

Abstract
The lack of health human resources is a global issue. China also faces the same issue, in addition to the equity of human resources allocation. With the launch of new healthcare reform of China in 2009, have the issues been improved? Relevant data from China Health Statistical Yearbook and a qualitative study show that the unequal allocation of health human resources is getting worse than before.
Keywords: Equality, China, Health Human Resources, Rural Area, Urban Area
In 2009, the new round of health reform in China confirmed political and financial supports towards universal and equitable health coverage by 2020 (1). Expanding health insurance universal coverage to more than 90% of the population, establishing a national essential medicines system to meet everyone’s primary needs of healthcare, improving primary care delivery system to provide basic healthcare and to manage referrals to specialist care and hospitals, making public health services available and equal for all, and piloting public hospital reforms are the main five objectives in the reform (2). That how well the reform worked in the past 5 years has become a curious issue in China and in the world. Has the investment improved the distribution of health human resources, especially in the rural area? “All people, everywhere, shall have access to a skilled, motivated and facilitated health worker within a robust health system” (3). Of the three major resources (financial, physical, and human), human resources for health was considered as the least mapped and analyzed in China (4). The main element of a health system is human resources (5). The impacts of health workforce mobility by health system reform brought to the front globally in Africa (6), America (7), and all over the world. It is reported that the whole world is short of 7.2 million healthcare workers by 2013, and the figure will reach at 12.9 by 2035 (8). However, there is few studies about Chinese human resources. A latest review about equity of Chinese health workforce was reported in 2008 (4). It is found that the inequality in the distribution of both doctors and nurses is very high, with most of this inequality accounted for by within-province inequalities rather than by between-province. Another study estimated that China would need 12.88 million human resources for health by 2020 (9).
What is the actual achievements of the reform on health workforce equity from 2009? Do the main measurements contribute positive or negative influence on China’s health workforce? In order to find the answers for these questions, we collected relevant data from China Health Statistical Yearbook and made a qualitative study in a province.
From year 2003 to 2012, the gap in medical and technical personnel per 1,000 population between urban and rural areas has become bigger and bigger (Figure 1). After the new round reform in 2009, the gap has become even bigger than before (Figure 1). Why the new round health system reform does not narrow the gap? After a deep discussion with local health authorities; a discussion with directors, physician at primary, secondary and tertiary hospitals; we found several so-called health system reform policies have negatively affected on it.
Figure 1 .
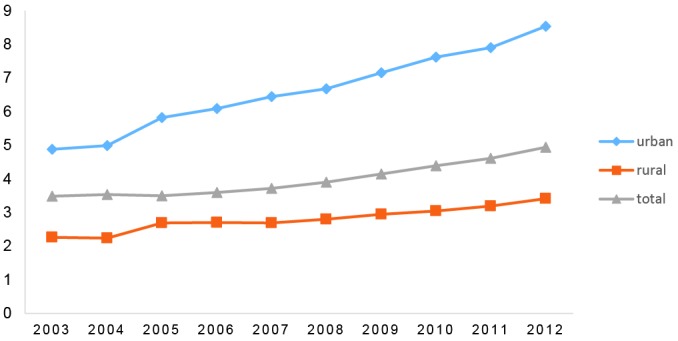
Number of medical and technical personnel per 1,000 population Note: As indicated by the China Health Statistic Book, when urban area is comparing with the rural area, the denominator of number of medical and technical personnel per 1,000 population is the permanent resident population instead of census registered population.
The aim of establishing national essential drugs programs to improve the primary care delivery system to provide basic and necessary healthcare. However, in China, the basic health facilities are only allowed to use the essential drugs, thus results in the inconsistency of drugs available between tertiary, secondary hospitals and primary health institutions (basic health facilities) because the tertiary and secondary hospitals which are usually located in urban areas are allowed to use essential drugs and also other drugs, further reduces the clinical capacity in the basic health facilities, makes patients move to a big hospital. It also leads to a fall in physician’s income (10). Physicians rely on patients to hone their skills, especially for those who have a dream of future career development, thus the essential drugs program has deteriorated the stability of health human resources in basic health facilities.
