patients with medial compartment knee osteoarthritis: increased load at the ankle, knee, and hip during walking. Arth & Rheum. 2005;52:2835–2844. doi: 10.1002/art.21262. [DOI] [PubMed] [Google Scholar]
- 28.Portney LG, Watkins MP. Foundations of clinical research. 1993 [Google Scholar]
- 29.Cohen J. Statistical power analysis for the behavioral sciences. 1988;567 [Google Scholar]
- 30.Schwartz MH, Trost JP, Wervey RA. Measurement and management of errors in quantitative gait data. Gait & Posture. 2004;20:196–203. doi: 10.1016/j.gaitpost.2003.09.011. [DOI] [PubMed] [Google Scholar]
- 31.Andriacchi TP, Mundermann A, Smith RL, Alexander EJ, Dyrby CO, Koo S. A framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann Biomed Eng. 2004;32:447–457. doi: 10.1023/b:abme.0000017541.82498.37. [DOI] [PubMed] [Google Scholar]
- 32.Souza RB, Powers CM. Predictors of Hip Internal Rotation During Running: An Evaluation of Hip Strength and Femoral Structure in Women With and Without Patellofemoral Pain. Am J Sports Med. 2009;37:579–587. doi: 10.1177/0363546508326711. [DOI] [PubMed] [Google Scholar]
- 33.Ekstrom R, Donatelli R, Carp K. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. 2007;37:754. doi: 10.2519/jospt.2007.2471. [DOI] [PubMed] [Google Scholar]
- 34.Delp SL, Hess WE, Hungerford DS, Jones LC. Variation of rotation moment arms with hip flexion. Journal of biomechanics. 1999;32:493–501. doi: 10.1016/s0021-9290(99)00032-9. [DOI] [PubMed] [Google Scholar]
- 35.Bazett-Jones DM, Cobb SC, Huddleston WE, O'Connor KM, Armstrong BS, Earl-Boehm JE. Effect of patellofemoral pain on strength and mechanics after an exhaustive run. Med Sci Sports Ex. 2013;45:1331–1339. doi: 10.1249/MSS.0b013e3182880019. [DOI] [PubMed] [Google Scholar]
- 36.Ford KR, Taylor-Haas J, Genthe K, Hugentobler J. Relationship between Hip Strength and Trunk Motion in College Cross-Country Runners. Med Sci Sports Ex. 2013;45:1125–1130. doi: 10.1249/MSS.0b013e3182825aca. [DOI] [PubMed] [Google Scholar]
- 37.Earl JE, Hoch AZ. A proximal strengthening program improves pain, function, and biomechanics in women with patellofemoral pain syndrome. Am J Sports Med. 2011;39:154–163. doi: 10.1177/0363546510379967. [DOI] [PubMed] [Google Scholar]