The package of basic public health services is a good measure to improve the public health services in urban and rural areas. However, while governments emphases the importance of the package, neglects the importance of the basic medical services in the basic health facilities to a certain degree, thus making physicians change jobs or moving to a hospital. “…Equal attention should be paid to both of public health and medical care, but... medical services began to be weaken, our community medical service is degenerating”. “Public health services and clinical services cannot be completely separated. Existing community health resources is limited, if we have to bear the public health workload, it will inevitably lead to the atrophy of clinical service”. Physicians in the basic health facilities said. Actually, most primary health workers hold a relatively negative attitude toward the growing workload on public health services (11).
The payment mechanism for health providers has been changed also. The global payment budget for a basic health facilities is previously decided. The payment includes a basic salary and a bonus which is based on so-called performance (1). This change has also made a negative contribution on clinical services because the total payment budget in a facility cannot be broken and the size of bonus is small, people worked more cannot get more pay. Thus, no one wants to work hard, resulting in a lazy (10). This kind of reform further makes clinician switch to hospitals where they can earn more by better performance.
Ethical issues
Not applicable.
Competing interests
Authors declare that they have no competing interests.
Authors’ contributions
HD and QY conceptualized and designed the study and collected the data. QY made the data analysis and drafted the manuscript. HD and QY finalised and approved the manuscript.
Citation: Yang Q, Dong H. Have health human resources become more equal between rural and urban areas after the new reform? Int J Health Policy Manag 2014; 3: 359–360. doi: 10.15171/ijhpm.2014.129
References
- 1.Yip WC, Hsiao WC, Chen W, Hu S, Ma J, Maynard A. Early appraisal of China’s huge and complex health-care reforms. Lancet. 2012;379:833–42. doi: 10.1016/s0140-6736(11)61880-1. [DOI] [PubMed] [Google Scholar]
- 2. People’s Republic of China. Current major project on health care system reform (2009–2011) [database on the Internet]. 2009. [cited 2014 November 6]. Available from:http://www.gov.cn/zwgk/2009-04/07/content_1279256.htm.
- 3.Cometto G, Boerma T, Campbell J, Dare L, Evans T. The Third Global Forum: framing the health workforce agenda for universal health coverage. Lancet Glob Health. 2013;1:1324–5. doi: 10.1016/s2214-109x(13)70082-2. [DOI] [PubMed] [Google Scholar]
- 4.Anand S, Fan VY, Zhang J, Zhang L, Ke Y, Dong Z. et al. China’s human resources for health: quantity, quality, and distribution. Lancet. 2008;372:1774–81. doi: 10.1016/s0140-6736(08)61363-x. [DOI] [PubMed] [Google Scholar]
- 5.Sheikh K, Ranson MK, Gilson L. Explorations on people centredness in health systems. Health Policy Plan. 2014;29:ii1–5. doi: 10.1093/heapol/czu082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Crisp N, Gawanas B, Sharp I. Training the health workforce: scaling up, saving lives. Lancet. 2008;371:689–91. doi: 10.1016/s0140-6736(08)60309-8. [DOI] [PubMed] [Google Scholar]
- 7.Márquez M. Health-workforce development in the Cuban health system. Lancet. 2009;374:1574–5. doi: 10.1016/s0140-6736(09)61919-x. [DOI] [PubMed] [Google Scholar]
- 8.Tucker C. WHO: Global health worker shortage to have major impact in next decades. The Nation’s Health. 2014;44:15. [Google Scholar]
- 9.Zhang G. [Analysis and forecasting on the demand for health human resources in China] Chinese Jouranl of Health Policy. 2011;4:1–5. [in Chinese]. [Google Scholar]
- 10.Zhou XD, Li L, Hesketh T. Health system reform in rural China: Voices of healthworkers and service-users. Soc Sci Med. 2014;117:134–41. doi: 10.1016/j.socscimed.2014.07.040. [DOI] [PubMed] [Google Scholar]
- 11. Yang Q. The problem and strategy of fist diagnosis in community: psychological study based on grass-roots health workers in urban and rural areas of Zhejiang Province. Symposium of grass-roots health reform in East China; 2014; Hangzhou. [in Chinese].